Retrospective Analysis of the Clinical Utility of a Protocol for Baseline Clinical Swallow Examination
Objective: The Bilancio Logopedico Breve (BLB)-swallowing subtest is a non-validated baseline Italian protocol widely used for clinical swallow examination (CSE). The aim of the study was to critically analyze the clinical utility of the items of BLB based on 5-years clinical experience in an intensive rehabilitation facility. Methods: In this retrospective study, 407 patients with different diagnoses were included. Clinical data, BLB assessment at admittance and discharge, signs of dysphagia during fiberoptic endoscopic evaluation of swallowing (FEES) and diet recommendations were extracted. A univariate analysis was performed to investigate the items associated with the decision of nutrition method and diet type, the presence of penetration or aspiration on FEES, and an improvement in diet type during the hospital stay. Results: Oral motor skills, dentition, voluntary cough, gag reflex, swallow trigger and signs of aspiration with liquid and/ or puree consistencies items showed significant associations with the decision of oral nutrition and/or to the type of oral diet, and with an evolution in the diet type. Gag reflex, swallow trigger and signs of aspiration with liquid and/or puree consistencies were significantly associated with penetration or aspiration at FEES. Pathological reflexes, lip sealing during swallowing, laryngeal excursion and oral residue items displayed poor associations with the clinical outcomes considered. Conclusion: The present findings support the use of BLB in the clinical practice as a guideline for CSE despite its limitations. Results should guide the revision of the protocol, preliminary to an advisable validation process of the tool.
Introduction
Dysphagia is defined as an alteration in the bolus transit from the mouth to the stomach [1]. Swallowing process may be impaired by neurological disorders and damages, oncological diseases, and the aging process [2]. Prevalence of dysphagia in the general population is about 3-5% [3], while it reaches 16% in elderly [4], 40-60% in patients with stroke [5], and 50-90% in patients with Parkinson’s disease [6]. Complications of dysphagia are aspiration pneumonia, malnutrition, dehydration, reduced QOL and limitations to social participation [7, 8, 9]. Therefore, the identification and the accurate assessment of patients at risk for dysphagia are of critical importance [10, 11].
The typical clinical pathway for swallowing evaluation consists, in order, of a screening, a clinical swallow examination, a mealtime observation and an instrumental assessment. Screening is usually performed by non-specialized professionals and is applied to the whole population of patients at risks of dysphagia [10]. The goal of a swallowing screening is to identify patients requiring an extended assessment of swallowing and promptly decide whether or not to orally feed the patient. Clinical Swallow Examination (CSE) is performed by professionals specialized on swallowing, typically speech and language therapists (SLTs), on patients who are suspected to have dysphagia. The CSE aims to recognize patients with dysphagia, to identify patients requiring an instrumental assessment, to decide the possibility and the type of oral nutrition, and to guide the possible swallowing treatment. Usually, the CSE is appropriately followed by a mealtime assessment to verify an adequate oral intake, the patient’s independence and the dietary prescription. Finally, instrumental assessment provides the final diagnosis of dysphagia, allows to identify pathophysiological mechanisms of swallowing disorders, and adds information to the CSE for decision on oral nutrition and swallowing treatment [12, 13, 14].
In our Intensive Rehabilitation Facility (IRF), considering the high prevalence of dysphagia in neurorehabilitation settings [15], all patients are directly assessed at admission by a SLT using the Bilancio Logopedico Breve (BLB)- swallowing subtest, an Italian baseline CSE protocol [16]. The advantages on the use of the BLB over other available CSE protocols are its shortness and rapidity, making it suitable for the use on a large number of patients. However, although its use has become widespread in different Italian hospitals and rehabilitation units, and its items provide a useful checklist for guiding a meticulous CSE, the BLB is a non-validated protocol. Beside this limitation, the clinical experience on the application of the CSE allowed to qualitatively identify other drawbacks of the protocol, e.g. the absence on an item on indirect signs of aspiration with solids or the different score range for the items.
The aim of the study is to retrospectively analyze the clinical utility of the BLB-swallowing subtest, in particular to identify which items are more relevant for identifying a swallowing disorder and for guiding an adequate diet prescription. This finding might lead to a future revision of the protocol, preliminary to the validation process. The clinical utility is investigated by studying: (i) the association between the scores of the BLB items and the clinician’s decision on the diet; (ii) the association between the scores of the BLB items and the signs of penetration and aspiration on instrumental assessment; (iii) the responsiveness of the BLB items to the diet evolution of the patients within the hospital stay.
