The Comparative Study of OAE and ABR in Neonatal Intensive Care Units
Study Aims: To compare the correlation of two screening protocols using otoacoustic emissions (OAE) is screening and auditory brainstem response (ABR) in infants requires intensive care. Methods: Three hundred newborns in NICU were tested using both OAE and ABR at the ages of 3 days, 42 days, and 3 months. Results: At the age of 3 days, OAE referral rates were significantly higher than the rates of abnormal ABR (χ2=8.75, p0.05; χ2=0.15, P>0.05). Conclusion: We demonstrated that there is significantly difference between the OAE referral rate and the rate of abnormal ABR of infants in the NICU at 3 days after birth. The difference became smaller with age. So combined OAE/ABR can be considered an efficient hearing screening method for NICU infants at risk from the first hearing screen at 3 days after birth.
Background
According to global research statistics, sensorineural hearing loss (SNHL) is one of the most common congenital anomalies, occurring in 1-3 cases per 1000 otherwise healthy newborn infants. In certain high-risk populations, this value could increase 10- to 50-fold [1]. The high incidence of hearing loss among infants in neonatal intensive care units (NICU) could be attributed to specific etiologies, such as a family history of hereditary deafness, uterine infection, very low birth weight (VLBW), preterm birth, hyperbilirubinemia, and asphyxia. The criteria for high-risk newborns, as established by the American Academy of Pediatrics joint committee on infant hearing in 1994 include: preterm birth, neonatal sepsis, hypoxia, jaundice, craniofacial anomalies, ototoxic drugs, and requirements for ventilatory support [2]. Recent studies have shown that auditory neuropathy spectrum disorder (ANSD) covers a wide range of auditory dysfunction [3, 4, 5]. ANSD involves the brainstem and cortical maturation. From this perspective, babies at high risk for hearing loss require precise evaluation, including screening of auditory function along the largest possible portion of the hearing pathway, and not only the cochlea.
Hearing screening tests for neonates are currently composed of two components
Auditory brainstem responses (ABR) and otoacoustic emissions (OAEs). ABR records the electrical response of the cochlea and the auditory neural pathways. OAEs are generated by the outer hair cells of the cochlea, OAEs represent sounds generated by the cochlea. The TEOAE results are presented as red light (refer) and green light (pass). Passing scores do not necessarily indicate normal hearing, as passing newborns may have mild hearing loss or auditory neuropathy. Newborns in the NICU are considered high risk for ANSD [6]. In this regards, tests of OAE alone may be inappropriate to detect neural hearing loss and ABR is recommended as the important screening tool for infants in NICU. We recently studied the screening of NICU newborns for hearing loss with both OAE and ABR. We aimed to identify the incidence of hearing loss in NICU babies and to classify the degree of hearing loss in a manner that describes the main causes for hearing loss in this population. We focused on the importance of suitable, adequate hearing assessment. Another purpose of this study was to investigate the concordance between OAE and ABR.
Methods
Subjects
The study was approved by the Research Ethics Committee of China Medical University. We evaluated 375 newborns between June 2010 and April 2012. All were admitted to our hospital’s NICU for the following risk factors: prematurity, infant respiratory distress syndrome (IRDS), neonatal infection, hyperbilirubinemia, ABO hemolysis, and cytomegalovirus infection. The study consisted of 375 newborns (204 boys and 171 girls). All underwent two screening procedures. In accordance with Ethical Committee requirements, the study protocol was fully explained to parents, who provided written consent for each baby. Three hundred and seventy-five babies were screened on the third day of life. Forty-eight infants were lost to follow up at 42 days. Three months after birth, 300 infants were available for follow-up, constituting the study population.
Study protocol
ABR and TEOAE were performed by trained technicians, supervised by a licensed audiologist. ABR threshold elevations were considered as reflecting mild (36-50 dB nHL), moderate (51-70 dB nHL), severe (71-90 dB nHL), and profound (>90 dB nHL) categories of hearing impairment [7]. TEOAE was performed after removal of debris. The results are presented as red light (refer) or green light (pass). The parents of infants were informed of the results of the first test and recommended to return for a follow-up evaluation once the infants had reached 42 days of age. All newborns were tested in deep sleep in a soundproof room. Both ears were tested sequentially. We recorded absolute latencies, inter peak intervals, and thresholds. The two types of measurements, TEOAE and ABR, were performed at 3 days, 42 days, and 3 months, and their results analyzed accordingly. Statistical analysis was conducted with SPSS version 13.0 statistical software. The chi-squared test was used. A P-value of less than 0.05 was considered statistically significant. TEOAE combined with ABR were also studied using a concordance test.
