A Review of Rift Valley Fever: Its Epidemiology and Economic Impact on Livestock
Rift Valley fever is a significant zoonotic disease transmitted by mosquitoes, affecting domestic ruminants and occasionally humans, with substantial economic implications. This review highlights the epidemiology and economic impacts of RVF, emphasizing its emergence beyond traditional endemic regions, notably in recent outbreaks across Africa and the Middle East. RVF outbreaks are closely linked to climatic factors such as heavy rainfall and flooding, facilitating mosquito vector proliferation. While primarily transmitted by mosquitoes, the virus exhibits a complex multispecies epidemiology involving various hosts and vectors. The diversity of host and vector species present, as well as climate change, has resulted in outbreaks in previously unreported areas. However, in Ethiopia, the occurrence of the disease was reported, but clinical Rift Valley fever has never been detected or reported yet. Outbreaks lead to livestock market closures, trade restrictions, and substantial economic losses, particularly in countries heavily reliant on livestock trade. Vaccination, vector control, and movement restrictions are crucial for disease prevention and control. Understanding RVF's complex epidemiology and implementing effective surveillance and control measures are essential for mitigating its impact on both livestock and human populations. Collaboration between endemic countries and their trading partners is vital for managing the disease and ensuring food security.
Abbreviations
RVF: Rift Valley Fever Virus; WHO: World Health Organization.
Introduction
Rift Valley fever is a zoonotic, an emerging mosquito- borne viral disease important in domesticated ruminants. It is caused by the RVF virus, a member of the Phlebovirus genus of the Phenuiviridae family [1]. RVF was first reported in 1930 as massive abortion and necrotic hepatitis in sheep in Kenya [2]. It has since been reported in most countries in South and East Africa [3]. Massive RVF outbreaks occurred in East Africa in the years 1997–1998 and 2006–2007, both of which were accompanied by heavy rains and widespread floods and caused livestock owners to suffer significant financial losses [4].
Currently Most African countries are endemic to the RVFV and have experienced infrequent outbreaks, usually after heavy rainfall. Outside of Africa, the epidemics were recognized in 1979 in Madagascar [3]; in 2000, Saudi Arabia
and Yemen [5]. More recently several African countries reported between 2020 and 2023, including Burundi, Algeria, Uganda, Niger, Libya, Mauritania, Senegal, Sudan, Kenya, and Madagascar [6, 7, 8, 9]. The spread of RVFV outside its endemic region raises concerns about the potential threat of new geographic areas [3].
The Rift valley fever virus can affects domestic ruminants such as sheep, goats, cattle, and camels, causing high abortion rates and sudden infant deaths. It has also been found in humans and wild wildlife, causing mild illness [10]. Mosquitoes, especially those of the Aedes and Culex genera, are the principal means of transmission [11]. The virus appears to survive in the dried eggs of Aedes mosquitoes, and epidemics are associated with the hatching of eggs during years of heavy rainfall and localized flooding [12]. RVFV can also be transmitted by other vectors, including many mosquito species and possibly other biting insects such as ticks and midges. The Rift Valley Fever virus has a complex, multispecies epidemiology [13]. A host’s transmission of RVF depends on its vector capacity, infection susceptibility, and favourable ecological and climatic conditions for mosquito survival and reproduction [14]. Exposure to competent mosquito vectors is a significant risk factor for humans and animals, especially among livestock handlers [2].
Rift Valley Fever has a significant economic impact including high mortality rates among young animals and abortion rates among livestock [15]. It not only affects animal and human health, but economic impacts of the disease may include impacts of disease occurrence and its management associated with quarantine restrictions, bans on the movement of livestock, the cost of surveillance and control interventions, and the collapse of demand for products due to public perceptions of risk [16]. Understanding the nature and epidemiology of Rift Valley Fever is crucial to understanding how to prevent and control the disease. Therefore, the objectives of this paper are to review on epidemiology and economic impacts of Rift valley fever disease related to live- stocks.
Literature Review
Etiology of Rift Valley Fever
Rift Valley Fever virus (RVFV) is a spherical enveloped RNA virus from the Phenuiviridae family (formerly Bunyaviridae) of the genus Phlebovirus that causes Rift Valley Fever [1]. It has an 80–120 nm diameter and consists of three segments, short (S), medium (M), and large (L), that make up the virus genome, which is a tripartite RNA [17]. The L segments are encoded by viral RNA-dependent RNA polymerase. The M segment also codes for non-structural proteins (NSm) and the two envelope glycoproteins, Gn and Gc. Nucleoproteins (N) and second non-structural proteins (NSs) are both encoded by the S segment, as illustrated in Figure 1 [18].
The virus is resistant in alkaline environments but inactivated at pH 6.8, with an ideal pH range of 7-8. At neutral or alkaline pH, particularly in the presence of protein material such as serum, the virus can remain viable for up to 4 months at 4°C and for 8 years when stored below 0°C (32°F). Under optimal conditions, the RVF virus remained viable in aerosols for more than an hour at 23°C and 50–80% relative humidity. Due to a lipid bilayer in the virion envelope, the virus is susceptible to lipid solvents (sodium or calcium hypochlorite and acetic acid) [19].
