Malignant Degeneration of Oral Condyloma Acuminatum
Background: Condyloma acuminatum is considered to be a benign lesion of oral cavity; in comparison to its anogenital counterpart which carries a significant malignant potential. Oral condyloma acuminatum lesions have not been reported in literature to undergo malignant change. Methods: A 47 year old patient presented with a rapidly progressive proliferative mass in oral cavity infiltrating the skin. He was operated earlier for excision of tumour at same site which was diagnosed as condyloma acuminatum. Results: This case study shows that there may be a potential risk of malignant degeneration for oral condyloma acuminatum to oral squamous cell carcinoma in long term. Conclusion: An oral condyloma acuminatum patient need to be followed up regularly for long time to detect potential malignant transformation and larger prospective study is required to establish its malignancy potential and/or annual transformation rate.
Introduction
Oral squamous papilloma (OSP) and Condyloma acuminatum are both benign lesions of oral cavity and has been associated with Human Papilloma Virus (HPV). OSP can present as single or multiple pedunculated or nodular lesions. Multiple and recurrent lesions are usually seen in children and immune compromised adults while immune competent adults usually present with a solitary papilloma [1]. They are most commonly seen in tongue followed by palate, lip, labial commissure and rarely buccal mucosa. Although, any site in oral cavity or oropharynx can be involved and present as mostly pinkish or whitish papillary projection [2]. Oral Condyloma often occurs in labial mucosa, tongue and floor of mouth. Lesions are usually sessile or pedunculated and can have satellite nodules, usually seen in third or fourth decade of life [3]. HPV association has been reported in both these benign conditions. Most commonly subtype 6 and 11 has been documented in these lesions. Small risk of malignant degeneration of OSP has been documented in literature [2]. Though malignant degeneration of condyloma acuminatum in ano-genital region has been reported in the literature; [4] malignant degeneration of condyloma acuminatum in oral cavity is not reported so far. We came across a case wherein a patient had squamous papilloma, condyloma acuminatum and squamous cell carcinoma of left buccal mucosa sequentially in a span of 10 years. The purpose of reporting this case to share this unusual sequence of pathology at a single site and to discuss whether it is a natural history of HPV inflicted lesions or malignant transformation of condyloma acuminatum.
Case History
Forty seven year old male patient resident of Uttar Pradesh, India presented to us in the clinic with progressive lesion of oral cavity for last 4 months. The lesion was painful and rapidly progressive in nature. On examination, it was involving left buccal mucosa, gingiva- buccal sulcus, mandible, tongue, floor of mouth and skin over left cheek with active pus discharge. Patient had limited mouth opening and progressive dysphagia to solids. The lesion (Figure A.1, A.2, A.3, A.4) was approximately 6 x10cm over cheek and 2 x 7 cm in submandibular region. Radiologically (Figure B.1,B.2,B.3,B.4,B.5) there was a heterogeneous lesion in left retromolar trigone infiltrating infratemporal space with involvement of lateral and medial pterygoid as well erosion of lateral wall of maxillary sinus and extension into the maxillary sinus. It was seen extending to base of tongue, lateral wall of oropharynx and parapharyngeal space. Left side level Ia (1x2cm), Ib (3x2cm) and right side level IV (2x1cm) lymph nodes were palpable and fixed. There were no co-morbidities like diabetes mellitus or hypertension. Viral markers for HIV, Hepatitis B & C were negative. He worked as a farmer and had strong history for addiction to smoking (2bidis/day), tobacco chewing and occasional alcohol intake since last 25 years. While evaluating the patient, there was past history of surgery in oral cavity two times. Medical records available with the patient showed that he underwent surgeries in year 2005 and 2010 for lesion in left buccal mucosa. In year 2005, wide local excision of a pedunculated papilloma on left buccal mucosa was done which was histopathological confirmed as squamous papilloma. After 5 years of recurrence free interval; in 2010, patient presented with cauliflower like lesion of approximately 35mm x 33mm in left buccal mucosa with enlarged lymph node in left level II. Contrast enhanced computed tomography (CECT) scan of face showed heterogeneous mass in left buccal space reaching upto upper gingivo-buccal sulcus without any erosion in maxilla or mandible. He underwent wide local excision with neck dissection with pectoralis major myocutaneous flap (PMMF) repair in a tertiary care centre. The final histopathology reported was 5x4x2 cm cauliflower like growth in buccal mucosa; cut surface of growth was solid greyish –white. There was parakeratosis, hyperkeratosis and papillomatosis associated with koilocytic changes. The mucosal margins were free but close to tumour, deep resected margin was free of tumour. Six lymph nodes showed reactive hyperplasia in neck specimen. Histology suggested condyloma acuminatum. No HPV testing was done. The biopsy from the present lesion was reported to be consistent with squamous cell carcinoma (Fig C.1, C.2). As per AJCC staging system, it was T4b disease and thus unresectable. The decision of best supportive care in term of pain management and enteral feeding through Ryle’s tube was consensus by the tumour clinic. Debulking surgeries for locally advanced disease is not a part of our management protocol.