Material and Methods
This retrospective study was carried out in Casa di Cura del Policlinico (Milan), a post-acute IRF. The study was conducted in accordance with the Declaration of Helsinki and was approved by the Local Ethics Committee (Milano Area B: Resolution 20_2017). At the time of admission, all patients signed an informed consent form on the use of demographic and clinical data for both clinical and research purposes. Clinical data of the patients and information on medical and rehabilitation procedures carried out during the hospitalization period were recorded on an electronic database management system, routinely used in the clinical practice.
Patients
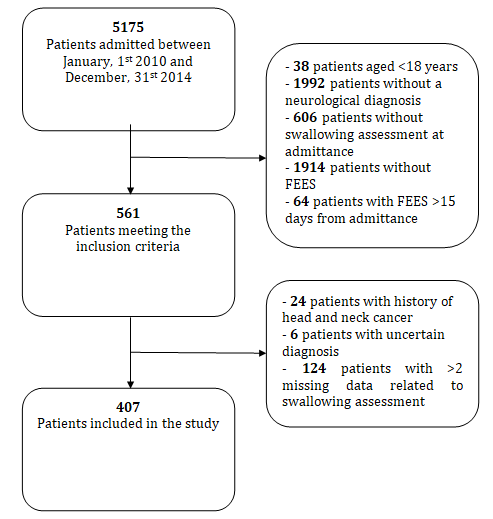
All patients, consecutively admitted to the post-acute IRF between January 1st, 2010 and December 31st, 2014, were screened for inclusion criteria. Inclusion criteria were: aged over 18 years, neurological diagnosis, BLB administered by a SLT before the first meal on the day of the admission, fiberoptic endoscopic evaluation of swallowing (FEES) conducted within 15 days from the admission. Patients were excluded if they had history of head and neck cancer, if diagnosis was uncertain, and if there were more than two missing data related to the swallowing clinical or instrumental assessment.
Bilancio Logopedico Breve-Swallowing Subtest
The BLB was developed by Gilardone, et al. [16] as a tool enabling a comprehensive and rapid baseline assessment of the areas of interest of SLTs in the neurological adult patients. The aims of the BLB – swallowing subtest (henceforth referred to as BLB) are to identify patients requiring a more extensive clinical and/or instrumental assessment and to guide the SLT in providing prompt diet recommendation. Because of its shortness it can be applied also to acute patients with fluctuations of vigilance or to bedridden patients. A validation process of the BLB has not been performed: yet no information regarding the psychometric properties of this test is available. It can be used by physicians and health professionals (SLTs in particular); no standardized training for administration is provided.
The BLB consists of 12 items, reported in Supplementary material. Each item is rated on a 2, 3 or 4-point scale; the lower the score the greater the impairment. BLB total score ranges from 0 (severe dysphagia) to 26 (within normal limits).
Procedures
All neurological patients underwent a CSE by a SLT at admission using the BLB, to establish the presence of dysphagia and to decide on a diet level. Moreover, the SLT assessed patient’s feeding independence. After the baseline CSE and a mealtime observation, the necessity of enteral tube feeding or the type of oral diet was documented and prescribed by the physician. Analogously, the method and the type of liquid and pharmacological treatments intake was recorded. The FEES was performed by a phoniatrician and swallowing trials included liquids (water), semisolids (pudding), and, if deemed safe, solids (biscuit). Due to the retrospective nature of the study, the number of trials and the volume of the bolus for each consistency are not available and might have varied across the sample. A CSE was again performed 2 days before discharge using the BLB and final diet recommendations were provided according to the final CSE and the supervisions during the hospitalization. No final CSE was available for patients that died or were transferred to an emergency unit.
Data Extraction
Data were extracted by two SLTs based on a defined data extraction sheet. The following data were extracted from the electronic clinical record database system for each patient meeting the inclusion criteria:
- Age
- Gender
- Diagnosis
- History of aspiration pneumonia
- Presence of tracheostomy and of enteral nutrition at admission
- Body mass index (BMI) at admission (introduced since January, 1st 2011)
- Item and total scores of the BLB swallowing subtest at admission and discharge
- Diet recommendations at admission and discharge
- Feeding independence at admission
- Penetration and/or aspiration detected on FEES The diagnosis was subsequently divided into 5 categories: 1) cerebrovascular diseases, including ischemic and/or hemorrhagic stroke, vasculopathy; 2) cerebrovascular diseases associated to minimally conscious state; 3) neurodegenerative diseases; 4) systemic diseases; 5) brain tumors. Diet recommendations were categorized as follows: nihil per os (NPO), pureed diet, solid diet.