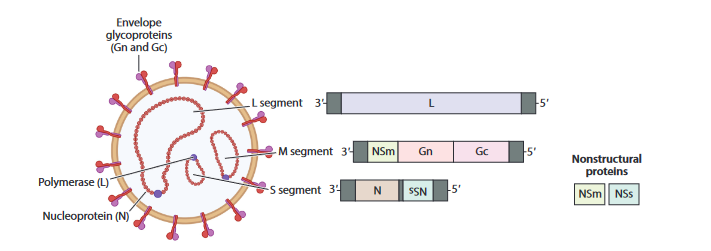
Source: [20]. Figure 1: Genomic organization of Rift valley fever virus.
Epidemiology
Host susceptibility: Natural hosts for RVFvirus include mosquitoes, sheep, goats, cattle, camels, and other ruminants [1]. The disease also affects humans, pets, and wildlife. Domestic ruminants (sheep, cattle, and goats) have experienced significant mortality and morbidity from RVF infection (Table 1) [21]. Wild life, including African buffalo, black rhinoceros, kudu, impala, African elephants, and various monkey species, are reservoirs for the virus during inter-epidemic periods and play a role in amplifying the virus during epizootics [22]. A lot of wild rodent species are susceptible to RVF, but their epidemiological significance in virus maintenance and transmission is not known [19, 23, 24, 25].
| Severe illness mortality >70% | Severe illness mortality20-70% | Moderate illness Mortality5-20% | Resistant to infection | Non susceptible | References | |
|---|---|---|---|---|---|---|
| Lambs | Sheep | Cattle | Dog | Avian | ||
| Kids | Calves | Goat | Cats | Reptilian | ||
| Puppies | Buffaloes | Equine | ||||
| Kittens | Camels | Pig | [19,24,25] | |||
| Mice | Humans | Guina pig | ||||
| Baby hamsters | Monkey |
Table 1: Rift valley Fever virus host range and disease severity.
Distribution and Occurrence of Rift Valley Fever: Rift Valley Fever was first reported in 1930 during outbreak of sheep in Rift valley of Kenya [2]. The illness has been linked to both humans and a number of different animal species [7, 9]. The disease was next discovered in South Africa between 1950 and 1951, where it caused significant sheep and bovine epizootics, catastrophic losses, and human cases [26]. Massive RVF outbreaks occurred in East Africa in the years 1997–1998 and 2006–2007, both of which were accompanied by heavy rains and widespread floods and caused livestock owners to suffer significant financial losses. It is documented as the most devastating outbreak in East Africa (Figure 2) [27]. In more recent times, epidemics have occurred in the majority of sub-Saharan countries, including West Africa, and have since 2010 extended to the Middle East, causing enormous economic losses in livestock (ruminants and camels) as well as human mortality [17].
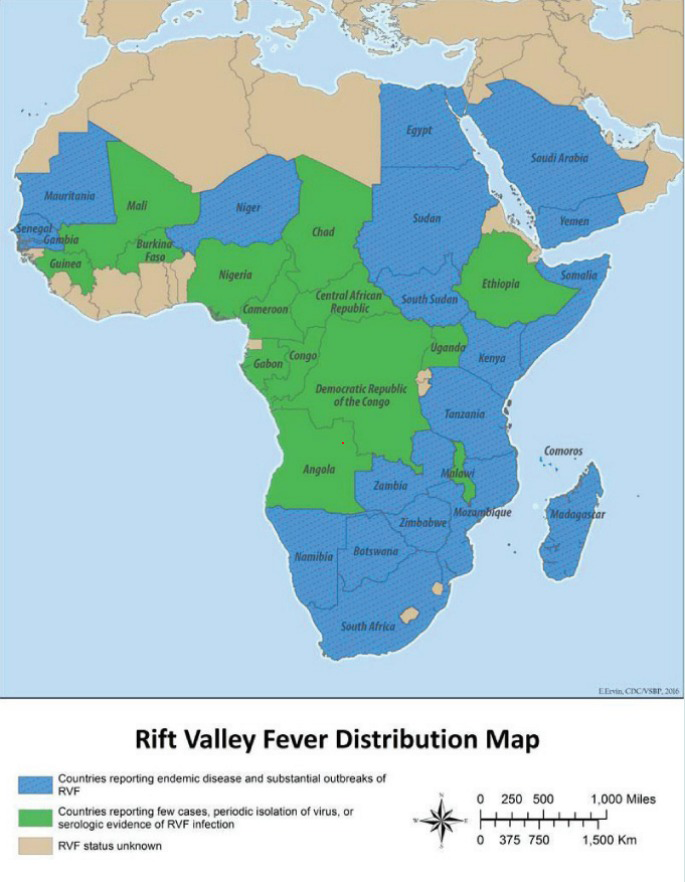
Source: [30]. Figure 2: Geographical distribution of RVF in Africa and Middle East.
Other than Africa, in Saudi Arabia and Yemen in 2000, an RVF outbreak was first identified in humans and livestock [5]. The importation of animals (cattle and camels) from endemic regions or the importation of mosquitoes carrying the disease was both factors in that outbreak. A case of RVFV was identified in 2007 on Mayotte (French island), likely introduced during the importation of infected ruminants from an endemic region [28]. In Algeria and Libya, where incidences of RVF in small ruminants have very recently (January 2020) been documented [6]. In 2022, Mauritania has reported RVF outbreaks, and Burundi is dealing with the nation’s first-ever RVF epidemic. This disease is affecting the nation’s livestock, which is a significant source of income and an essential part of ensuring food security and adequate nutrition [8].