A1 A2
A3 A4
Figures A.1-A.4: Clinical photographs of the case showing ulceroproliferative growth in oral cavity with skin infiltration.
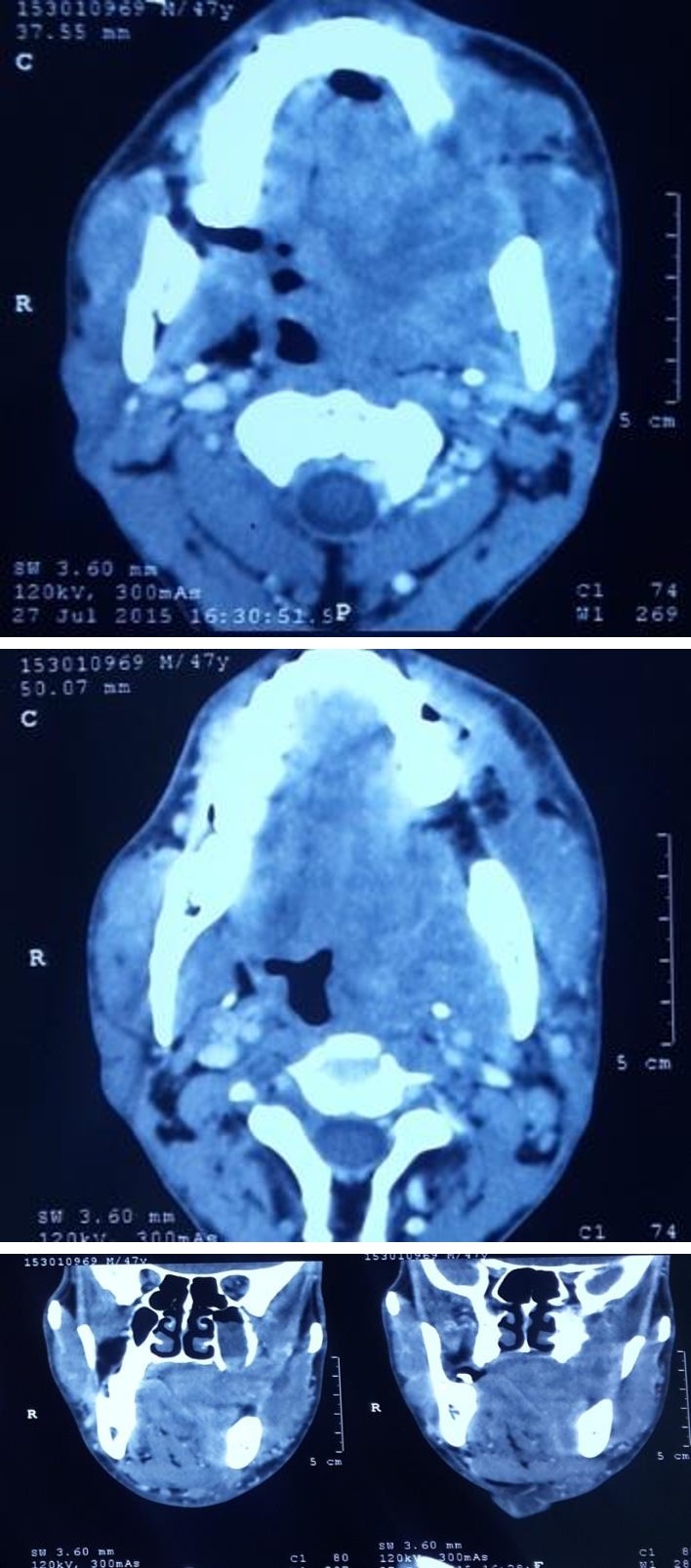
B1 B2
B3
B4 B5
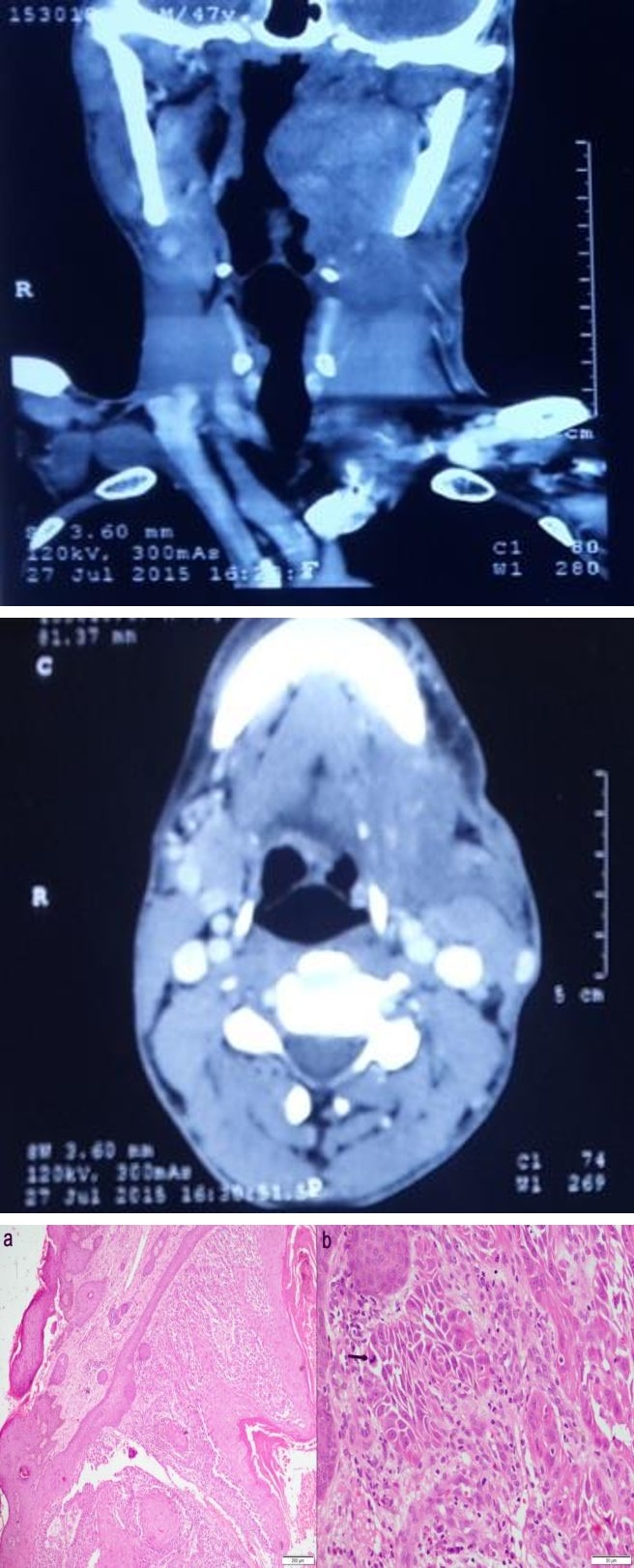
Figure B.1-B.5: Contrast enhanced CT scan face and neck of patient showing heterogenous mass in oral cavity, oropharynx, masticator space, parapharyngeal space extending to maxillary sinus and infratemporal fossa.
C1 C2
Figure C1 C2: Haematoxylin and eosin (HE) section shows squamous epithelial cell proliferation in groups and sheets in deep dermis (C.1, 40x). The tumor cells are polygonal with vesicular nuclei, prominent nucleoli, moderate eosinophilic cytoplasm and presence of intercellular bridge at places. Mitotic activity (arrow) was noted (C.2, HE; 200x).
| Discussion |
There is enough literature pertaining to established association of condyloma acuminatum with ano-genital cancer [4, 5, 6]. It has been reported to have 10-fold increased risk of cancer of the vulva and vagina among women, and anal cancer amongst both men and women in patients with condyloma acuminatum [4]. In cervix there is no significant excess risk of invasive cancer, whereas the risk of carcinoma in situ is almost doubled [4]. In contrast, malignant degeneration of oral condyloma acuminatum has not been reported in literature to best of our knowledge [4, 7, 8, 9, 10]. Condyloma acuminatum is usually seen in sexually active individuals especially with multiple partners. HPV infection is now known to be common in sexually active people with prevalence of subclinical infection in almost 15% [5]. In our case, patient was married with history of single partner. Although due to social taboo in India, history of multiple sexual partners and of oral sex is often not revealed by the patients. In immune competent people most HPV infections are eliminated, but some establish a persistent infection [6]. Our case patient initially has squamous papilloma, followed by recurrence which histologically confirmed as condyloma acuminatum, with subsequent transformation to squamous cell carcinoma. All three lesions have one thing in common, that is HPV association. We think that persistent HPV infection in mucosa may have lead to this sequence. It has been reported