Results
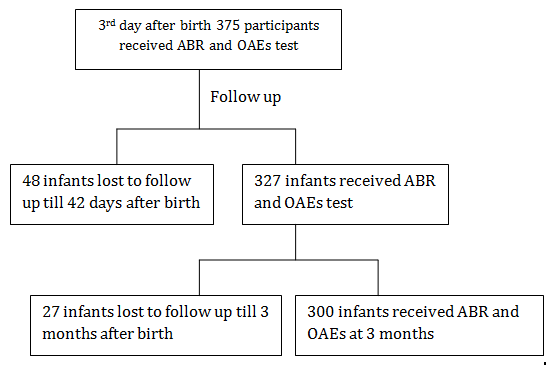
Figure 1: The process of the hearing screening in NICU. (Figure 1) illustrates the process of the hearing screening in the NICU. Among the 300 at-risk infants who were comprehensively tested at 3 days, 42 days, and 3 months with the two methods (TEOAE and ABR), there were 164 boys (54.67%) and 136 girls (45.33%), with a male/female ratio of 1.21. There was no statistically significant difference among sexes (χ2=2.61, P<0.05). All newborns were tested 72 h after birth. Ninety-nine newborns failed the first TEOAE screening test. Sixty-four newborns (unilateral or bilateral SNHL) had abnormal ABR. This indicated a statistically significant difference (χ2=8.75, P<0.05) between TEOAE and ABR tests on the first test. At the 42-day screening, 67 infants failed the second TEOAE screening test and 71 infants had an abnormal ABR. There was no statistically significant difference between the results of these two tests (χ2=0.19, P>0.05). At the 3-month screening, 69 infants failed the third TEOAE screening test and 73 infants had an abnormal ABR. There was no statistically significant
| OAE | Referral | Rates (%) | ABR | Abnormal | Rates (%) | |
|---|---|---|---|---|---|---|
| Left ear | Right ear | Total | Left ear | Right ear | Total | |
| 3 days | 10.8% (81/750) | 10.53% (79/750) | 21.33% (160/750) | 6.93% (52/750)▲ | 7.2% (54/750)▲ | 14.13% (106/750)▲ |
| 42 days | 7.8% (51/654) | 8.41% (55/654) | 16.21% (106/654) | 8.87% (58/654) | 9.33% (61/654) | 18.20% (119/654) |
| 3 months | 9% (54/600) | 9.5% (57/600) | 18.5% (111/600) | 10.17% (61/600) | 10.5% (63/600) | 20.67% (124/600) |
Table 1: Comparing the OAE and ABR test results of babies in NICU (ears).
had mild neural hearing loss. This also verified that patients with mild hearing loss can pass the TEOAE.
| TEOAE pass | But ABR | Fail (≥36dBnHL) | |
| MRI: structure normal | Internal auditory canal stenosis | Acoustic nerve absence | |
| 3 months | 9 | 9 | 5 |
Table 2: The patients failed ABR and passed TEOAE.
Table 2: The patients failed ABR and passed TEOAE. Based on the ABR results at 3 days, 42 days, and 3 months, we found that varying degrees of hearing loss were detected in these infants (Table 3). All of the NICU newborns had one or more risk factors. In our study, we found that there were 104, 16, 10, 49, 9, and 112 babies, respectively, with risk factors of prematurity, IRDS, neonatal infection, hyperbilirubinemia, ABO hemolysis, and cytomegalovirus infection. There were 38, 18, and 10 babies with prematurity risk factors who had abnormal ABR results at 3 days, 42 days, and 3 months after birth. We determined the number of infants with hearing loss associated with each risk factor (Table 4).
| Degree of | Hearing | Loss | (n %) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mild | Moderate | Severe | Profound | |||||||||
| 3 days | 9.2%(69/750) | 2.13% (16/750) | 0.13% (1/750) | 0% (0/750) | ||||||||
| 42 days | 9.3% (61/654) | 4.13% (27/654) | 0.46% (3/654) | 0.46% (3/654) | ||||||||
| 3 months | 9.5% (57/600) | 5.17% (31/600) | 0.83% (5/600) | 0.33% (2/600) |
Table 3 Varying degrees of hearing loss (ears).