The RVF virus can be found in a variety of ecological climates, including the arid regions of western Africa and the Arabian Peninsula, the sub-humid region of east Africa, the wet forests of central Africa, the dam-irrigated agricultural land of Egypt, Mauritania, and Sudan, and the humid highlands of Madagascar [29]. The reports by different groups on the cyclic epidemic interval have typically occurred at 5–15 years [21].
Vector of Rift Valley Fever: Various mosquito species involved in the spread of this disease can be infected with RVFV [31]. In areas where outbreaks have been observed, RVFV has been isolated from a wide range of mosquito species of many genera. RVFV vectors, which were into primary maintenance, secondary amplification vectors, and potential mechanical vectors (Table 2) [32].
| Primary (maintenance) vectors | Secondary (amplifying) Vectors | Potential mechanical vectors |
|---|---|---|
| Aedes | Culex, | Culicoides |
| Anopheles, | sand flies | |
| Eretmopodites, | stable flies | |
| Mansonia | Midges | |
| ticks |
Table 2: ** Rift valley fever virus different vector genera.
Source: [29, 33]. Table 2: Rift valley fever virus different vector genera.
Mode of Disease Transmission: The primary method of RVFV transmission among livestock is through mosquito bites [11]. While feeding on infected animals, the Aedes mosquito becomes infected with RVFV, which then spreads transovarially to the developing egg [30]. This cycle happens when there is unusually high rainfall and when dams flood. In mosquito eggs produced near the border of typical dry depressions, known as dambos, which are widespread throughout grassy plateau regions, the virus can survive for an extended period. The eggs hatch, and the affected adult female mosquitoes transmit the virus to nearby livestock and wildlife vertebrate hosts serving as amplifiers (Figure 3) [12], while secondary vectors, including Culex, Anopheles, Eretmopodites, Mansonia mosquitoes, and other arthropods, contribute to the transmission to non-infected domestic animals and humans [34].
In addition, the direct animal-to-animal transmission of RVFV neither occurs among herds nor experimentally in the laboratory [35]. Large quantities of virus particles are present in the tissues and membranes of aborted foetuses. Reusing needles while administering vaccinations has the potential to spread disease to animals, especially in areas with limited resources. Additionally, breastfeeding animals may have the ability to transmit disease to their young through milk [36]. Consequently, humans can contract RVFV when domestic livestock experience widespread sickness and death, either through an infected mosquito bite or exposure to infected animal blood, bodily fluids, or tissues [37], though the precise mode of infection remains uncertain in many human cases. A high risk of RVFV exposure exists in endemic areas for professions like ranchers, farmers, abattoir workers, and veterinarians. All unprocessed fresh animal products that come from infected areas during an epizootic should be regarded as potentially infective and treated accordingly [38]. The animal products that are considered include fresh, chilled, and frozen meat, wool, bones, skins, hides, and the milk and milk products of sick animals. Few cases of vertical transmission in infants have been documented in humans. However, transmission between humans does not seem to occur, but viruses have been demonstrated to function in laboratory conditions as a result of aerosol transmission [37].
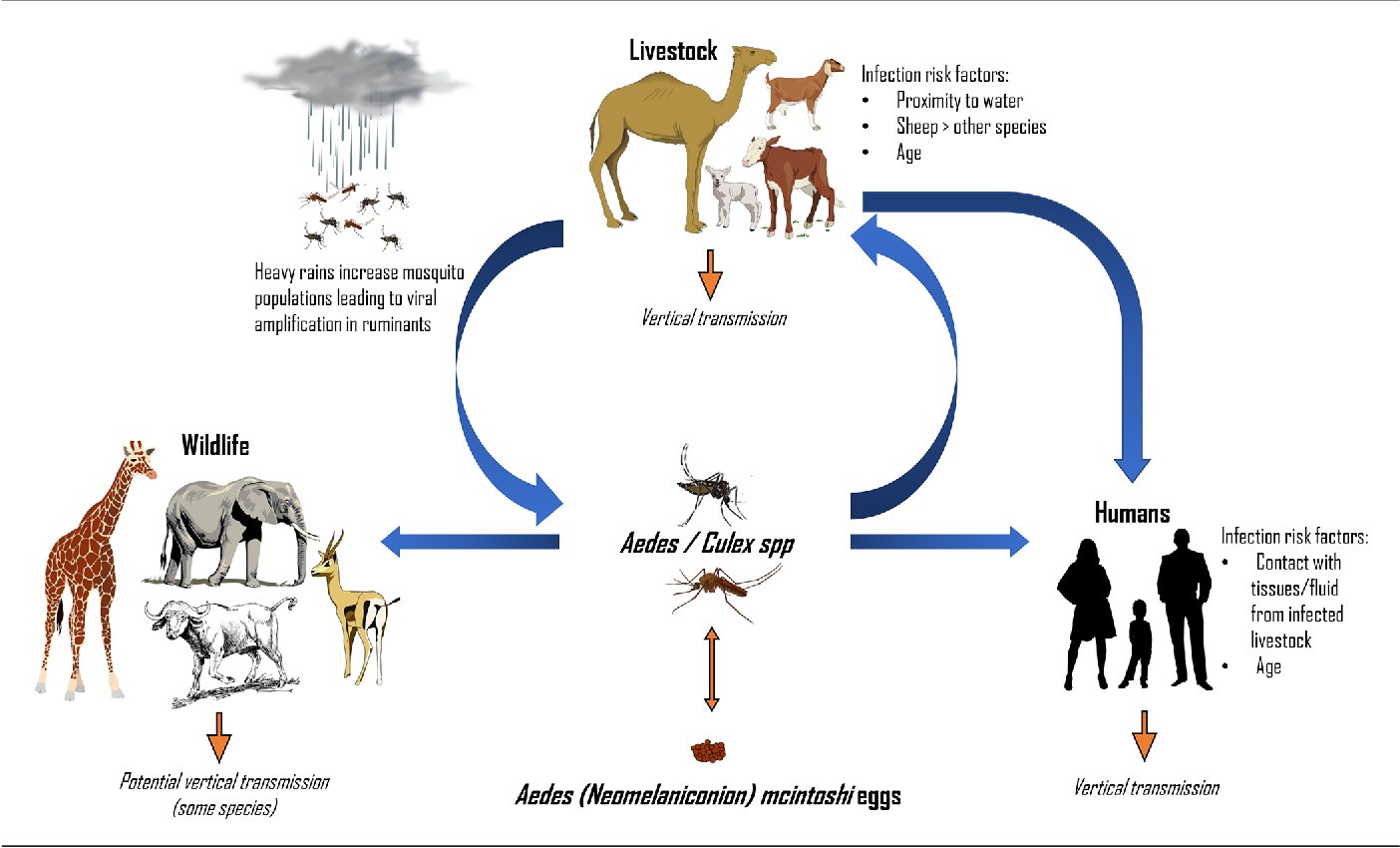
Source: [1] Figure 3: Transmission cycle of Rift valley fever virus.
