Apocrine Hidrocystoma- A Histological Diagnosis
An Asian female in her 20s, presented with a painless swelling in the left upper eyelid for 2 years. A cystic, non-tender, well defined swelling of 3 by 4 mm with a punctum was seen in the medial aspect of left upper eyelid. Best corrected visual acuity was 20/20 in both eyes, with anterior and posterior segment examination within normal limits in both eyes. Provisional diagnosis of Sebaceous cyst was made, excision of cyst was planned for cosmetic indication. Cyst removal in toto was done and sent for histopathological examination. HPE report was awaited and came the surprise report - APOCRINE HIDROCYSTOMA, a rare, benign, cystic tumor of the apocrine sweat glands. Since surgical excision is the treatment option for apocrine hidrocystoma, patient was informed of the same and reassured. The diagnosis is histological and hence apocrine hidrocystoma must be kept in mind while considering differential diagnosis of cystic lesions in ocular adnexa.
Introduction
Cystic swellings in ocular adnexa have varied differential diagnosis. Though clinically it appeared as a slow growing asymptomatic well circumscribed lesion with punctum mimicking a sebaceous cyst, only on histological evaluation after surgical excision was a diagnosis of Apocrine hidrocystoma made. Hence an additional differential diagnosis of apocrine hidrocystoma must be kept in mind in cystic swellings in ocular adnexa.
Case Presentation
An Asian female in her 20s, presented with a painless swelling in the left upper eyelid for 2 years. A cystic, non- tender, well defined swelling of 3 by 4 mm, with mild skin pigmentation and a punctum was seen in the medial aspect of left upper eyelid (Figure 1). Best corrected visual acuity was 20/20 in both eyes, with anterior and posterior segment examination within normal limits in both eyes. Provisional diagnosis of Sebaceous cyst was made, excision of cyst was planned for cosmetic indication. Cyst removal in toto was done (Figure 2) and sent for histopathological examination. HPE report was awaited and came the surprise report Multiloculated cyst lined by columnar to cuboidal epithelium, with apocrine snouts enclosing keratinous material (Figure 3 & 4) - Apocrine Hidrocystoma.


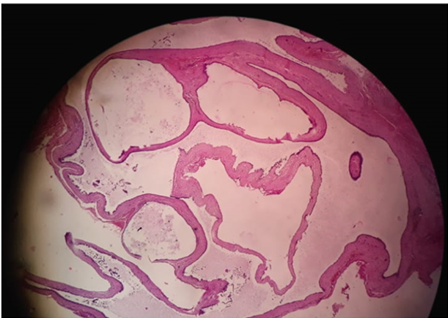
- Specimen showed an encapsulated solid lesion, multilocular cystic space with fibrous tissue lined by stratified epithelium.
- In the cystic lumen, proteinaceous fluid was present (haematoxylin and eosin).
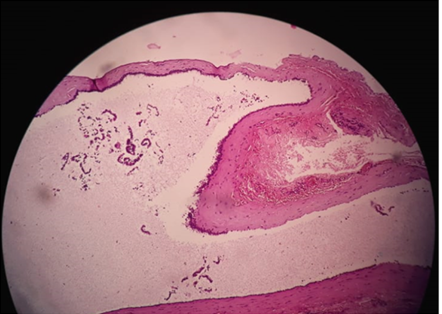
- Cystic wall composed of a stratified apocrine secretory epithelium consisting of epithelial sweat duct like lining.
- Rows of secretory cells showing decapitation secretion characterized by apocrine snouts and fringes are clearly recognizable (haematoxylin and eosin).
Treatment and Outcome
Surgical excision with narrow margin was done ad specimen sent for histopathological evaluation as a standard procedure. Patient had good cosmetic correction after the procedure with minimal scar along the skin crease on 1 month follow up. There was no recurrence of lesion or similar lesion elsewhere in head and neck area.
Discussion
Apocrine hidrocystoma– a rare, benign, cystic tumor of the apocrine sweat glands [1]. Estimated incidence is 1/1000 of cutaneous biopsies; the true value remains unknown and underestimated since many a times apocrine hidrocystomas seen in ophthalmology or surgery clinics are diagnosed as Moll’s gland cysts or sebaceous cysts [2]. Mostly seen in head and neck area affecting cheek and inner canthus of eye, as solitary asymptomatic papule or macule, may be seen in other areas as well. Multiple cysts are also documented and may be associated with rare inherited ectodermal dysplasias - Goltz-Gorlin syndrome and Schopf- Schultz-Passarge syndrome [1]. Seen in adults 30 to 70 years of age.No specific geographic predilection and no familial inheritance [1]. Presents as slow growing, solitary, dome shaped, well delineated cystic nodule. Blue, bluish black or brown in color of size 3 to 15 mm, giant apocrine hidrocystomas more than 20 mm are also documented. Derived from secretory part of apocrine sweat glands, with cystic proliferation and is not a simple retention cyst seen intradermally. Differential diagnosis includes: Sebaceous cyst, Lipoma, Eccrine hidrocystoma, Cystic epithelioma. Microscopic examination shows multilocular spaces with a sweat-duct-like epithelium with monomorphous cubic cells. Cyst wall is covered by apocrine-type epithelial cells with marked decapitation secretion identified by apocrine snouts. A pathognomonic sign is the presence of large columnar or cuboidal cells in the composition of the epithelial lining showing a decapitation secretion, usually associated with an outer layer of flat myoepithelial Cells.
Several treatment options have been documented including. Surgical excision with narrow margins, Simple needle puncture, Application of anticholinergic creams, Trichloroacetic acid injection, Hypertonic saline sclerotherapy [1] No malignant transformation of apocrine hidrocystoma has been reported to date.Histopathologic analysis is mandatory to obtain a final diagnosis due to its peculiar aspects.
Learning points- Mostly encountered by Dermatologists and Surgeons, this lesion presenting to an Ophthalmologist was indeed a Cyst with a twist Histopathologic analysis is mandatory to obtain a final diagnosis in all cases Rare, slow growing, benign, aysmptomatic cysts are an esthetic burden and psychological distress in patients and hence need to be diagnosed with caution [3, 4].
References
-
Hafsi W, Badri T, Farhan S (2019) Apocrine Hidrocystoma. StatPearls, Treasure Island (FL), StatPearls Publishing.
-
Poli PP, Creminelli L, Moramarco V, Gobbo AD, Ferrante F, et al. (2017) Diagnostic Workup and Treatment of a Rare Apocrine Hidrocystoma Affecting the Oral Mucosa: A Clinical and Histological Case Report. Case Reports in Dentistry 2017: 9382812.
-
Bordelon JR, Tang N, Elston D, Niedt G, Strugar TL (2017) Multiple apocrine hidrocystomas successfully treated with botulinum toxin A. British Journal of Dermatology 176(2): 488-490.
-
Verma SB (2010) Multiple apocrine hidrocystomas: a confusing clinical diagnosis. An Bras Dermatol 85(2): 260-263.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report