that persistent HPV infection can lead to formation of invasive cancer with genotypes that are seen in carcinoma oral cavity and oropharynx i.e. HPV 16, 18 [7, 11] This phenomena has been described in cervical cancer also [6]. The other factor that plays an important role is immune suppression. Definitively there is increases risk of malignancy in immune supressed patients like those with organ transplantation [9]. The other factors like smoking, tobacco and alcohol intake are independent risk factors of development of cancer, in a study on a part of Indian population the risk of developing oral cavity carcinoma was increased two, five and two folds respectively.12 It was found that HPV infection increased risk to three times in oral squamous cell carcinoma independent to risk factors of addiction to alcohol or tobacco [13]. In ano-genital region, there is definitive risk in development of dysplasia and also invasive cancer; which may be due to co-infection with HPV 16 & 18 in benign lesions which usually harbour HPV subtypes 6 &11 [4]. Other possible explanation may be due to susceptibility in these patients to infection with high risk HPV genotypes. Infection itself causes immune suppression and hence a persistence of infection would increase the risk of co- infection with other HPV types and this increases the chance of formation of malignant lesion [4]. Buccal mucosa is susceptible to trauma, infections; these continuous abrasions make the mucosa susceptible to HPV to reach the basal cells and cause transformation of keratinocytes [14, 15]. HPV infection detection rate is 0- 74% in oral cancer [9]. Patients having HPV related benign lesions in oral cavity need a strict follow up and should be educated about HPV infection and the modes of transmission to prevent repeated HPV exposure. They should be counselled about the additive risk factors like smoking, alcohol, multiple sexual partners and to maintain oral hygiene. There are no reports or large series estimating risk of oral condyloma acuminatum as a risk factor in oral carcinoma. Oral and anogenital condyloma have similar kind of history in development of these lesions and in corollary anogenital condyloma have found to increase the risk of anogenital carcinomas and persistent HPV infection.
