Giant Retropharyngeal Lipoma: A Case Report
Lipomas are among the most common mesenchymal neoplasms in humans, which occur more frequently in mature adults aged between 40–60 years old. Lipomas can arise from any part of the body where normal fat is present. The neck lipomas are rare tumors. Most lipomas are small, weighing only a few grams and measuring less than 2 × 2 cm. They usually remain asymptomatic and appear simply as a located mass that causes cosmetic concerns for the patient. Lipomas are typically slow-growing tumors; only a few grow to an exceptionally large size. A giant lipoma was defined as a lesion that measures at least 10 cm in one dimension. Most lipomas do not present any difficulty in diagnosis. The treatment of choice of cervical lipomas is surgical removal. We here present a case of a giant anterior neck lipoma with a progressive increase in the swelling, retropharyngeal localization, with pain, dyspnea, dysphagia and dysphonia reported.
and Mahtar M
Aout Hospital, Casablanca, Morocco, Tel: 0619816666; Email: medamine.mennouni@gmail.com Keywords: Lipoma; Giant Lipoma; Retropharyngial Tumefaction; Dysphagia
Introduction
Lipomas are the most common benign mesenchymal tumor, present most commonly in the fifth or sixth decade of life and arising in any location where fat is normally present. Commonly located in the head and neck region with a 13% ratio of all lipomas [1], it usually involves in the posterior triangle. Retropharyngeal neck lipomas are a rare entity, and fewer still are giant anterior neck lipomas (> 10 cm) [2, 3, 4, 5, 6, 7, 8]. Lipomas can be superficial or deep; deeper lipomas are extremely rare and they are usually detected because of their size. Localization of tumors determines the type of symptoms, like dyspnea, cough, if located in the retropharyngeal area [3]. Clinical examination alone is often insufficient to identify the nature and exact origin of the mass, in which case, imaging is necessary, particularly when the tumor is deep seated [7].
We report the case of a 41-year-old man with no particular pathological history who suffers from a retropharyngeal mass gradually increasing in volume. The clinical examination revealed a painless hard mass, the swelling was of firm consistency. There has been no increase in local temperature and it was not attached to the overlying skin and surrounding structures. The patient progressively showed signs of pharyngolaryngeal compression: dyspnea, dysphagia, and dysphonia. The general and systemic examinations were without particularity. Cervical ultrasound showed a large echogenic mass. Computed tomography confirmed the retropharyngeal compression of the pharynx and larynx protruding from the sternocleidomastoid (Figures 1).
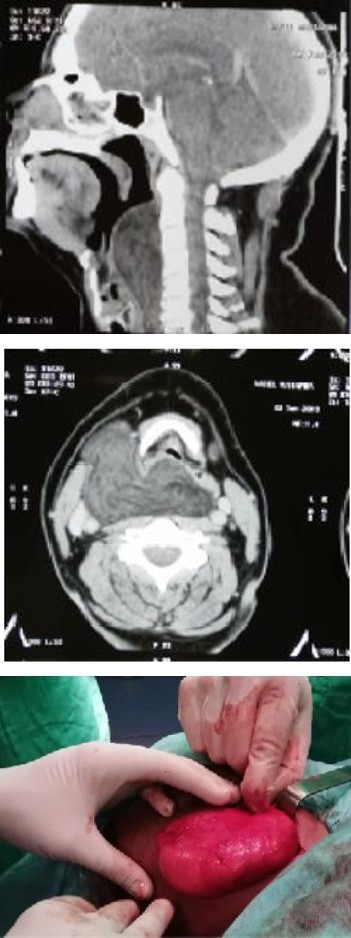
Figures 1: Retropharyngeal lipoma on CT scan.
Histopathological sections showed an encapsulated lesion comprising mature adipose tissue lobules, separated by fibrous septa, thus confirming the radio- cytological diagnosis of a giant benign lipoma. The postoperative period was uneventful. The check up after one year of follow-up was very good with no compressive symptoms or recurrence [9].
Discussion
Lipomas are one of the most common mesenchymal neoplasms in humans, which can arise from any part of In the literature, Solitary lipomas have rarely been objects of interest, and giant lipomas have been described as measuring up to 10 cm and weighing up to 1000 g [4, 6]. With a preferential location on the back and posterior cervical area [2, 3, 4, 5, 6, 7]. Below the clavicles, lipomas are more common in obese female patients over 40 years of age; however, the head and neck region, are mostly found in men in their seventh decade [2]. In a series of 25 cases of head and neck lipomas reported by Ahuja, et al. [10], 68% were men, correspondingly in the series of Som, et al. where 52 % of the cases reported were men [5]. The exact cause for lipoma is unclear though there is an association with genetic mutation in chromosome 12 in cases of solitary lipomas [2]. Malignant transformation of lipoma to liposarcoma is fairly rare [5].