Risk Factors for Spread of Disease: Rainfall has a significant influence on the interactions of the several components (vertebrate host, vectors, and virus) that make up the RVF transmission cycle [39]. Irrigation, rainfall, and human population density were the main causes of RVF cases, regardless of seasonal, climatic, or geographical change [40]. The high vector densities and the abundance of naive ruminant populations, particularly those that were extremely susceptible, both aided in the virus’s rapid spread and detrimental consequences on humans [41].
The rise in temperature helps mosquitoes survive and extend their active season. In order to provide the standing water surface needed for egg laying and larval development, heavy rainfall is also necessary. High air humidity improves the dynamics of vector populations [42].
Pathogenesis
The RVF virus replicates rapidly and at very high titers in target tissues after entry via mosquito bite, percutaneous injury, or oropharyngeal aerosol [42]. The virus spreads from the initial site of replication after infection to vital organs such as the spleen, liver, and brain, which either suffer harm from the pathogenic effects of the virus or its immunological pathological processes or heal as a result of general and specific host responses. Lymphatic drainage carries the virus from the inoculation site to the lymph nodes, where it replicates and spins out into the circulation, causing viremia and systemic infections [43]. In severe cases, hepatic necrosis is prominent, and necrotic foci can be observed in the brain of patients exhibiting the less frequent encephalitic form of the disease. RVF virus replication in cells is highly cytotoxic, suggesting that most cellular destruction in acute illness is likely due to direct virus killing of host cells [16].
Clinical Sings
In Animals: The incubation period for Rift Valley Fever varies across species, ranging from 12 hours in newborn animals to 4-6 days in humans [11]. Clinical symptoms of RVF affect animals’ age and species, with adult sheep and newborn lambs the most susceptible, experiencing abortion storms and high neonatal mortality in endemic areas, where infected animals can abort at any stage of gestation, with an abortion rate ranging from 40 - 100% [15]. Young animals with the condition frequently exhibit anorexia, weakness, and lymphadenopathy in addition to elevated body temperatures. Hemorrhagic or fetid diarrhoea, melena, regurgitation, signs of abdominal pain, a serosanguineous or bloodstained mucopurulent nasal discharge and elevated respiratory rate may also be seen [19]. Cattle are less prone to illness than sheep and goats [1]. Clinical signs in camels during an outbreak include sudden death or an acute syndrome characterized by fever, ataxia, and expiratory wheeze, and dyspnea, edema at the base of the neck, icterus, blood-tinged nasal discharge, and oral mucosal hemorrhages. Hemorrhagic symptoms typically cause camels to pass away within a few days [43]. In Human: In most cases, Rift Valley Fever (RVF) presents as a flu-like febrile disease that is self-limiting [11], with early symptoms being non-specific, likely resulting in many undetected cases. The case fatality rate is estimated to be between 1% and 30% in certain endemic areas [44]. Acute RVFV infection during pregnancy is associated with a higher risk of miscarriage. The signs in human cases are often characterized by three major complications: neurological symptoms such as headaches, irritability, confusion, encephalitis leading to coma, and visual hallucinations. Ocular complications include retinitis, vision loss, and complete or partial blindness. Hemorrhagic symptoms are marked by fever, muscle pain, and intense bleeding from mucous membranes [45].