Conclusion
We hypothesise that oral condyloma acuminatum may be an independent risk factor for HPV positive oral carcinomas that need to be investigated further in large cohort to establish its role. These HPV positive benign lesions need to be followed up even after complete removal as persistent HPV infection may predict the development of oral and oropharyngeal carcinomas in future.
References
-
Scully C, Prime S, Maitland N (1985) Papillomaviruses: their possible role in oral disease. Oral Surg Oral Med Oral Pathol 60(2): 166-174.
-
Carneiro TE, Marhino SA, Verli FD, Mesquita ATM, Lima NL, et al. (2009) Oral squamous papilloma: clinical, histologic and immunohistochemical analyses. J oral sciences 51(3): 367-372.
-
Zunt SL, Tomich CE (1989) Oral condyloma acuminatum. J Dermatol Surg Oncol 15(6): 591-594.
-
Nordenvall C, Chang ET, Adami HO, Ye W (2006) Cancer risk among patients with condylomata acuminate. Int J Cancer 119(4): 888-93.
-
Koutsky L (1997) Epidemiology of genital human papillomavirus infection. Am J Med 102(5A): 3-8.
-
Ho GY, Burk RD, Klein S, Kadish AS, Chang CJ, et al. (1995) Persistent genital human papillomavirus infection as a risk factor for persistent cervical dysplasia. J Natl Cancer Inst 87(18): 1365-1371.
-
Campisi G, Giovannelli L (2009) Controversies surrounding human papilloma virus infection, head & neck vs oral cancer, implications for prophylaxis and treatment. Head Neck Oncol 1:8.
-
Garlick JA, Taichman LB (1991) Human papillomavirus infection of the oral mucosa. Am J Dermatopathol 13(4): 386-395.
-
Gillison ML, Koch WM, Capone RB, Spafford M, Westra WH, et al. (2000) Evidence for a Causal Association Between Human Papillomavirus and a Subset of Head and Neck Cancers. JNCI J Natl Cancer Inst 92(9): 709- 720.
-
Eversole LR, Laipis PJ, Merrell P, Choi E (1987) Demonstration of human papilloma virus DNA in oral condyloma acuminatum. J Oral Pathol 16(5): 266-272.
-
Borborema SCM, de Castro MM, Benevides dos SPJ, Talhiri S, Astolfi-Filho S (2006) Oral Focal Epithelial Hyperplasia: Report of Five Cases. Braz Dent J 17(1): 79-82.
-
Znaor A, Brennan P, Gajalakshmi V, Mathew A, Shanta V, et al. (2003) Independent and combined effects of tobacco smoking, chewing and alcohol drinking on the risk of oral, pharyngeal and esophageal cancers in Indian men. Int J Cancer 105(5): 681-686.
-
Watts SL, Brewer EE, Fry TL (1991) Human papillomavirus DNA types in squamous cell carcinomas of the head and neck. Oral Surg Oral Med Oral Pathol 71(6): 701-707.
-
Syrjanen SM, Syrjanen KJ, Happonen RP (1988) Human papillomavirus (HPV) DNA sequences in oral precancerous lesions and squamous cell carcinoma demonstrated by in situ hybridization. J Oral Pathol 17(6): 273-278.
-
Sikka S, Sikka P (2014) Association of Human Papilloma Virus 16 Infection and p53 Polymorphism among Tobacco using Oral Leukoplakia Patients: A Clinicopathologic and Genotypic Study. Int J Prev Med 5(4): 430-438.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?