Diagnosis of head and neck lipomas starts with a good clinical examination [7]. Lipomas are nonpainful, usually round, mobile masses with a characteristic soft, and doughy feel on palpation, with the skin over them often feeling cool because of the insulating quality of fat [6]. Although most superficial subcutaneous lipomas can be suspected with a high degree of accuracy by clinical examination alone, very large, deep-seated or infiltrating lipomas, as well as lipomas arising from unusual regions within the head and neck, require imaging for further assessment and diagnosis [3]. An ultrasound can give a clear and fast diagnosis of a lipoma. Typically, a lipoma appears in the ultrasound as a homogeneous hypoechogenic lesion that can be ovoid or lobulated [3]. However, lipomas may be sometimes isoechogenic or even hypoechogenic relative to adjacent muscle [6]. The CT attenuation number is related to the radiodensity of a lesion [6]. The attenuation number of water is set arbitrarily at zero [5]. Thus, lipomas have the typical CT characteristics of a homogeneous mass with few septations, a low CT attenuation number (usually measuring between -50 and -150 Hounsfield Units (HU)) and no contrast enhancement [6]. The MRI can also clearly define the limits of the lipoma from normal adipose tissue [3].
One weakness in the use of current diagnostic imaging techniques in the diagnosis of tumours of fatty tissue, is that neither CT nor MRI can differentiate a lipoma from a liposarcoma. This distinction can only be made with certainty by histopathological examination [3]. Giant lipomas are primarily an aesthetic problem [1]. They may also lead to functional limitations because of their size and weight. Very rarely, functional and vital prognosis are involved or signs of compression may be present [11, 12]. In this case, we did not find complications related to the anatomical location of the mass. The patient was dyspneic and had dysphagia and dysphonia. However, he also encountered functional limitations such as difficulty in physical exertion. The treatment of choice for lipomas is a blunt dissection with an ablation of the whole mass [13]. Transformation of a large lipoma (> 10 cm) into liposarcoma is rare. Histopathological examination of large lipomas should be done with caution to eliminate any risk of malignancy. In this case, the surgical treatment was successful in relieving all the complaints of the patient. Fortunately in this case, even if the size of the mass was greater than 5 cm, in retropharyngeal intubation was possible , thus and under general anesthesia, a laterocervical incision was made the mass was removed entirely. In addition, the histopathological diagnosis was compatible with the lipoma. The evolution was very good with a follow-up of one year.
Conclusion
In the head and neck region, lipomas can be present under different forms. They mostly occur subcutaneously in the posterior neck, and have a male predominance. Clinical examination alone is often insufficient to identify the nature and exact origin of the mass, so computed tomography or MRI scans are usually used to dernmine a specific pre-operative diagnosis. The treatment of choice for lipomas is a blunt dissection with an ablation of the whole mass associated to histological examination.
References
-
Phulari RG, Vidhi Soni, Trupti Pramod T, Gaurav Bakutra (2018) Oral fibrolipoma: A report of two cases and review of literature. Indian Journal of Dental Research 29(4): 513-516.
-
Brandler TI (1894) Large fibrolipoma. Br Med J 1:
-
Gowri Sankar M, Manu CB, Arun A (2017) Giant Lipoma Anterior Neck: A case report. Archives of Case Reports 1: 6- 8.
-
Francesco G, Ilaria Z, Valentina C, Francesco G, Giuseppe R, et al. (2012) A case of lipoma of lateral anterior neck treated with surgical enucleation. Dent Res J 9(2): 225-228.
-
Shamita C, Sandeep P, Sayan DN, Susenjit PM (2015) Anterior Neck Lipoma-A Giant Predicament. Hellenic Journal of Surgery 87(2): 203-205.
-
Som PM, Scherl MP, Rao VM, Biller HF (1986) Rare Presentations of Ordinary Lipomas of the Head and Neck: A Review. Am J Neuroradiol 7(4): 657-664.
-
Rahmani G, McCarthy P, Bergin D (2017) The diagnostic accuracy of ultrasonography for soft tissue lipomas: a systematic review. Acta Radiol Open 6(6): 205846011771670.
-
Terzioglu A, Tuncali D, Yuksel A, Bingul F, Aslan G (2004) Giant lipomas: a series of 12 consecutive cases and a giant liposarcoma of the thigh. Dermatol Surg 30(3): 463-467.
-
Sanchez MR, Golomb FM, Moy JA, Potozkin JR (1993) Giant lipoma: case report and review of the literature. J Am Acad Dermatol 28(2): 266-268.
-
Ahuja AT, King AD, Kew J, King W, Metreweli C (1998) Head and Neck Lipomas: Sonographic Appearance. Am J Neuroradiol 19(3): 505-508.
-
Signorini M, Campiglio GL (1998) Posttraumatic lipomas: where do they really come from? Plast Reconstr Surg 101(3): 699-705.
-
Yakubu AA, Edino ST, Mohammed AZ, Sheshe AA, Alhassan SU (2008) Giant and complicated subcutaneous lipoma of the neck. West Afr J Med 27(1): 44-46.
-
Eryilmaz M, Yigit T, Ozturk G, Safali M, Aksu AY (2007) Giant spindle cell lipoma of the posterior neck. Dermatol Surg 33(10): 1258-1261.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?