Epidemiological Clinical Profile and Management of Nasal Masses of Vascular Origin: About 10 Cases
Abstract: Vascular tumors of the sinonasal cavities are rarely documented in the literature. They are characterized by a histological diversity. They can be benign or malignant. The most common histologic type is the hemangioma. Their management is not well codified, it has benefited from advances in modern imaging and endoscopic surgery. The objective of the study was to investigate their clinicopathological characteristics, treatment and results.Patients and methods: Observations of 10 vascular tumors of the nasal cavities collected between January 2014 and July 2016 were reviewed retrospectively.Results: The average age was 25.4 years, male dominance was marked with a sex ratio of 4. The epistaxis was the sign main developer (100%). All tumors were benign with predominance of hemangioma (4 cases), followed angiofibroma of the partition (3 cases) and nasopharyngeal fibroma (3 cases). All patients were operated by endonasal in 7 cases / 10 and transfacial track in 3 cases. Embolization was performed in 5 patients; it was of hemangiomas 2 and 3 nasopharyngeal fibroids. No cases of recurrence were noted to date.Conclusion: Vascular tumors of the nasal cavity are difficult to treat, especially when they reach a large volume and at an extension to adjacent areas, making the delicate and bleeding surgical procedure. The use of selective embolization in these cases proves mandatory.
Introduction
Vascular tumors of the sinonasal cavities are rarely documented in the literature. They are characterized by a histological diversity; benign tumors are the most common. The most common histologic type is the hemangioma. These tumors are hyper-vascularized and can be high sometimes destructive potential life- threatening deluge epistaxis, intracranial extension or intraoperative bleeding. Advances in medical imaging (CT, MRI, selective angiography) revolutionized diagnostic and therapeutic approach to this entity.
Patients and Methods
The observations of 10 patients undergoing vascular tumor of the nasal cavities collected between January 2014 and July 2016 were reviewed retrospectively. The management of these tumors based on nasal endoscopy, imaging, angiography and some for embolization. The epidemiological, histopathological, clinical, treatment and outcome were investigated.
The objective of Our Work
We report 10 cases of vascular tumors of the nasal cavities pit through which it seemed interesting to clarify the different histological, clinical and laboratory of these tumors and finally the current literature data about their surgical approach.
Results
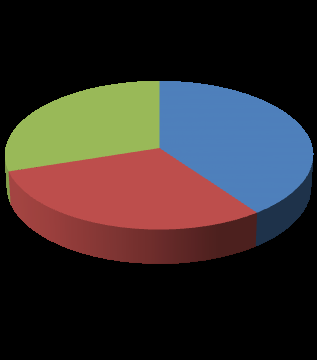
haemangioma
30%
40% angiofibroma
30% nasopharyngeal fibroma Figure 1: Distribution of vascular tumors of the nasal fossae according to their histology.
Histology
Vascular tumors accounted for 39% of benign tumors of the FN, followed papillomas 25%. 3 histological types: Predominantly hemangioma (4 cases), followed angiofibroma of the nasal septum (3 cases) and nasopharyngeal fibroma (3 cases) (Fig 1). SEX: male predominance. The sex ratio=4. The average age: 25.4 years (12-68 years). Fibroma nasopharyngeal and angiofibroma selectively touched young adults. Signs: The epistaxis was the major telltale sign for all tumors (100%).
| Nasopha | Angiofibro | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hemang | ||||||||||||
| Clinical signs | ryngeal | ma of the | ||||||||||
| ioma | ||||||||||||
| fibroma | septum | |||||||||||
| Epistaxis | 4 | 3 | 3 | |||||||||
| Nasal | 2 | 3 | 1 | |||||||||
| obstruction | ||||||||||||
| Rhinorrhea | - | - | - | |||||||||
| Facial pain | - | 2 | 2 | |||||||||
| Nasal vestibule | - | - | 2 | |||||||||
| mass | ||||||||||||
| Facial | - | 1 | - | |||||||||
| Deformation | ||||||||||||
| Expansion | - | - | - | |||||||||
| intra sinus sign | ||||||||||||
| Table 1: Clinical signs according to the histological type. | ||||||||||||
| Paraclinical |
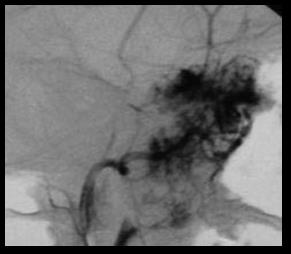
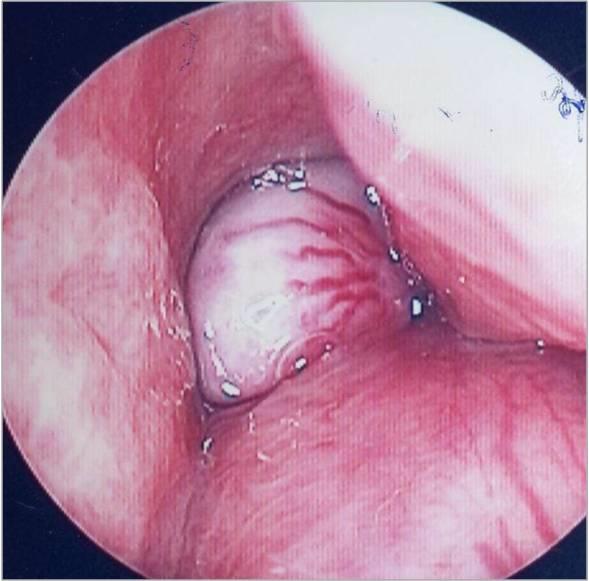
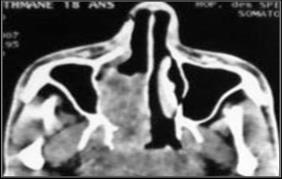
Rhinocavoscopy: performed in all patients. No patients received biopsy. All patients underwent a CT scan of the sinuses. The MRA was performed in 2 patients with nasopharyngeal fibroids and arteriography in 5 patients: 3 nasopharyngeal fibroids and 2 hemangiomas (Figure 2-5).



