Therapeutic Management of Epistaxis in CHU Yalgado Ouedraogo
Objective: The objective of this study was to report the treatment results of epistaxis in our practice. Materials and Methods: This is a prospective study over a period of one (01) year from January to December 2015, wearing on 264 patients received and supported for epistaxis in the ENT and Neck of facial Surgery Department in CHU Yalgado Ouedraogo of Ouagadougou. Results: The epistaxis represents 15% of emergency in the service. The average age of onset was 30.8 years with extremes ranging from 2 months to 80 years. We noted 213 (80.7%) adults and 51 (19.3%) children. The subjects of male sex represented 194 cases (73.5%) and female sex 70 cases (26.5%). The epistaxis was anterior in 90.1% of cases, unilateral in 56.8% of cases and severe in 40. 2% of cases. The commonest causes of epistaxis were locoregional (45.8%), dominated by the trauma of the facial structure (33%). The benign tumors represented 2.2%, and malignant tumors 1.6% of the workforce. The arterial hypertension (14%) was the commonest general cause. Non surgical measures have been the main methods of intervention in 98.5% of cases. The treatment had essentially consisted in anterior nasal packing (80.3%) and the etamsylate administration (75%). We observed 5.8% of complications. The death rate was 5%. Conclusion: Epistaxis, hemorrhagic emergency ENT, is common in our practice. The causes are diverse, dominated by locoregional causes. The epistaxis is serious and unpredictable evolution hence the need to initiate a consequent resuscitation.
Introduction
The epistaxis represents one of the most common emergencies encountered in the daily ENT practice [1]. They can affect up to 60% of the population, with 6% requiring medical care [2]. Generally benign, they are by their abundance or repetition to put sick life threatening [3, 4]. Their management should be both symptomatic and etiological. It is codified in Western countries [1, 3, 4]. The African literature is relatively poor on the subject. Across this the present study, it is to report our experience in the therapeutic management of epistaxis in the ENT and CCF department in CHU Yalgado Ouedraogo.
Material and Methods
This is a prospective study over a period of 1 year, from January to December 2015 in the ENT and Cervicofacial Surgery department of CHU Yalgado Ouedraogo of Ouagadougou. Thus, 264 cases of epistaxis were examined. Were included in the study, any patient regardless of the age and sex received in emergency, in consultation or hospitalization in the service. Data were gathered starting from questionnaires sheets during direct interviews with patients. The admission registers, clinical records of disease and the notebooks’ operative report were also used as source data. The study variables were socio demographic characteristics (age, sex, and history), clinical manifestations (abundance, seat, anatomical localization of the bleeding site, repetition), the causes of epistaxis, aspects therapeutic. The anonymity and confidentiality of data has been respected. The study protocol was approved by the ethics committee. The patients were hypertensive known, diagnosed in cardiology but irregularly followed or not known. The blood pressure was taken on two occasions in supine position and sitting at 15 minute intervals, preceded by a rest period of 10 minutes using a manual blood pressure monitor. Initially the epistaxis was classified in small abundance, mean abundance and great abundance. But today the current trend class in epistaxis benign with no sign of impact, serious with repercussions signs. We opted for the second classification. Only the patients with a hemoglobin lower or equal to 6 g / dl have benefited a blood transfusion.
Result
| Effective (n) | Percentage (%) | |
|---|---|---|
| Locoregional | 121 | 45.8 |
| Traumatic | 87 | 33 |
| Rhinosinusitis | 11 | 4.1 |
| Sinonasal tumors | 10 | 3.8 |
| Foreign bodies | 7 | 2.6 |
| Iatrogenic (surgery, medications) | 6 | 2.3 |
| General | 48 | 18.2 |
| High blood pressure | 37 | 14 |
| hematological disease | 6 | 2.3 |
| Pregnancies | 3 | 1.1 |
| Typhoid fever | 2 | 0.8 |
| Idiopathic or essential | 95 | 36 |
Table 1: The causes of epistaxis.
Table 1: The causes of epistaxis. According to the site of bleeding, the epistaxis was anterior in 238 cases (90.1%), posterior in 10 cases (3.8%), anterior and posterior in 16 cases (6.1%). She was unilateral in 150 cases (56.8%) and bilateral in 114 cases (43.2%). According to the seriousness, the epistaxis was benign in 158 cases (59.8%) and severe in 106 cases (40.2%) of which 6.8% (18 cases) very severe. with signs of shock. Therapeutically, the non-surgical measures have been the main methods of intervention in 98.5% of cases. All patients received a treatment referred to local hemostatic and / or general. The local hemostasis was constituted by an anterior nasal packing in 80.3% of cases. The general hemostasis was essentially constituted by parenteral administration (72 hours) then oral of etamsylate in 75% of cases. Surgical measure was carried out in 1.5% of cases essentially constituted by resection of sinonasal tumors. Treatment modalities are summarized in (Table 2).
| Therapeutic modalities | Effective (n) | Percentage (%) |
|---|---|---|
| Local hemostasis | ||
| Anterior nasal packing | 212 | 80.3 |
| Digital compression | 32 | 12.1 |
| Unspecified treatment | 20 | 7.6 |
| GeneralHemostasis | ||
| Etamsylate | 198 | 75 |
| Tranexamic acid | 61 | 23.1 |
| Association of 2 | 7 | 1.9 |
| Surgical hemostasis | ||
| Endonasal excision of tumor | 4 | 1.5 |
Table 2: Treatment modalities.