Diagnosis
A combination of molecular and serological methods is ideal for clinical testing. Nonetheless, the usefulness of testing is determined by disease dynamics. periods during which specific virological indicators, such as viruses, viral RNA, IgG, and IgM, as well as liver abnormalities, are most likely to be found. Due to differences in susceptibility within and between species, there may be some variance in illness kinetics between humans and other animal species [46]. Virus Isolation: Isolation of infecting viruses from blood at the acute phase of disease is the most sensitive method of diagnosing viral disease [47]. Samples from the liver, which is the main location of RVFV replication, as well as those from the spleen, kidney, lymph nodes, blood, and samples from aborted foetuses, should be obtained for histopathology, preferably in sterile containers for viral isolation. The brain is a useful specimen to send to the lab on ice for diagnosis in the case of an autolyzed foetus [38]. Serology: Virus neutralization is the gold standard serological assay used for the determination of vaccine potency and is the OIE recommended test for international trade [1]. Cannot differentiate the presence of antibodies in naturally infected animals from animals vaccinated with RVF vaccine; detects antibodies against RVF virus in the serum of a variety of species, is highly specific, and will record the earliest response [36].
Antibody detection by enzyme-linked immunosorbent assay can be used to confirm presence of specific IgG and IgM antibodies. The use of inactivated whole virus or mouse liver antigens has recently been replaced by recombinant nucleocapsid proteins as antigens [48]. The detection of IgM indicates a current or recent infection. However, IgG-based enzyme-linked immunosorbent assay cannot distinguish between past and current infections unless paired serum samples (acute and convalescent) are analysed and a four- fold increase in antibody titer is observed [36]. Molecular Methods: Molecular methods are used for detection viral RNA in blood, tissue and mosquito samples. The viral RNA is discovered using RT-PCR. It is a very specific and sensitive molecular tool for the diagnosis of RVF in the early phase of the disease. PCR is used for rapid diagnosis, antigen detection, and to detect the RVF virus genome in infected animal sera and in mosquitoes [21]. Quantitative RT- PCR is also used to quantify the virus load in mosquito samples during RVFV outbreaks. RT-PCR followed by sequencing of the nucleocapsid protein-coding region has been used in phylogenetic analysis [36].
Status of Rift Valley Fever in Ethiopia
The Somali region of Ethiopia is one of the most active livestock trade areas, and according to various sources, 60– 80% of Somali national livestock exports from this region of Ethiopia are primarily due to informal cross-border trade. No clinical cases of RVF have been detected or reported in Ethiopia. Due to its geographic proximity to disease-endemic countries like Kenya, northern Somalia, Sudan, and South Sudan, cross-border livestock movement, and the capacity of infected mosquitoes to migrate greater distances via wind, Ethiopia will always be susceptible to clinical RVF during the epizootic periods of the diseases in endemic countries [29].
Economic Impacts of Rift Valley Fever
The Rift Valley Fever disease (RVF) has severe economic consequences, including large-scale animal abortions, food security threats, and strict trade restrictions. It also leads to livestock market closures, high control costs, and severe losses in livestock output (meat and milk) [49]. Pastoralists are particularly affected by RVF because they live in vulnerable communities with low levels of resilience to adversity [39]. Due to high rates of animal death and abortion, livestock farmers were the first group to directly experience the socioeconomic effects of RVF. In particular for young ruminants, this constitutes a significant loss of stock [35]. The disruption of herd dynamics may also have long- term impacts, including productivity losses that continue for several years or even several animal generations. Long-term and subject to the combined influence of various economic forces besides the rigid herd dynamics, these consequences are felt [50].
The livestock value chain and its associated services will be impacted by RVF’s effects on producers. RVF may have a stronger overall effect on the economy as a whole and on other service providers throughout the livestock supply chain than it does on individual farms [51]. The effects could be qualitative (value chain reconfiguration), quantitative (performances and socio-economic values), or both, short- term (less than a year) or long-term (over a year). A portion of these effects can be attributed to variations in the price and availability of animals on the market. Beyond the livestock value chain, there may be spillover effects on other agricultural value chains; for example, the importation of other agricultural products from the afflicted nations may be forbidden, in addition to non-agricultural sectors like transportation or tourism [52].
Due to international health regulations, RVF outbreaks may impose export restrictions on live animals and animal products. National economies can be greatly affected by export bans, which are a significant part of national trade balances [52]. A series of RVF-related trade bans can adversely affect national treasuries, the value of national currencies, and the cost of imports. Exports of livestock are a significant source of employment, revenue, and foreign exchange [53]. A significant portion of employment, revenue, and foreign cash comes from exporting livestock. As a result of the export restrictions, livestock prices decline and trading conditions deteriorate, further eroding the purchasing power and standard of living of pastoralists [35].
The impact on livestock marketing is more severe, especially during times of religious festivals. Due to high animal population density and religious observances, the risk of RVF infection rises during these times [54]. As a result, the zoonotic character of RVF causes a loss of confidence in an importing country, prompts a long-lasting trade restriction on livestock and animal products during an outbreak, and has significant economic and social repercussions on all sectors (livestock and other industries) [55]. Rift Valley fever outbreaks negatively impact the livestock industry and human population, especially in developing and transitional nations. The risk is high due to the insufficient public health infrastructure in low-resource settings, which is insufficient to support routine disease surveillance, prevention, and control operations, especially when outbreaks occur every 5 to 15 years [54].
Control and Prevention of Rift Valley Fever
There is no specific treatment for RVFV infection in humans or animals; rather, supportive therapy is the mainstay of care [48]. Many different preventative methods are typically discussed, including the following: immunizing animals in endemic areas; managing vector (mosquito) populations; keeping track of changes in the climate; and movement management.