Treatment
| Endonasa | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| l Surgical | |||||||||||
| Approach | |||||||||||
| Transfaci | Embolizati | ||||||||||
| es Under | |||||||||||
| al Way | on | ||||||||||
| Endoscop | |||||||||||
| ic | |||||||||||
| Guidance | |||||||||||
| Hemangioma | 3 | 1 | 2 | ||||||||
| Nasopharyng | 1 | 2 | 3 | ||||||||
| eal fibroma | |||||||||||
| Angiofibrom | 3 | - | - | ||||||||
| a of the | |||||||||||
| septum | |||||||||||
| Total | 7 | 3 | 5 |
Discussion
Vascular tumors of the sinonasal cavities are rare tumors. They are in most cases benign.
Epidemiology
The most frequent tumors are capillary hemangiomas, followed by NPF, cavernous hemangiomas, angiofibroma of the nasal septum, paraganglioma and low grade angiosarcoma. The hemangiopericytomas are rare [1, 2].
Seat
Capillary hemangiomas: from triangle Kiesselbach. Cavernous hemangiomas: from the side wall of the nasal cavity and reach cones. FNP: originates on the periphery of the sphenopalatine foramen. Angiofibroma of the nasal septum: The original site is often the septal cartilage [3] at the vascular spot.
Age
Capillary hemangiomas: young age. Hemangiomas: adult (4th and 5th decade). Angiofibroma of the nasal septum: Adolescents 14-17 years and patients over 40 years [4]. FNP: exclusively in adolescents between 7 and 25 years [5, 6].
Clinical
Symptom common: unilateral epistaxis and nasal obstruction. At endoscopy: red, purple lesions, or sometimes white as the NPF. Sessile or pedunculated, easily bleeding at the slightest trauma. Vascular tumors are sometimes covered with whitish necrotic tissue making it difficult to distinguish with other nasal tumors (inverted papilloma).
Extension of tumor
Endonasal form development: Sphenoid and maxillary sinuses +++ Side extension form: •in front of the pterygoid process, • behind the process pterygoid Shaped lower extension to the parapharyngeal spaces with cervical extension Shape intracranial extension cribrosa, jugum, sphenoid wing, enlargement a foramen of the skull base.
Paraclinic
The enhanced CT PDC can confirm the vascular nature of the mass: tissue density lesion is enhanced after injection of PDC. CT determines the exact location and extent of the tumor: FIT, sinus, intracranial extension, and specify the existence of bone destruction. At MRI: discrete mass hypo signal in T1. T2: heterogeneous aspect. After gadolinium injection: intense and early enhancement of tumor signal, reflecting the hypervascular nature of the tumor. MRI allows a better assessment of tumor extension: guide the choice of surgical approach. It allows distinguishing between sinus invasion and retention. The arteriography can explore the different pedicle feeding the tumor and a second time to embolization before surgery (2 or 3 days before) to reduce blood loss intraoperatively and allow draining the tumor. This is often the internal maxillary artery, ascending pharyngeal and facial. Two methods of embolization: -Endovascular embolisation . -Percutaneous embolisation by direct injection of sclerosing product intratumoral. The degree of devascularization obtained depends essentially the size of the tumor.
Treatment
Goal: complete resection of the tumor with minimal blood loss (prior embolization), resulting in the least possible sequelae, and avoiding relapses. The choice of the route first: depending on the location, volume and the extent of the tumor, and on the experience of the surgical team. For strictly nasal tumors, endonasal approach is favored by endoscopy. For large tumors transfacial way Nasal Hemangiomas: wide excision carrying the tumor, the mucous membrane and the underlying perichondrium. For angiofibromas septum: excision taking the basis of cartilage implant in order to avoid recurrence [6]. Other therapeutic methods: cryotherapy and laser YAG: if extensive tumors.
Conclusion
The therapeutic treatment of vascular tumors benefited many of the development: - Imaging: early diagnosis specifying the morphology and extent of the tumor;
- Embolisation: dry the tumor before the procedure; - Endonasal surgery under endoscopic guidance: Allows a less invasive and more precise surgery.
References
-
Fu YS, Perzin KH (1974) Non-epithelial tumors of the nasal cavity, paranasal sinuses, and nasopharynx: a clinicopathologic study. I. General Features and Vascular tumors. Cancer 33(5): 1275-1288.
-
Perez-Ordonez B, Huvos AG (2001) Nonsquamous lesions of nasal cavity, paranasal sinuses, and nasopharynx. In: Gnepp DR, et al. (Eds.) Diagnostic surgical pathology of the head and neck, 1st (edn), WB Saunders Company pp: 79-139.
-
Lazar CC, Costentin B, François A, Marie JP, Dehesdin D (2004) Bleeding polyp" of the nasal septum: an uncommon lesion in adults. Ann Otol Rhinol Laryngol. 113(8): 652-654.
-
Legent F (1986) Epistaxis - EMC. ORL (3) 20310 A 10.
-
S Oueslati, OB Gamra, S Kharrat, S Sassi, N Milka, et al. (2008) Le fibrome nasopharyngien: à proposde 15 cas traités par embolisation Journal de Radiologie 89(5-C1): 579-584.
-
François Legent ORL: pathologie cervico-faciale. Pathologie de la cloison nasale. P1203.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?