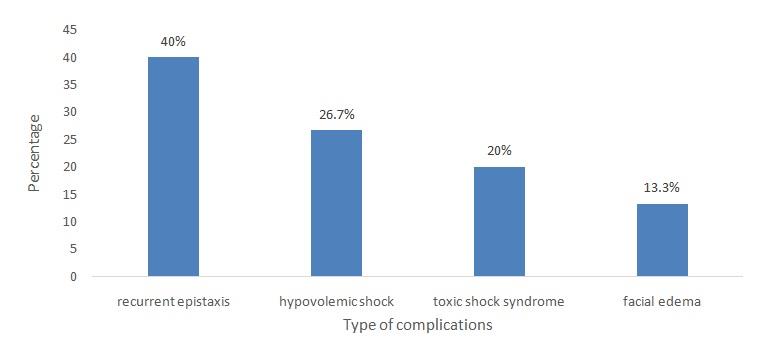
In our series, there has been no posterior nasal packing nor of cauterization, nor of embolization nor of ligation of blood vessels, because of the inadequacy of the technical platform. The transfusion of whole blood was required in ten (10) patients i.e. 3.8% of cases. Four (4) patients 1.5% was admitted to intensive resuscitation. Those are the patients who had hemoglobin lower or equal to 6 g / dl, who received a blood transfusion. The prophylactic antibiotics were prescribed in 36% of our patients. The evolution was marked by 04 types of complications in 15 patients or 5.7% of complications (Figure 1). Among these complications, the recurrent epistaxis was the most common with 40% of cases. The average duration of stays in hospital was 7.6 days with extremes of 1 to 30 days. The evolution after treatment was favorable in 95% of cases. Thirteen (13) patients died either a rate of 5% of mortality. Three (03) died in an array of toxic shock syndrome, four (04) in an array of hypovolemic shock in trauma of the face associating a trauma of the skull and six (6) by anemia in an array of recurrent epistaxis due to various causes (nasopharyngeal carcinoma, hemopathies, typhoid fever).
Discussion
The epistaxis is a common ENT emergency 15% of emergency ENT [3, 4]. Our results corroborate those in the literature. In our practice, the epistaxis is above all the fact of young adults. The average age of our patients was 30.8 years. The young age of the patients was also noted by African authors [2, 5, 6]. Our results are different from those of Western authors [4, 7, 8, 9] who showed that the epistaxis is a geriatric problem affecting the subject of average age of about 60 years. In our series, the young people are exposed of the trauma of the face by accident of the traffic, since they are device users with 2 wheels for their daily traveling. We noted a male predominance (73.7%) with a sex ratio of 1.8. This male predominance make unanimous of the authors [2, 5, 6, 10, 11]. The men exercise the more often of the occupations that expose them of the trauma. The main etiology of epistaxis varies by series. In our study, the etiology the most incriminated in the occurrence of epistaxis is the cause locoregional 45.8% of cases with in head the trauma facial bones 33% of cases. This etiological factor was followed by the epistaxis so- called essential 36% of cases. This same observation was made in the African series [2, 5, 6] and in some Western studies [7, 10, 12]. This high rate of idiopathic epistaxis could reflect the limit of etiological investigations. Any epistaxis without obvious cause has been retained as idiopathic epistaxis in our series. Other factors that of essential epistaxis are then to look for: the scratching of the nose, the sun exposure, the physical exertion. The high blood pressure (hypertension) was the third cause in our series. It translates a poor control of blood pressure. This
is in agreement with a Nigerian report on not controlled hypertensive patients (treatment discontinuation antihypertensive) showing epistaxis [13]. The management of epistaxis is well summarized and codified in a secular saying: resuscitate the patient, establish the site of bleeding, stop bleeding and treat the cause of epistaxis [14]. The aim of treatment is to stop the bleeding, to ensure a good hemodynamics and prevent complications [9, 14]. There is controversy regarding the treatment that will be the best adapted to achieve those objectives. The modalities of treatment can be separated into two groups: non-surgical or conservative’s interventions and interventional or surgical approaches. The non-surgical approach has been reported to stop bleeding in more than 80-90% of cases [15]. The anterior nasal packing was the commonest treatment modality of treatment in this present study and that of certain authors [16, 17]. This form of treatment would be effective in some centers in Nigeria [18]. Moreover, the effectiveness of posterior packing and probes at double-balloon is variously appreciated in the literature, ranging from 74 to 90% of cases [4, 19]. In our context, no cases of posterior nasal packing have not been carried out because the anterior nasal packing has always been sufficient. But sometimes the anterior nasal packing exposes the staff to the risk of blood accident. The authors [2, 14, 15] then recommend universal precautions (face mask with shield, hair cover, double gloving, glasses) for all personnel of care of health involved in the management of these patients. The etamsylate was the general hemostasis the most used due to its geographic availability, and its financial accessibility. However, its formal input in the control of hemostasis remains to be demonstrated by hematological studies. The rate of blood transfusion in our study (3.8%) is lower than that reported in the literature which falls between 6.92 to 15.1% [2]. It reflects the severity of epistaxis. However, the ideal is the transfusion of packed cells (PRBC). The use of antibiotic prophylaxis after an anterior nasal packing is controversial. Most authors [14, 20] recommend the use of prophylactic antibiotics because of the risk of infectious complications such as sinusitis, toxic shock syndrome. In our study, it was used in 36% of cases. For our part, the aseptic realization of this nasal packing do not put immune to the infection. The rate of mortality in our study was 5%. It is superior to those reported by some authors [2, 11, 13]. This rate is inherent at the etiology of epistaxis. Indeed, the nasopharyngeal cancers are deadly in our practice because of the insufficient of technical platform of supported. Also the absence of a service of therefore reanimation explains the deaths of some trauma to the face associating a skull trauma. We agree with DUVAL [4] that the epistaxis is the most common symptom and the most worrisome of bleeding emergencies ORL, responsible for 10 to 25% of mortality.