Vaccination: Vaccination is the best method in animals for the protection of human health. To control RVFV, the best way is to vaccinate all susceptible ruminants before an anticipated epidemic [1]. RVF can be controlled in endemic countries with both live attenuated and killed vaccinations, which are readily available. RVF can be controlled in endemic countries with both live attenuated and killed vaccinations, which are readily available. Another livestock vaccine, clone 13, was one of a number of viral clones isolated from a human patient infected with the 74HB59 strain in the Central African Republic. Clone 13 has proven safe and immunogenic after a single dose in cattle, sheep and goats [56]. Vector Control: At various stages of the development of mosquitoes, vector control measures can be put into place. By focusing on the application of pesticides, adult mosquitoes can be managed. It can be used to target resting adults via thermal fogging or ultra-low volume spraying, or it can directly target flying or resting adults [57]. In order to survive, mosquito larvae must reside in water. Any type of standing water, including ponds, used tyres, tarps, and birdbaths, might be a home for them. The control of this stage concentrates on ongoing management of mosquito egg-laying regions since mosquito larvae continue to live in the same body of water where they emerged from eggs [58]. Movement Control and Surveillance in RVF free Areas: A comprehensive quarantine program is crucial for controlling virus entrance, establishment, and transmission in high- risk regions. This prevents contaminated animals, products, and fomites from leaving infected or suspicious places. Management strategies include moving livestock to pastures with better drainage and wind protection, or containing animals in sheds with mosquito-proofing technology to lower RVF frequency [59]. Regular surveillance and prediction are crucial for effective disease control and prevention in non-endemic countries, especially along shared borders with neighboring endemic countries. Identifying potential mosquito species transmitting RVF helps acquire biological information, such as oviposition sites and biting habits [60].
Conclusion and Recommendations
Rift Valley Fever has a significant economic impact for both the RVF-affected countries and their livestock trade partners in other countries. It affects livestock trade through the closure of livestock markets, and bans on the movement and slaughter of livestock, significantly in countries where income mainly depends on livestock trade. Until now, the disease was confined to certain regions of sub-Saharan Africa. But now, as outbreaks in the Arabian Peninsula show, the disease spreads beyond traditional herds into new areas. The epidemiology of RVF is complex and multiple mosquito vectors, livestock, and wildlife are involved in transmission. Rainfall, flooding, animal contact; breeding grounds, livestock availability, and migration are all factors in the epidemiology of Rift Valley fever.
Based on the conclusion the following points are forwarded as recommendations:
- The complex ecological cycle should be considered while planning surveillance programs for the disease.
- The disease endemic countries and its trading partners should work together to maximize the benefits of livestock production and consider cost-effectiveness analyses for Rift Valley fever planning and monitoring.
- Animal movement control and biosecurity measures should be taken, especially in disease-free countries.
Ethical Approval and Consent to Participate
Ethical clearance will be obtained from the Ethical Review Board of Ambo University.
References
-
Wright D, Kortekaas J, Bowden TA, Warimwe GM (2019) Rift Valley fever: biology and epidemiology. Journal of General Virology 100(8): 1187-1199.
-
Nanyingi MO, Munyua P, Kiama SG, Muchemi GM, Thumbi SM, et al.(2015) A systematic review of Rift Valley Fever epidemiology 1931-2014. Infection ecology & epidemiology 5(1): 28024.
-
Pepin M, Bouloy M, Bird BH, Kemp A, Paweska J (2010) Rift Valley fever virus (Bunyaviridae: Phlebovirus): An update on pathogenesis, molecular epidemiology, vectors, diagnostics and prevention. Veterinary research 41(6): 61.
-
Pienaar JN, Peter NT (2013) Temporal and spatial history of Rift valley fever in South Africa 1950 to 2011. Onderstepoort Journal of Veterinary Research 80(1): 1-13.
-
Akash S, Islam MR, Rahman MM (2023) Rift Valley fever. A re-emerging zoonotic disease, pathogenesis, epidemiology, current status, and future perspective– correspondence. International Journal of Surgery 109(3): 587-588.
-
OIE (2012) Regional Strategy for Priority Transboundary Animal Diseases (2021-2025).
-
Cecilia H, Vriens R, Kortekaas J, Schreur P, Wit M, et al. (2021) Heterogeneity of Rift Valley fever virus transmission potential across livestock hosts, quantified through a model-based analysis of host viral load and vector infection. PLoS Comput Biol 93: 1-23.
-
(2022) Disease Outbreak News; Rift Valley fever Mauritania. WHO.
-
Wichgers SPJ, Bird BH, Ikegami T, Bermudez ME, Kortekaas J (2023) Perspectives of Next-Generation Live-Attenuated Rift Valley Fever Vaccines for Animal and Human Use. Vaccines 11(3): 707.
-
Connors KA, Hartman AL (2022) Advances in understanding neuropathogenesis of rift valley fever virus. Annual Review of Virology 9: 437-450.
-
Nielsen SS, Alvarez J, Bicout DJ, Calistri P, Depner, K, et al. (2020) Rift Valley Fever-epidemiological update and risk of introduction into Europe. EFSA Journal 18(3): 6041.