Statistical Analysis
Data are reported as median (1st quartile – 3rd quartile) or as absolute (relative) frequency. The distribution of scores frequency for each BLB item at admission was analyzed to identify floor (frequency of the lowest score) and ceiling (frequency of the highest score) effects. Pearson chi- squared test was used to investigate the factors associated with (i) the decision of nutrition method and diet type and, (ii) the presence of penetration or aspiration on FEES. Mann-Whitney U test was performed to compare BLB item scores at admission and discharge in patients who evolved from a more restricted diet to a less restricted diet during hospital stay. Statistical analysis was performed with STATA version 12 (STATA Corp. Texas, USA). Significance was set at p<0.05.
Results
Patients
Overall, 5175 patients were admitted to the IRF over the 5-years period. After screening for inclusion criteria, 561 were initially selected, while 407 were finally included in the study. The flowchart for patients’ selection is reported in Figure 1. Patients were 218 males and 189 females with a mean age of 75.7±10.8. A diagnosis of cerebrovascular disease was recorded in 342 (84%) patients.
Score Distribution
Five items showed a clear skewness toward the ceiling, reaching a frequency >50% in the maximum score. In particular, the item pathological reflexes had the higher frequency, with 96% of the patients scoring 1 (maximum score). The items signs of aspiration with puree, lip sealing, laryngeal excursion, and oral residues followed with a frequency at the maximum score of 85%, 69%, 62.8%, and
58.1%, respectively.
• Factors associated with the decision of nutrition method and diet type A chi-squared analysis was performed to compare the distribution of BLB items’ scores and of clinical and demographic variables at admission between patients with decision of oral diet and those on NPO diet (Table 1).
| NPO diet N (%) | Oral diet N (%) | p | ||
|---|---|---|---|---|
| 104 (34.3%) | 303 (65.7%) | |||
| Age, yearsa | <78 | 48 (23.7) | 155 (76.3) | 0.379 |
| >= 78 | 56 (27.4) | 148(72.6) | ||
| Gender | Male | 52 (23.9) | 166 (76.1) | 0.282 |
| Female | 52 (27.5) | 137 (72.5) | ||
| Diagnosis | Cerebrovascular | 96 (28.1) | 246 (71.9) | 0.008 |
| Othersb | 8 (12.3) | 57 (87.7) | ||
| History of aspiration pneumonia | No | 88 (23.5) | 287 (76.5) | 0.001 |
| Yes | 16 (50) | 16 (50) | ||
| Tracheal cannula | No | 98 (24.8) | 297 (75.2) | 0.049 |
| Yes | 6 (50) | 6 (50) | ||
| Nasogastric tube | No | 15 (4.8) | 299 (95.2) | <0.001 |
| Yes | 89 (95.7) | 4 (4.3) | ||
| BMIa,c | <=22.8 | 53 (38.7) | 84 (61.3) | 0.003 |
| >22.8 | 31 (22.5) | 107 (77.5) | ||
| Feeding independence | No | 99 (32.3) | 208 (67.7) | < 0.001 |
| Yes | 0 (0) | 54 (100) | ||
| BLB Oral motor skills | 0 | 12 (70.6) | 5 (29.4) | < 0.001 |
| 1 | 32 (35.6) | 58 (64.4) | ||
| 2 | 40 (19) | 171 (81) | ||
| 3 | 17 (20.5) | 66 (79.5) | ||
| BLB Voluntary cough | 0 | 30 (42.9) | 40 (57.1) | 0.001 |
| 1 | 40 (21.5) | 146 (78.5) | ||
| 2 | 27 (20.2) | 107 (79.9) | ||