Conclusion
The epistaxis is potentially serious. It can be life- threatening patients by its abundance and repetition hence the necessity to coordinate the actions of management: treat emergency while researching in parallel the etiology for efficient management.
References
-
Herman P (2000) Epistaxis. Orientation diagnostique et prise en charge. Rev Prat 50(17): 1959-1964.
-
Japhet M Gilyoma, Phillipo L Chalya (2011) Etiological profile and treatment outcome of epistaxis at a tertiary care hospital in Northwestern Tanzania: a prospective review of 104 cases. BMC ear, nose and throat disorders 11: 8.
-
Dufour X, Lebreton JP, Gohler C, Ferrié JC, Klossek JM (2010) Epistaxis, EMC (Elsevier Masson SAA, Paris) Otorhinolaryngologie 20-310-A-10.
-
Duval G, Herman P (2003) Urgences ORL, épistaxis et autresurgenceshémorragiques ORL, 03_confMed_SFMU8LC, P12.
-
Boko E, Goune L, Kpemissi E (2006) Epidémiologie et étiologies des épistaxis dans notre pratique: A propos de 250 cas colligés de 1986 à 1997 au CHU de Lomé. Journal de la recherche scientifique de l’université de Lomé 8(1).
-
Badou KE, Melleu LV, M’pessa EM (2013) Aspects épidémiologiques des épistaxis au CHU de Yopougon Rev Int Sc Méd 15(1): 9-11.
-
Pallin DJ, Chang Y, Mc Kay MP, Emond JA, Pelletier AJ, et al. (2005) Epidemiology of epistaxis in USA emergency departments, 1992 to 2001. Ann Emerg Med 46(1): 77-81.
-
Walker TWM, Caefarlane TV, Mc Garry GW (2007) The epidemiology and chronobiology of epistaxis: an investigation of Scottish hospital admission 1995- 2004. Clin Otolaryngol 32(5): 361-365.
-
Varshney S, Saxena RK (2005) Epistaxis: a retrospective clinical study. Indian Journal of Otolaryngology, Head Neck Surgery 57(2): 125-129. $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$
-
Payen JF, Bettega G (1999) Les traumatismes maxillofaciaux. Conférences d’actualisation, SFAR Elsevier Paris 705-719.
-
Eziyi JAE, Akinpelu OV, Amusa YB, Eziyi AK (2009) Epistaxis in Nigerians: A 3-year Experience. East Cent Afr J Surg 14(2): 93-98.
-
Messner AH (2011) Epidemiology and etiology of epistaxis in children. Essentials of emergency medicine 82: 472.
-
Iseh KR, Muhammad Z (2008) Pattern of epistaxis in Sokoto, Nigeria: A review of 72 cases. Ann Afr Med 7(3): 107-111.
-
Daudia A, Jaiswal V, Jones NS (2008) Guidelines for the management of idiopathic epistaxis in adults: how we do it. Clinical Otolaryngology 33: 607-628.
-
Rodney JS (2009) Epistaxis: A clinical experience. New England Journal of Medicine 360: 784-789.
-
Harkani A, Ziad T, Rochdi Y, Nouri H, Aderdour L, et al. (2012) L’épistaxis aux urgences: à propos de 140 cas. 129: A103.
-
Bouchareb N, Barhmi S, El hani L, Abada R, Rouadi S, et al. L’épistaxis aux urgences : à propos de646 cas P034.
-
Mgbor NC (2004) Epistaxis in Enugu: A 9 year Review. Nig J of Otorhinolaryngology 1(2): 11-14.
-
Schaitkin B, Strauss M, Houck JR (1987) Epistaxis: medical versus surgical therapy; a comparison of efficacy, complications, and economic considerations. Laryngoscope 97(12): 1392-1395.
-
Biswas D, Wilson H, Mal R (2006) Use of systemic prophylactic antibiotics with anterior nasal packing in England, UK. Clin Otolaryngol 31(6): 566-567.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?