Juvenile Nasopharyngeal Angiofibroma: Changing Trends
Introduction: Juvenile nasopharyngeal angiofibroma is a very rare, highly vascular, unencapsulated and locally invasive tumor. Recently a changing trend has been seen in its epidemiology, pathogenesis, diagnosis, medical management, pre-operative care, surgical management and post-operative care including radiotherapy. Aim: Study the changing trend basically in the Upper - Assam region of India and its prospects. Case setting and design: Retrospective study of patients presenting with JNA between the study period of one year (July 2014 - June 2015) in the, Department of Otolaryngology and Head and Neck Surgery, Assam Medical College, Dibrugarh, Assam, India. Materials and methods: Fifteen patients were treated in the study period. Different approaches were used. Results: Mean age of presentation was 16 years and more than 80 % of them were either Stage III or Stage IV. Different approaches like transpalatine, transpalatine along with transnasal, lateral rhinotomy and endoscopic surgery were used. Conclusion: Surgery by transpalatine approach should be the choice of treatment.
Introduction
Juvenile nasopharyngeal angiofibroma is highly vascular, uncapsulated and locally invasive tumor. Its incidence is 0.05% of all head and neck neoplasms as per many study reports [1]. The exact site of origin is still unclear. The postero-superior margin of the sphenopalatine foramen or from the contents of the distal vidian canal or vascular malformation resulting from incomplete regression of the first branchial arch artery [2]. A good number of cases reported to our department, Department of Otolaryngology Assam Medical College and Hospital, Assam, India. Since the department caters to the need of most of the people residing in the Upper-Assam region of India, it can be well said that a changing trend has been seen in the incidence of the disease in recent times. Most of patients present with nasal obstruction and bleeding from nose. The presenting symptoms are severe, recurrent epistaxis with persistent nasal obstruction, facial deformities, proptosis, blindness, and cranial nerve palsies. Diagnosis based on a careful history and nasal endoscopic examination, supplemented radiological study. MRI is more accurate than CT in assessing intracranial extension [3]. Biopsy and pre-op histological diagnosis are contraindicated and definitive diagnosis is established by angiography. Surgery is the main modality for this tumor. The treatment for the nasopharyngeal angiofibroma, most notably is concerned with the management of bleeding and hence the subject has stimulated good interest [4].
Materials and Methods
The study is a retrospective. We have highlighted the changing trend in the epidemiology, pathogenesis, management and post-operative care including radiotherapy. A note should be taken about the actual scenario that is trending. In a span of one year (July 14- June 15) there has been alarming reporting of fifteen cases of which one recurred thrice. Out of fifteen patients thirteen were of age group 12- 19 years and two were of age group 20-30 years. 80% were of either Stage III or Stage IV (Fisch grading). Different approaches for surgery were used. The recurrence rate was 6.7%. The patients are on continuous follow up.
Results
Epidemiology
A total of 21840 cases visited opd during the study period. Out of it 3276 were of the risk age group and 585 were of head and neck neoplasm which were admitted. Out of 585 diagnosed cases of head and neck neoplasms 15 cases were of juvenile naso- pharyngeal angiofibroma. It was a study of fifteen patients in a period of one year.
100%
95%
90%
85% Series 2
80% Series 1
75% Figure 2: Category 1 Shows Opd Cases, Category 2 Shows risk group attended Opd for any cause, Category 3 Shows total risk group admitted for any cause.
100%
| Seri Seri | ||||
Figure 3: Calculation of Incidence: Total No. of New Cases (15) X 1000 = 0.37% Population at Risk (40317) Category 1 Shows Rest Of World Category 2 Shows Upper Assam All the patients were of the age group 12- 30 years. Tinsukia reported the highest with 46.67% cases and Golaghat reported the lowest with 6.67%. Total population at risk of this district is 40317. The incidence calculated was 0.37% which has raised 0.32% from 0 .05% (Figure 1-3). Environment: All the above mentioned districts are generally same as far as environment is concerned and all have a specific period of dry, hot and dusty weather during similar period of a year. Hormonal: All the cases except two were growing children during their pubertal period of life.