| BLB Pathological reflexes | 0 | 9 (56.3) | 7 (43.8) | 0.004 |
| 1 | 94 (24.2) | 295 (75.8) | ||
| BLB Gag reflex | 0 | 38 (34.5) | 72 (65.5) | 0.003 |
| 1 | 35 (27.6) | 92 (72.4) | ||
| 2 | 27 (16.7) | 135 (83.3) | ||
| BLB Dentition | 0 | 45 (48.4) | 48 (51.6) | < 0.001 |
| 1 | 36 (19.5) | 149 (80.5) | ||
| 2 | 23 (17.8) | 106 (82.2) | ||
| BLB Lip sealing during swallowing | 0 | 3 (37.5) | 5 (62.5) | 0.655 |
| 1 | 31 (26.5) | 86 (73.5) | ||
| 2 | 68 (24.4) | 211 (75.6) | ||
| BLB Oral preparatory phase | 0 | 4 (36.4) | 7 (63.6) | 0.214 |
| 1 | 26 (30.6) | 59 (69.4) | ||
| 2 | 37 (20.1) | 147 (79.9) | ||
| 3 | 21 (24.7) | 64 (75.3) | ||
| BLB Swallow trigger | 0 | 3 (75) | 1 (25) | <0.001 |
| 1 | 38 (55.1) | 31 (44.9) | ||
| 2 | 45 (26) | 128 (74) | ||
| 3 | 18 (11.2) | 143 (88.8) | ||
| BLB Laryngeal excursion | 0 | 4 (66.7) | 2 (33.3) | 0.062 |
| 1 | 37 (25.5) | 108 (74.5) | ||
| 2 | 62 (24.3) | 193 (75.7) | ||
| BLB Oral residues | 0 | 8 (38.1) | 13 (61.9) | 0.017 |
| 1 | 24 (16.5) | 121 (83.5) | ||
| 2 | 63 (27.4) | 167 (72.6) | ||
| BLB Signs of aspiration with liquid trials | 0 | 21 (30.4) | 48 (69.6) | 0.225 |
| 1 | 30 (20.1) | 119 (79.9) | ||
| 2 | 38 (21.8) | 136 (78.2) | ||
| BLB Signs of aspiration during puree trials | 0 | 7 (87.5) | 1 (12.5) | <0.001 |
| 1 | 27 (51.9) | 25 (48.1) | ||
| 2 | 64 (18.8) | 276 (81.2) |
Table 1: ** Chi-squared analysis on factors associated with the decision of oral diet A NPO diet was prescribed for 104 (34.3%) p
Note: Significant p vales are reported in bold aPatients were divided into 2 groups based on the median of the distribution of the variable in the clinical sample bOther diagnosis included: neurodegenerative diseases (n=44), systemic diseases (n=15), brain cancer (n=6) cMeasure only available since January, 1st 2011 Table 1: Chi-squared analysis on factors associated with the decision of oral diet A NPO diet was prescribed for 104 (34.3%) patients. Diagnosis of cerebrovascular disease, history of aspiration pneumonia, presence of tracheal cannula and nasogastric tube, lower BMI, and feeding dependence were significantly associated with the NPO diet. Concerning BLB, 8 items showed an association between a lower score and the frequency of NPO recommendation: oral motor skills, voluntary cough, pathological reflexes, gag reflex, dentition, swallow trigger, oral residues, and signs of aspiration with puree.
| Pureed oral diet N (%) | Solid oral diet N (%) | p | ||
|---|---|---|---|---|
| 153 (50.5%) | 150 (49.5%) | |||
| Age, yearsa | <78 | 72 (46.5) | 83 (53.5) | 0.15 |
| >= 78 | 81 (54.7) | 67 (45.3) | ||
| Gender | Male | 81 (48.8) | 85 (51.2) | 0.515 |
| Female | 72 (52.6) | 65 (47.4) | ||
| Diagnosis | Cerebrovascular | 138 (56.1) | 108 (43.9) | <0.001 |
| Othersb | 15 (26.3) | 42 (73.7) | ||
| History of aspiration pneumonia | No | 143 (49.8) | 144 (50.2) | 0.324 |
| Yes | 10 (62.5) | 6 (37.5) | ||
| Tracheal cannula | No | 147 (49.5) | 150 (50.5) | 0.014 |
| Yes | 6 (100) | 0 (0) | ||
| Nasogastric tube | No | 150 (50.2) | 149 (49.8) | 0.324 |
| Yes | 3 (75) | 1 (25) | ||
