An Unusual Cause of Upper Airway Obstruction in Newborn: Congenital Nasal Pyriform Aperture Stenosis
Congenital nasal pyriform aperture stenosis (CNAPS) is a rare cause of pediatric nasal airway obstruction that clinically mimics choanal atresia in a neonate. CNPAS is suspected clinically and confirmed with CT scanning. Early diagnosis and management is essential for this potentially life-threatening condition. Because of the association this anomaly has with other midline defects, such as holoprosencephaly, it is important to recognize it and pursue a thorough workup. Patients can be managed conservatively or surgically. Surgical treatment is usually reserved for those patients that fail conservative treatment. We present a case of CNPAS, to highlight the importance of recognizing the classic signs of CNPAS on cross-sectional imaging to prevent fatal outcome.
Introduction
Congenital nasal pyriform aperture stenosis (CNPAS) is a rare and potentially lethal nasal airway anomaly in newborn, first published in the radiology literature in 1988 and described clinically in 1989 [1], it typically presents with clinical features such as respiratory distress or episodic cyanosis due to narrowing of the pyriform aperture anteriorly and it can be confused with choanal atresia. CNPAS may present as an isolated condition or with associated craniofacial anomalies. The purpose of this report is to describe a case of CNPAS in association with solitary median maxillary central incisor, and to present the author’s experience in the non-surgical management of this rare anomaly.
A 10-day-old female baby, born at full-term, to nonconsanguinous parents, history of respiratory distress and cyanosis at birth, presented to our ear, nose and throat department for cyanosis and difficulty during feeding. Clinical examination revealed an oral breathing. There was no evidence of a cleft palate or others dysmorphic features. A pediatric nasal fiberoptic endoscope (2.7-mm diameter) was attempted but the scope could not pass through either nares.
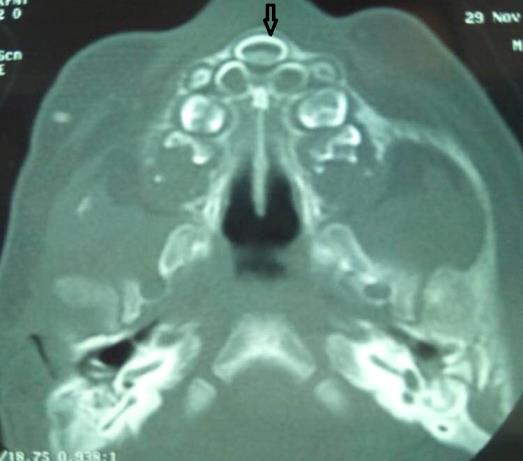
A CT scan was performed to evaluate the upper airways, showed a pyriform aperture stenosis of 4.5 mm, with solitary median maxillary central incisor and was negative for choanal atresia or others anomalies (Figures 1 & 2). MRI of the brain showed no intracranial abnormalities. Conservative treatment using nasal conformers and nasal decongestant drops, and feeding in the upright position. No active intervention was undertaken during this visit and the patient was asked to report for review earlier, in case there was any symptomatic worsening.

Discussion
The pyriform aperture is bounded laterally by the nasal processes of the maxilla and inferiorly by the junction of the horizontal processes of the maxilla and the anterior nasal spine and superiorly by the nasal bones [1, 2]. It's the narrowest part of the normal nasal airway, and small changes in its cross-sectional area can result in a significant increase in nasal airway resistance [3]. Congenital nasal pyriform aperture stenosis (CNPAS is characterized by the narrowing of the anterior bony nasal apertures, It is a rare condition due to bony overgrowth of the medial nasal process of the maxilla which is most often bilateral [4].
CNPAS may lead to asphyxia and respiratory failure, so early diagnosis and treatment is very important [5]. CNPAS can clinically mimic choanal atresia, with infants presenting with respiratory distress, either at birth or within the first few months of life. The neonate can present at birth with cyanosis, breathing difficulty (particularly when feeding) and nasal cavity narrowing to the extent that passage of a nasogastric tube is impossible [6]. Clinical symptoms of CNPAS may be delayed until several weeks, but bilateral choanal atresia is manifested in the first s of life [6].
This anomaly may be manifested as an isolated form or in association with other abnormalities including holoprosencephaly or solitary median maxillary central incisor (SMMCI) syndrome which presents in about 60% of infants with CNPAS [5]. The diagnosis of pyriform aperture stenosis can be made accurately with a CT scan, by obtaining thin (1.5 to 3.0 mm), contiguous axial sections in a plane parallel to the anterior hard palate. The normal range of width of the pyriform sinus in the age group of 0 – 6 months is 8.8 – 17.2 mm [median width = 13.5 mm] [7]. Each pyriform aperture width less than 3 mm, or a whole pyriform aperture width less than 8 mm, in a term infant, confirms the diagnosis of CNPAS. Once the diagnosis has been established, screening should rule out other congenital abnormalities involving the pituitary gland, cardiac and urogenital systems.
Treatment is either conservative or surgical depending on the severity of symptoms [8]. Conservative treatment, which involves the use of topical nasal decongestants, humidification, insertion of oral airway, and lavage feeding, is the initial line of management [5]. When there is moderate-to-severe stenosis, a surgical approach is preferred. A diameter of <5 mm at the inferior meatus and patient not responding to conservative treatment require surgical treatment, which involves pyriform aperture enlargement through an endo-oral sublabial approach to reshape the stenotic area with burs. This is a good and safe method that provides adequate field exposure, preventing damage to nasolabial soft tissues without visible scarring [6]. Surgical results are excellent and prognosis largely depends on co-existing neurological and/or endocrine problems [8].
Conclusion
This case has been presented to increase the awareness about this rare entity, potentially life- threatening condition in neonates. It should be considered in the differential diagnosis of any neonate or infant with signs and symptoms of upper airway compromise.
References
-
Sesenna E, Leporati M, Brevi B, Oretti G, Ferri A (2012) Congenital nasal pyriform aperture stenosis: diagnosis and management. Ital J Pediatr 38: 28.
-
Lowe LH, Booth TN, Joglar JM, Rollins NK (2000) Midface anomalies in children. Radiographics 20(4): 907-922.
-
Rozner L (1964) Nasal obstruction due to restriction of the bony nasal inlet. Br J Plast Surg 17: 287-296.
-
Robson CD, Hudgins PA (2003) Pediatric airway disease. In: Som PM, Curtin HD, (Eds.), Head and Neck Imaging. 4th (Edn.), Missouri: Mosby pp: 1540-1542.
-
Devambez M, Delattre A, Fayoux P (2009) Congenital nasal pyriform aperture stenosis: Diagnosis and management. Cleft Palate Craniofac J 46(3): 262-267.
-
Rao A, Godehal SM, Patil AR, Mallarajapatna G, Nandikoor S, et al. (2015) Congenital nasal pyriform aperture stenosis: a rare cause of neonatal nasal airway obstruction. BJR Case Rep 1(1): 20150006.
-
Ey EH, Han BK, Towbin RB, Jaun WK (1988) Bony inlet stenosis as a cause of nasal airway obstruction. Radiology 168(2): 477-479.
-
Visvanathan V, Wynne DM (2012) Congenital nasal pyriform aperture stenosis: A report of 10 cases and literature review. Int J Pediatr Otorhinolaryngol 76(1): 28-30.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?