| Risk factors | 3 days | 42 days | 3 months | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Preterm | 36.54% (38/104) | 17.31% (18/104) | 9.62% (10/104) | ||||||||
| IRDS | 18.75% (3/16) | 12.5% (2/16) | 12.5% (2/16) | ||||||||
| Neonatal infection | 20% (2/10) | 40% (4/10) | 30% (3/10) | ||||||||
| Hyperbilirubinaemia | 28.57% (14/49) | 49.98% (24/49) | 61.22% (30/49) | ||||||||
| ABO hemolysis | 55.56% (5/9) | 77.78% (7/9) | 55.56% (5/9) | ||||||||
| Cytomegalovirus infection | 1.79% (2/112) | 14.29% (16/112) | 20.54% (23/112) |
Table 4 Risk factors of hearing loss (n=300).
Discussion
In the general population, one newborn per 500-1000 births presents with permanent hearing impairment. This is significantly greater than the incidence of other diseases routinely screened at birth [8]. In certain high- risk populations, this incidence can increase to 8-100 cases per 1000 infants [9]. Some of the importance of deafness as a public health issue comes from its tendency to cause sequelae and complications such as irreversible delays in speech and cognitive development [10]. Early detection and effective rehabilitation can decrease the number of hearing-disabled people and their degree of disability. Studies involving children in CHIP (Children who are high risk population) indicate that the diagnosis of hearing loss within the first few months of life allows for the opportunity to begin early intervention services for families with infants, and that early identification and early intervention results in significantly better language, speech, and social-emotional development [11]. Language development in hearing-impaired newborns who receive rehabilitation during the first 6 months of life is significantly better than in those who do not receive it until later [12, 13, 14]. In this regard, the Neonatal Hearing Screen (NHS) is essential to early detection of hearing loss in newborns. A recent systematic review of the evidence supporting Universal Newborn Hearing Screening (UNHS) has concluded that modern screening tests for hearing impairment can improve identification of newborns who have permanent hearing impairment [15].
In the present study, TEOAE screening alone was compared to ABR in NICU newborns. With TEOAE screening, the referral rates were 26.4%, 20.49%, and 23% at 3 days, 42 days, and 3 months of age. Our results showed that babies in the NICU had significantly higher referral rates after the OAE test (Table 1). We found the TEOAE referral rate decreased gradually. Preterm infants may have smaller external auditory canal and middle ear cavities than full-term babies. The transmission of OAE energy from the cochlea to the external ear is difficult and the evacuation of liquids takes longer. By 3 months, the subjects’ ear cavities had grown, and referral rates decreased. There are several factors that may explain why ABR showed higher rates of hearing abnormalities than TEOAE at 42 days and 3 months. The most important is auditory neuropathy [16, 17, 18, 19]. Most NICU babies with auditory neuropathy suffered from hyperbilirubinemia and asphyxia disorders at birth [20]. Some of the infants in the NICU showed delayed maturation of the auditory pathway, so that when they are older, they experienced spontaneous recovery of the hearing threshold. Our findings demonstrate that many of the infants in the NICU experienced delayed hearing improvement and progressive hearing loss. The analysis of the frequency of the occurrence of hearing loss in NICU infants with risk factors showed that it was reduced from 36.54% to 9.62% in preterm infants. The frequency of hearing loss in cytomegalovirus infection and hyperbilirubinemia increased significantly from 1.79% to 20.54% and from 28.57% to 61.22%. This illustrated that hearing in patients with cytomegalovirus infection and hyperbilirubinemia will deteriorate gradually while preterm infants have more of a chance to recover to normal hearing. Among the risk factors at 3 days, 42 days, and 3 months, ABO hemolysis, ABO hemolysis, and hyperbilirubinemia were associated with the highest rates of hearing abnormalities (55.56%, 77.78%, and 61.22%). Hyperbilirubinemia could damage the outer hair cells of the cochlea in infants [21]. While. 6.75% of Jordanian high risk infants failed bilaterally, and 9% unilaterally, in the second screening DPOAE test, 7.8% were diagnosed later with bilateral confirmed SNHL [22]. Diseases in which hearing deteriorates gradually in NICU infants should be paid close attention.
Conclusion
In the NICU population, the requirement for ABR testing was confirmed by the low concordance value between TEOAE and ABR at the first test (χ2 =8.75, P<0.05). Our experience highlights that, for the neonates in the NICU, auditory brainstem response is the most reliable method of assessing hearing level and minimizes the false positive rate. Using ABR and OAEs together is appropriate and may help NICU babies with hearing loss benefit from early remediation of their hearing deficit.