| BMIa,c | <=22.8 | 50 (59.5) | 34 (40.5) | 0.116 |
| >22.8 | 53 (49.5) | 54 (50.5) | ||
| Feeding independence | No | 128 (61.5) | 80 (38.5) | < 0.001 |
| Yes | 10 (18.5) | 44 (81.5) | ||
| BLB Oral motor skills | 0 | 5 (100) | 0 (0) | < 0.001 |
| 1 | 44 (75.9) | 14 (24.1) | ||
| 2 | 87 (49.1) | 84 (50.9) | ||
| 3 | 14 (21.2) | 52 (78.8) | ||
| BLB Voluntary cough | 0 | 31 (77.5) | 9 (22.5) | <0.001 |
| 1 | 80 (54.8) | 66 (45.2) | ||
| 2 | 36 (33.6) | 71 (66.4) | ||
| BLB Pathological reflexes | 0 | 5 (71.4) | 2 (28.6) | 0.259 |
| 1 | 147 (49.8) | 148 (50.2) | ||
| BLB Gag reflex | 0 | 39 (54.2) | 33 (45.8) | 0.093 |
| 1 | 53 (57.6) | 39 (42.4) | ||
| 2 | 59 (43.7) | 76 (56.3) | ||
| BLB Dentition | 0 | 44 (91.7) | 4 (8.3) | < 0.001 |
| 1 | 72 (48.3) | 77 (51.7) | ||
| 2 | 37 (34.9) | 69 (60.1) | ||
| BLB Lip sealing during swallowing | 0 | 5 (100) | 0 (0) | 0.001 |
| 1 | 54 (62.8) | 32 (37.2) | ||
| 2 | 93 (44.1) | 118 (55.9) | ||
| BLB Oral preparatory phase | 0 | 7 (100) | 0 (0) | <0.001 |
| 1 | 45 (76.3) | 14 (23.7) | ||
| 2 | 59 (40.1) | 88 (59.9) | ||
| 3 | 17 (26.6) | 47 (73.4) | ||
| BLB Swallow trigger | 0 | 1 (100) | 0 (0) | <0.001 |
| 1 | 26 (83.9) | 5 (16.1) | ||
| 2 | 81 (63.3) | 47 (36.7) | ||
| 3 | 45 (31.5) | 98 (68.5) | ||
| BLB Laryngeal excursion | 0 | 2 (100) | 0 (0) | 0.039 |
| 1 | 63 (58.3) | 45 (41.7) | ||
| 2 | 88 (45.6) | 105 (54.4) | ||
| BLB Oral residues | 0 | 9 (69.2) | 4 (30.8) | 0.105 |
| 1 | 53 (43.8) | 68 (56.2) | ||
| 2 | 89 (53.3) | 78 (46.7) | ||
| BLB Signs of aspiration with liquid trials | 0 | 40 (83.3) | 8 (16.7) | <0.001 |
| 1 | 61 (51.3) | 58 (48.7) | ||
| 2 | 52 (38.2) | 84 (61.8) | ||
| BLB Signs of aspiration during puree trials | 0 | 1 (100) | 0 (0) | 0.215 |
| 1 | 16 (64) | 9 (36) | ||
| 2 | 135 (48.9) | 141 (51.1) |
Table 2: ** Chi-squared analysis on factors associated with diet type.
Note: Significant p vales are reported in bold aPatients were divided into 2 groups based on the median of the distribution of the variable in the clinical sample bOther diagnosis included: neurodegenerative diseases (n=44), systemic diseases (n=15), brain cancer (n=6) bVariable only available since January 1st, 2011 Table 2: Chi-squared analysis on factors associated with diet type.
Analogously, the association between BLB and clinical and demographic information at admission and diet type recommendation was analyzed. Among the 303 patients on oral nutrition, the variables’ distribution was compared between patients who were recommended a pureed diet and patients on solid diet. Table 2 depicts the results of the chi-squared analysis. Diagnosis of cerebrovascular disease, presence of tracheal cannula and nasogastric tube, and feeding dependence were significantly associated with the recommendation of a pureed diet. Eight BLB items showed an association between a lower score and the frequency of pureed diet recommendation: oral motor skills, voluntary cough, dentition, lip sealing, oral preparatory phase, swallow trigger, laryngeal excursion, and signs of aspiration with liquid.