-
Eastwood G, Sang RC, Lutomiah J, Tunge P, Weaver SC (2020) Sylvatic mosquito diversity in kenya-considering enzootic ecology of arboviruses in an era of deforestation. Insects 11(6): 342.
-
Iacono G, Cunningham A, Bett B, Grace D, Redding DW, et al. (2018) Environmental limits of Rift Valley fever revealed using Eco epidemiological mechanistic models. Proceedings of the National Academy of Sciences 115(31): 448-7456.
-
Cecilia H, Vriens R, Wichgers SPJ, Wit MM, Metras R, et al. (2020) Heterogeneity of Rift Valley fever virus transmission potential across livestock hosts, quantified through a model-based analysis of host viral load and vector infection. PLoS Computational Biology 18(7): e1010314.
-
Lubisi BA, Mutowembwa PB, Ndouvhada PN, Odendaal L, Bastos AD, et al. (2023) Experimental Infection of Domestic Pigs (Sus scrofa) with Rift Valley Fever Virus. Viruses 15(2): 545.
-
Mariner JC, Raizman E, Pittiglio C, Bebay C, Kivaria F, et al. (2022) Rift Valley fever action framework. FAO Animal Production and Health Guidelines.
-
Meegan J, Bailey CL, Monath TP (2019) Rift valley fever. WHO.
-
Waqar MA, Qureshi A, Ahsan A, Sadaqat S, Zulfiqar H (2023) Epidemiology, Clinical Manifestations, Treatment Approaches and Future Perspectives of Rift Valley Fever. Epidemiology of Rift Valley Fever. Pakistan Journal of Health Sciences pp: 2-8.
-
Spickler AR (2015) Rift Valley fever fact _sheet. The Center for food security and public health.
-
Kitandwe PK, McKay PF, Kaleebu P, Shattock RJ (2022) An Overview of Rift Valley Fever Vaccine Development Strategies. Vaccines 10(11): 1794.
-
Lean FZ, Johnson MM (2022) Rift Valley fever: a zoonotic viral haemorrhagic disease. Journal of Medical Microbiology 72(12): 1619.
-
(2015) Rift Valley Fever. CDC.
-
Atuman Y, Kudi C, Abdu PA, Abubakar A, Okubanjo O (2020) Antibodies to Rift Valley Fever virus in some wildlife and domestic animals in Bauchi state, Nigeria. International Journal of Infectious Diseases 101: 261- 262.
-
(2017) Panel on Animal Health and Welfare. Vector‐ borne Diseases. EFSA J 15(5): 4793.
-
(2023) Rift valley fever (RVF). CDC.
-
Sall PM, Zanoto A, Sene OK, Zeller HG, Digoutte JP, et al. (1999) Genetic Reassortment of Rift Valley Fever Virus in Nature. Journal of Virology 73(10): 8196-8200.
-
Paweska JT (2014) Rift valley fever. In Emerging Infectious Diseases. Academic Press pp: 73-93.
-
Chevalier V, Pepin M, Plee L, Lancelot RJ (2010) Rift Valley fever-a threat for Europe. Eurosurveillance 15(10): 19506.
-
Tran A, Trevennec C, Lutwama J, Sserugga J, Gely M, et al. (2016) Development and assessment of a geographic knowledge-based model for mapping suitable areas for Rift Valley fever transmission in Eastern Africa. PLoS neglected tropical diseases 10(9): e0004999.
-
Regassa SL, Tarafa M, Guta BB (2019) Role of Vectors and Climate Change on the Epidemiology of Rift Valley Fever. J Veter Sci Med 7(1): 7.
-
Sang R, Arum S, Chepkorir E, Mosomtai G, Tigoi C, et al. (2017) Distribution and abundance of key vectors of Rift Valley fever and other arboviruses in two ecologically distinct counties in Kenya. PLoS neglected tropical diseases 11(2): 5341.
-
Linthicum KJ, Britch SC, Anyamba A (2016) Rift Valley fever: an emerging mosquito-borne disease. Annual review of entomology 61: 395-415.
-
Lumley S, Horton DL, Hernandez TLL, Johnson N, Fooks AR, et al. (2017) Rift Valley fever virus: strategies for maintenance, survival and vertical transmission in mosquitoes. Journal of General Virology 98(5): 875-887.
-
Hartman A (2017) Rift valley fever. Clinics in laboratory medicine 37(2): 285-301.
-
Peyre M, Chevalier V, Abdo SS, Velthuis A, Antoine MN, et al. (2015) A systematic scoping study of the socio‐ economic impact of Rift Valley fever: research gaps and needs. Zoonoses and public health 62(5): 309-325.
-
Mansfield KL, Banyard AC, McElhinney L, Johnson N, Horton DL, et al. (2015) Rift Valley fever virus: A review of diagnosis and vaccination, and implications for emergence in Europe. Vaccine 33(42): 5520-5531.
-
Kwasnik M, Rozek W, Rola J (2021) Rift Valley fever a growing threat to humans and animals. Journal of Veterinary Research 65(1): 7-14.
-
Chopra H, Dhama K, Emran TB (2023) Re-emergence of Rift Valley fever : an update and preventive measures. International Journal of Surgery 109(1): 68-70.
-
Baba M, Masiga DK, Sang R, Villinger J (2016) Has Rift Valley fever virus evolved with increasing severity in human populations in East Africa? Emerging microbes & infections 5(1): 1-10.