Pathogenesis
There is marked predilection for adolescent boys, with a peak at approximately 15 years of age [5]. Although the hormonal and the distal vidian canal theory are the most widely accepted ones, there still raises the question as to why only that specific part is involved and also why only during the pubertal spurt, that also in a limited number of similar patients. The theory of origin from vascular malformation in relation to pubertal growth is a promising one and should be widely accepted. Stage Distribution: The patients in the study were distributed into the following stages I 0% II 20% III 53.33% IV 26.67%
Treatment modalities
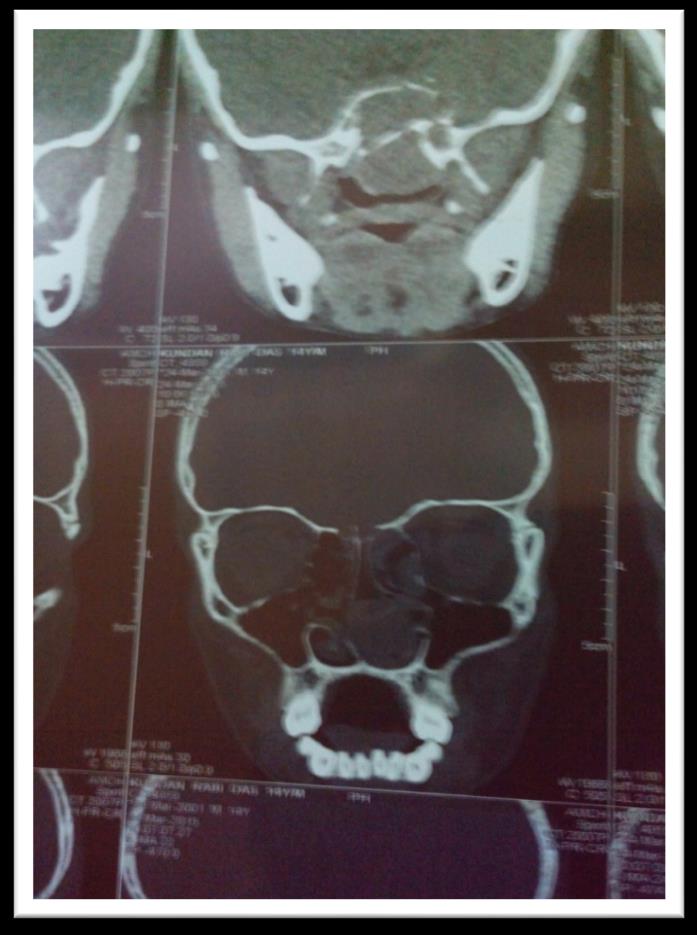
All cases were treated by surgery. All patients were properly planned for operative procedures. All routine investigations were done etc. Apart from these tests a CT scan, MRI, and CT Angiogram were performed. In Figure 4 we can see that there is an ill defined lobulated heterogeneously enhancing soft tissue density lesion completely filling the left nasal cavity, causing widening of the sphenopalatine foramen and extending into pterygopalatine and infratemporal fossa and causing pressure effect on right Eustachian tube opening. None of the patient received adjuvant radiotherapy [6]. The prime anaesthetic concern in the resection of JNAs is prevention of the aspiration of blood, minimization of blood loss and prevention of airway obstruction in the postoperative period owing to surgical manipulation. All patients were taken proper anaesthetic care in a regular manner. Premedication was done by Ondansetron, Glycopyrolate and Tramadol. Induction by Propofol and muscle relaxant for maintenance by Vecuronium. Reverse and extubate with Neostigmine and Glycopyrolate when patient was awake and responding to verbal commands. Figure 5 shows that the mass is removed by transpalatal incision.
Outcome
All the patients presenting to the department were male of age group 12-30. All patients received surgical treatment. Only one case was operated endoscopically. One case was operated by lateral rhinotomy and he was in

Stage IV. The rest by transpalatine and both transpalatine and transnasal approach. No recurrence was found in fourteen cases. One of the patient was operated thrice after twin recurrence. There were no complications during the treatment period. It was seen that the ratio of the interpupillary distance to that of the distance between the nasion and the nasal tip was almost 0.7 in all the cases and in a newer discovery we named it as “Tiwari’s Ratio”.
Discussion
Angiofibromata often grow and extend along natural foramina and fissures, displacing and distorting the adjacent areas as they expand. Collateral blood supplies develop. The tumors spread to pterygopalatine fossa through the pterygomaxillary fissure. They can also extend along the inferior orbital fissure. Continued tumor expansion causes pressure over the sphenoid. This brings the tumor against the Dura [7]. Surgical resection is the recommended modality of treatment. There is now availability of different modalities for pre-op reduction of bleeding; however, management of JNA still poses a great challenge. Adequate exposure reduces morbidity and mortality. Even tumors extending to pterygopalatine fossa are managed through the transpalatine approach in experienced hands [8]. The study previously on juvenile nasopharyngeal angiofibroma shows it is rare and its incidence is 0.05%. However in this study it was seen that there should be a rise in the incidence as within a span of one year and with increase in the number of cases. The incidence calculated was 0.37% which has raised 0.32% from 0 .05%.
Conclusion
Surgery remains the mainstay of therapy. Newer advances in technology like endoscopic removal should be limited to earlier stages. The management, pre- operative care, surgical management and post-operative care including radiotherapy should be properly planned.
References
-
Gullane PJ, Davidson J, Dwyer T, Forte V (1992) Juvenile angiofibroma: a review of literature and a case series report. Laryngoscope 102(8): 928-933.
-
Schick B (2009) Current aspects of angiofibroma. ENT News 17(6): 67-69.
-
Lloyd G, Howard D, Phelps P, Cheesman A (1999) Juvenile angiofibroma: modern imaging and its influence on the surgical treatment of juvenile angiofibroma. J Laryngol Otol 113(2): 43-44.
-
Naresh KP, Gaurav G, Suresh S, Ashok Gupta (2012) Nasopharyngeal Angiofibroma-changing Trends in the Management. Indian J Otolaryngol Head Neck Surg 64(3): 233-239.
-
Neel HB, Whicker JH, Devine KD, Louis HW (1973) Juvenile angiofibroma: Review of 120 cases. Am J Surg 126(4): 547-556.
-
Khanna P, Ray BR, Sinha R, Kumar R, Sikka K, et al. (2013) Anaesthetic management of endoscopic resection of juvenile nasopharyngeal angiofibroma: our experience and a review of the literature. South Afr J Anaesth Analg 19(6): 314-320.
-
CT Chew Angiofibroma. Scott Brown’s Diseases of the Ear Nose Throat 4: 23-27.
-
Pippal SK, Khare M, Yashveer B (2011) A Study on Reliability and Safety of Transpalatine Approach for Nasopharyngeal Angiofibroma: A Case Series. World Articles in Ear Nose Throat 4-1.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?