| No penetration/ aspiration N (%) | Penetration/ aspiration N (%) | p | ||
|---|---|---|---|---|
| 327 (80.9%) | 77 (19.1%) | |||
| Age, yearsa | <78 | 160 (79.6) | 41 (20.4) | 0.495 |
| >= 78 | 167 (82.3) | 36 (17.7) | ||
| Gender | Male | 178 (82.8) | 37 (17.2) | 0.374 |
| Female | 149 (78.8) | 40 (21.2) | ||
| Diagnosis | Cerebrovascular Othersb | 274 (80.6) | 66 (19.4) | 0.678 |
| 53 (82.8) | 11 (17.2) | |||
| History of aspiration pneumonia | No | 298 (80.1) | 74 (19.9) | 0.146 |
| Yes | 29 (90.6) | 3 (9.4) | ||
| Tracheal cannula | No | 319 (81.6) | 72 (18.4) | 0.07 |
| Yes | 8 (61.5) | 5 (38.5) | ||
| Nasogastric tube | No | 262 (84) | 50 (16) | 0.004 |
| Yes | 65 (70.7) | 27 (29.3) | ||
| Distance admission-FEES, days a | <=5 | 170 (82.1) | 37 (17.9) | 0.604 |
| >5 | 157 (80.1) | 39 (19.9) | ||
| Feeding independence | No | 243 (79.7) | 62 (20.3) | 0.246 |
| Yes | 45 (86.6) | 7 (13.5) | ||
| BLB Oral motor skills | 0 | 14 (82.4) | 3 (17.6) | 0.676 |
| 1 | 76 (83.5) | 15 (16.5) | ||
| 2 | 166 (78.7) | 45 (21.3) | ||
| 3 | 67 (83.7) | 13 (16.3) | ||
| BLB Voluntary cough | 0 | 55 (77.5) | 16 (22.5) | 0.26 |
| 1 | 147 (79.5) | 38 (20.5) | ||
| 2 | 113 (85.6) | 19 (14.4) | ||
| BLB Pathological reflexes | 0 | 12 (80) | 3 (20) | 0.932 |
| 1 | 313 (80.9) | 74 (19.1) | ||
| BLB Gag reflex | 0 | 76 (71) | 31 (29) | 0.006 |
| 1 | 104 (82.5) | 22 (17.5) | ||
| 2 | 141 (86.5) | 22 (13.5) | ||
| BLB Dentition | 0 | 70 (76.1) | 22 (23.9) | 0.268 |
| 1 | 153 (84.1) | 29 (15.9) | ||
| 2 | 104 (80) | 26 (20) | ||
| BLB Lip sealing during swallowing | 0 | 6 (75) | 2 (25) | 0.899 |
| 1 | 94 (80.3) | 23 (19.7) | ||
| 2 | 224 (81.2) | 52 (18.8) | ||
| BLB Oral preparatory phase | 0 | 9 (81.8) | 2 (18.2) | 0.816 |
| 1 | 67 (78.8) | 18 (21.2) | ||
| 2 | 150 (82.9) | 31 (17.1) | ||
| 3 | 67 (78.8) | 18 (21.2) | ||
| BLB Swallow trigger | 0 | 1 (25) | 3 (75) | <0.001 |
| 1 | 48 (70.6) | 20 (29.4) | ||
| 2 | 139 (79.9) | 35 (20.1) | ||
| 3 | 139 (88) | 19 (12) | ||
| BLB Laryngeal excursion | 0 | 4 (66.7) | 2 (33.3) | 0.606 |
| 1 | 114 (80.3) | 28 (19.7) | ||
| 2 | 209 (82) | 46 (18) | ||
| BLB Oral residues | 0 | 14 (70) | 6 (30) | 0.352 |
| 1 | 120 (83.3) | 24 (16.7) | ||
| 2 | 187 (81.7) | 42 (18.3) | ||
| BLB Signs of aspiration with liquid trials | 0 | 49 (71) | 20 (29) | 0.011 |
| 1 | 118 (80.3) | 29 (19.7) | ||
| 2 | 151 (87.3) | 22 (12.7) | ||
| BLB Signs of aspiration during puree trials | 0 | 4 (50) | 4 (50) | 0.015 |
| 1 | 37 (72.5) | 14 (27.5) | ||
| 2 | 281 (83.1) | 57 (16.9) |
Table 3: ** Chi-squared on factors associated with penetration or aspiration in FEES.
Note: Significant p vales are reported in bold. aPatients were divided into 2 groups based on the median of the distribution of the variable in the clinical sample. bOther diagnosis included: neurodegenerative diseases (n=44), systemic diseases (n=15), brain cancer (n=6). Table 3: Chi-squared on factors associated with penetration or aspiration in FEES.
• Factors associated with penetration or aspiration at FEES The association between the BLB and signs of penetration or aspiration instrumentally assessed during FEES was assessed. Results are reported in Table 3. The presence of a nasogastric tube at admission was the only clinical factor associated with lower airways’ invasion (p=0.004). Penetration or aspiration on FEES was significantly associated with lower scores at the items gag reflex, swallow trigger, signs of aspiration with liquid, and signs of aspiration with puree.