-
Redding DW, Tiedt S, Iacono G, Bett B, Jones KE (2017) Spatial, seasonal and climatic predictive models of Rift Valley fever disease across Africa. Philosophical Transactions of the Royal Society B: Biological Sciences 372(1725): 20160165.
-
WHO (2009) Joint FAO - WHO experts consultation on Rift Valley fever outbreaks forecasting models Rift Valley fever outbreaks forecasting models.
-
Sayed A, Kamel M (2020) Climatic changes and their role in emergence and re-emergence of diseases. Environ Sci Pollut Res Int 27(18): 22336-22352.
-
Fawzy M, Helmy YA (2019) The one health approach is necessary for the control of Rift Valley fever infections in Egypt: A comprehensive review. Viruses 11(2): 139.
-
Sado FY, Tchetgna HS, Kamgang B, Djonabaye D, Nakoune E (2022) Seroprevalence of Rift Valley fever virus in domestic ruminants of various origins in two markets of Yaounde, Cameroon. PLoS Neglected Tropical Diseases 16(8): 10683.
-
Javelle E, Lesueur A, Pommier SV, Laval F, Lefebvre T, et al. (2020) The challenging management of Rift Valley Fever in humans: literature review of the clinical disease and algorithm proposal. Annals of Clinical Microbiology and Antimicrobials 19(1): 1-18.
-
Ikegami T, Makino S (2011) The pathogenesis of Rift Valley fever Virus. Infectious Disease of Livestock 3(5): 493-519.
-
Idris I, Adesola RO (2022) The Existence of Rift Valley Fever Virus in Nigeria: Past, Present and Future. Intersect: The Stanford Journal of Science, Technology, and Society 16(1).
-
Petrova V, Kristiansen P, Norheim G, Yimer SA (2020) Rift valley fever: diagnostic challenges and investment needs for vaccine development. BMJ Global Health 5(8): 2694.
-
Aziz MA, Nur HM, Nantima N, Hassan AM, Malik KH (2018) Effect of Trans boundary Animal Diseases on Livestock Trade and Export in Sudan, a Case Study on Rift Valley Fever. Journal of Medical and Biological Science Research 4(1): 1-10.
-
Mburu CM, Bukachi SA, Bett B (2022) Pastoralists perceptions on the impact of Rift valley fever disease following an outbreak in North Eastern Kenya 12(1): 1-8.
-
Murithi RM, Munyua P, Ithondeka PM, Macharia JM, Hightower A, et al. (2011) Rift Valley fever in Kenya: history of epizootics and identification of vulnerable districts. Epidemiology & Infection 139(3): 372-380.
-
Handlos M (2009) Assessment of the estimated costs of past disease outbreaks in Yemen, Rain fed Agriculture and Livestock Project: International expertise service for the General Directorate of Animal Resources, Yemen. Sana’a and Vientiane, Yemen. IDA.
-
Sindato C, Karimuribo ED, Pfeiffer DU, Mboera LE, Kivaria F, et al. (2014) Spatial and temporal pattern of Rift Valley fever outbreaks in Tanzania; 1930 to 2007. PLoS One 9(2): e88897.
-
Mahmoud AS, Sawesi OK, Waer OR, Bennour EM (2021) Rift valley fever in Africa with the emerging interest in Libya. International Journal of One Health 7: 237-245.
-
Rich KM, Wanyoike F (2010) An assessment of the regional and national socio-economic impacts of the Rift Valley fever outbreak in Kenya. The American journal of tropical medicine and hygiene 83: 52-57.
-
Njenga MK, Njagi L, Thumbi SM, Kahariri S, Githinji J (2015) Randomized controlled field trial to assess the immunogenicity and safety of Rift Valley fever clone 13 vaccine in livestock. PLoS Neglected Tropical Disease 9(3): 3550.
-
Bird BH, Nichol ST (2012) Breaking the chain: Rift Valley fever virus control via livestock vaccination. Current opinion in virology 2(3): 315-323.
-
Chengula AA, Kasanga CJ, Mdegela RH, Sallu R, Yongolo M (2014) Molecular detection of Rift Valley fever virus in serum samples from selected areas of Tanzania. Tropical animal health and production 46: 629-634.
-
Melkamu S (2018) Review on economic significance and current diagnostic techniques on Rift valley fever. International Journal of Advanced Research Biological Sciences 5(7): 115-122.
-
Taira K, Toma T, Tamashiro M, Miyagi I (2012) DNA barcoding for identification of mosquitoes (Diptera: Culicidae) from the Ryukyu Archipelago, Japan. Medical Entomology and Zoology 63(4): 289-306.
- The Digital Stethoscope: Harnessing AI in Veterinary Medicine Without Losing Our Healing Touch
- Meningoencephalomyelitis of Unknown Etiology: Short-Term Effect of Two Treatment Protocols on Cerebrospinal Fluid
- Safety and Efficacy of the HomeoPet Cough in Domestic Pets –A Clinical and Correction Analysis Based Upon User Response Survey
- Non Human Animals Responses to Social Loss
- Owner Reported Clinical Outcomes of a Homeopathic Proprietary Preparation for the Treatment of Upper Respiratory and Nasal Disorders in Companion Animals
- Effects and Diagnostic Approach of Ultrasound in Veterinary Practice: A Systematic Review