Acknowledgement
This study was supported by The Liaoning Province science and technology plan project (L2015586).
References
-
American Academy of Pediatrics, Joint Committee on Infant Hearing (2007) Year 2007 position statement: Principles and guidelines for early hearing detection and intervention programs. Pediatrics: 120(4): 898- 921.
-
Joint Committee on Infant Hearing 1994 Position Statement American Academy of Pediatrics Joint Committee on Infant Hearing. (1995) Pediatrics 95(1): 152-156.
-
Salamy A, Eldredge L, Tooley WH (1989) Neonatal status and hearing loss in high-risk infants. J Pediatr 114(5): 847-852.
-
Borradori C, Fauwer CL, Baclin T, Calame A (1997) Risk factors of sensorineural hearing loss in preterm infants. Biol Neonate 71(1): 1-10.
-
Borg E (1997) Perinatal asphyxia, hypoxia, ischemia, and hearing loss: An Overview. Scand Audiol 26(2): 77-91.
-
Berlin CI, Hood LJ, Morlet T, Wilensky D, Li L, et al. (2010) Multi-site diagnosis and management of 260 patients with auditory neuropathy/dys-synchrony (auditory neuropathy spectrum disorder). Int J Audiol 49(1): 30-43.
-
ZM Xu, Cheng WX, Yang XL (2011) Performance of two hearing screening protocols in NICU in Shanghai. Int J Pediatr Otorhinolaryngol 75(10): 1225-1229.
-
Meyer C, Witte J, Hildmann A, Hennecke KH, Schunck KU (1999) Neonatal Screening for hearing disorders in infants at risk: incidence, risk factors, and follow- up. Pediartics 104(4): 900-904.
-
Mehl AL, Thomson V (1998) Newborn hearing screening: the great omission. Pediatrics 101(1): 4.
-
Yoshinaga Itano C, Sedey AL, Coulter DK, Mehl AL (1998) Language of early-and-later-identified children with hearing loss. Pediatrics 102 (5): 1161- 1171.
-
Kok MR, Zanten GAV, Brocaar MP, Jongejan HT (1994) Click-evoked oto-acoustic emissions in very- low-birth infants: a cross-sectional data analysis. Audiology 33(3): 152-164.
-
Bonfils P, Francols M, Avan P, Londero A, Trotpux J, et al. (1992) Spontaneous and evoked otoacoustic emissions in preterm neonates. Laryngoscope 102(2): 182-186.
-
Kok MR, Zanten GAV, Brocaar MP (1993) Click- evoked otoacoustic emissions (EOAEs) in 1036 ears of healthy newborns. Audiology 32(4): 213-224.
-
Yoshinaga-Itano C (1995) Efficacy of early identification and intervention. Seminars in Hearing 16: 115-120.
-
Jennifer S, Martyn H (2002) Hearing screening. Pediatr Rev 23(5): 155-162.
-
Madden C, Rutter M, Hilbert L, GreinWald JH Jr, Choo DI (2002) Clinical and audiological features in auditory neuropathy. Arch Otolaryngol Head Neck Surg 128(9): 1026-1030.
-
Amaral MI, Martins JE, Santos MF (2010) A study on the hearing of children with non-syndromic cleft palate/lip. Braz J otorhinolaryngol 76(2): 164-171.
-
Rhee CK, Park HM, Jang YJ (1999) Audiologic evaluation of neonates with severe hyperbilirubinemia using transiently evoked otoacoustics emissions and auditory brainstem responses. Laryngoscope 109(12): 2005-2008.
-
Talero GC, Carvajalino MI, Samper BS, Ibanez PM (2008) Delayed auditory pathway maturation in the young children. Int J pediatr Otorhinolaryngol 72(4): 519-527.
-
Robertson CM, Howarth TM, Bork DL, Dinu IA (2009) Permanent bilateral sensory and neural hearing loss of children after neonatal intensive care because of extreme prematurity: a thirty-year study. Pediatrics 123(5): 797-807.
-
Oysu C, Aslan I, Ulubil A, Baserer N (2002) Incidence of cochlear involvement in hyperbilirubinemic deafness. Ann Otol Rhinol Laryngol 111(11): 1021- 1025.
-
Attias J, Al Masri M, Abukader L, Cohen G, Merlov P, et al. (2006) The prevalence of congenital and early- onset hearing loss in Jordanian and Israeli infants. Int J Audiol 45(9): 528-536.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?