| pre | post | pa | |
|---|---|---|---|
| Oral motor skills | 2 (2-2) | 2 (2-3) | <0.001 |
| Voluntary cough | 1 (1-2) | 2 (1-2) | <0.001 |
| Pathological reflexes | 1 (1-1) | 1 (1-1) | 0.375 |
| Gag reflex | 1 (0-2) | 1 (1-2) | 0.032 |
| Dentition | 1 (0-2) | 1 (1-2) | 0.001 |
| Lip sealing during swallowing | 2 (1-2) | 2 (2-2) | 0.066 |
| Oral preparatory phase | 2 (1-2) | 2 (2-3) | <0.001 |
| Swallow trigger | 2 (2-3) | 3 (2-3) | <0.001 |
| Laryngeal excursion | 2 (1-2) | 2 (2-2) | <0.001 |
| Oral residues | 2 (1-2) | 2 (1-2) | 0.007 |
| Signs of aspiration with liquid trials | 1 (1-2) | 2 (2-2) | <0.001 |
| Signs of aspiration during puree trials | 2 (2-2) | 2 (2-2) | <0.001 |
Table 4: Responsiveness of BLB items to diet evolution (N=161).
aMann-Whitney-U test. Results are reported as median (1st quartile-3rd quartile). Significant p-values are in bold. Table 4: Responsiveness of BLB items to diet evolution (N=161).
• Responsiveness to diet evolution Six patients died during hospitalization and 42 were transferred to an emergency unit. Thus, BLB at discharge was available for 359 patients. Among these patients, 159 (44.3%) patients evolved from a more restricted diet to a less restricted diet. In particular, 37 patients evolved from NPO to a pureed diet, 35 patients from NPO to a solid diet, while
87 patients from pureed to solid diet. BLB items scores were compared between the CSE at admission and at discharge in this sample of patients. All items, except two (pathological reflexes and lip sealing), showed a statistically significant improvement (Table 4). A summary of the findings for each BLB item is reported in Table 4.
| Scores distributiona | Association with the decision of oral nutrition | Association with diet type | Association with penetration- aspiration | Sensitivity to diet evolution | |
|---|---|---|---|---|---|
| Oral motor skills | + | + | + | - | + |
| Voluntary cough | + | + | + | - | + |
| Pathological reflexes | - | + | - | - | - |
| Gag reflex | + | + | - | + | + |
| Dentition | + | + | + | - | + |
| Lip sealing during swallowing | - | - | + | - | - |
| Oral preparatory phase | + | - | + | - | + |
| Swallow trigger | + | + | + | + | + |
| Laryngeal excursion | - | - | + | - | + |
| Oral residues | - | + | - | - | + |
| Signs of aspiration with liquid trials | + | - | + | + | + |
| Signs of aspiration during puree trials | - | + | - | + | + |
Table 5: ** Summary of items properties.
aCeiling effect (highest score frequency >50%). Table 5: Summary of items properties.
Discussion
The study provides a first critical analysis of the BLB swallowing subtest, an Italian baseline CSE protocol, based on its use in the clinical practice over a 5-years period in a large sample of patients with neurological diseases. It is essential to specify that the study did not aim to validate the BLB swallowing subtest, as the clinical experience accrued since 2010 allowed to qualitatively identify both advantages and limitation in the use of this CSE protocol. Conversely, the results enabled to pinpoint a different clinical utility of the BLB items and may be useful for a revision of the protocol in the future.
Among the 12 items, 4 items showed poor findings according to the analyses (Table 5): pathological reflexes, lip sealing during swallowing, laryngeal excursion, oral residue. The item pathological reflexes showed the greatest ceiling effect (>90%). This result may be a consequence of two aspects. Firstly, the item was dichotomous (0-1) as pathological oral reflexes were only judged as present or absent. Secondly, this symptom reflects a diffuse hemispheric dysfunction and, therefore, a severe neurological impairment, which is restricted to a limited number of patients in the IRF. Concerning laryngeal excursion, the poor association values may be related to the difficulties in assessing this aspect during CSE. Indeed, laryngeal elevation is a critical mechanism for swallowing safety (i.e. avoiding penetration and aspiration) [17]. However, a poor inter-rater agreement (ICC 0.446) was previously reported for its assessment during CSE [18]. Oral residue and lip sealing are relevant aspects to assess as they may reflect difficulties in oral preparation and oral transit, especially with solids. However, they were found to be significant only in respectively two and one analyses performed in the present study. The items showed a clear ceiling effect (>50%), thus reducing the variability in the scores. It may be argued that, although recognizing their important in oral processing of food, the possibility to assess them during CSE, with a small number of swallowing trial, in a standard situation, and with small volumes, may be limited. Conversely, their assessment during a meal observation may provide more valuable information to guide the refinement of diet recommendations.
The items swallow trigger, oral motor skills, voluntary cough, gag reflex, dentition, and signs of aspiration during liquid showed the best findings in the analysis of the present study (Table 5) and, therefore, seem to be useful for guiding the clinician in the decision of nutrition method and diet type, for identifying the patients with signs of penetration and aspiration on FEES, and for detecting changes of swallowing function over time. The item signs of aspiration during puree was significantly associated with the decision of oral nutrition, the presence of penetration or aspiration on FEES and was sensitive to diet evolution. As expected, no statistically significant association was found with the decision of the diet type (pureed vs. solid diet).
The association between the BLB and the diet recommendation was investigated in two different analyses: (i) comparing patients with NPO vs. oral diet recommendation and (ii) comparing patients with pureed vs. solid oral diet. The difference in the results of the two analyses arises interesting consideration on the items to include in a bedside swallowing protocol based on the targeted aim of the protocol. For instance, assessing oral preparation is relevant for the decision of the type of oral diet, but may be omitted if the tool only aims at supporting the decision of an oral or non-oral nutrition.
Prevention of pulmonary complication (i.e., aspiration pneumonia) is one of the primary goals of swallowing assessment [10]. Instrumental assessment, either with FEES or videofluoroscopy, represents the gold standard for swallowing evaluation [19]. Previous studies documented that CSE is still not strongly predictive of aspiration on instrumental assessment [20]. We assessed the association between BLB items and FEES findings of penetration or aspiration and found a significant association with the items gag reflex, swallow trigger, signs of aspiration with liquid, and with puree trials. Although all the items missed to identify a certain percentage of patients with penetration or aspiration, the value of the CSE in the identification of patients at risk of penetration and aspiration and its advantages over FEES or video fluoroscopy, being low-tech and promptly available in all settings, must be acknowledged. The association between the alteration of the gag reflex and deglutition difficulties is known and it has been previously documented [21]. The item swallow trigger is itself more problematic since a delayed initiation of the pharyngeal phase can be identified only though an instrumental assessment of swallowing [22, 23]. However, the clinical detection of any disturbance or latency in the timing of the swallowing act could reasonably and efficiently highlight a deficit in the transition between the voluntary and the reflex phases of deglutition. Such explanation could support the present finding.
The study has some limitations, mainly related to the retrospective design. Firstly, the data extraction showed some missing values. Patients with more than 2 missing values in the swallowing assessments were not included and the rate of missing value in the BLB items were <5%. The only exception is the item on oral preparatory phase that reached 10% of missing values. This item may be not assessable in some patients, but the retrospective design did not allow to discriminate between missing values and not assessable items. Secondly, the FEES protocol was not standardized, thus variability in the number of trials and volumes may have occurred among patients. Moreover, due to the retrospective nature of the study it was not possible to retrieve more reliable data from FEES reports other than the presence of penetration or aspiration. CSE and FEES interpretation may be prone to clinicians’ subjectivity, which could not be controlled through reliability analysis. Multivariate analysis was not performed due to the low frequency of some cells. However, independent association among BLB items and other factors may not be of primary importance when aiming to identify markers of swallowing impairment and not predictive factors. Lastly, BLB present several limitations: different scoring for each item, high risk of subjectivity in the administration and the interpretation, no standardized training before its administration, no validation study, and no trial with the solid consistency.
In conclusion, the BLB swallowing subtest was critically analyzed based on 5-years clinical experience in an inpatient rehabilitation department. Eight out of 12 items showed a satisfactory performance being associated to diet recommendations and signs of dysphagia on FEES and recording an evolution of swallowing function over time. The present findings support the use of BLB in the clinical practice as a guideline for CSE and highlight the need of a revision of the protocol and a subsequent validation procedure.
Statement of Ethics
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Local Ethics Committee (Milano Area B: Resolution 20_2017). At the time of admission, all patients signed an informed consent form.
Data Availability Statement
All data generated or analyzed during this study are included in this article or its supplementary material files. Further enquiries can be directed to the corresponding author.
Conflict of Interest Statement
- Financial Disclosure: no funding, or financial relationship to disclose. Non-financial disclosure and conflict of interest: Marco Gilardone is one of the authors of the Bilancio Logopedico Breve; the other authors have nothing to disclose.
- Authors’ Contributions N.P., M.G., and M.C. designed the study. M.L., M.V. and G.G. performed patients’ enrolment and data collection. F.M. and N.V. provided the data analysis. N.P., I.D., M.C. and M.G. interpreted the results. N.P. and M.V. took the lead in writing the manuscript. All authors provided critical feedback and helped shape the paper. All authors read and approved the final version of the paper.
References
-
Merlo A, Cohen S (1988) Swallowing disorders. Annu Rev Med 39: 17-28.
-
Cook IJ, Kahrilas PJ (1999) AGA technical review on management of oropharyngeal dysphagia. Gastroenterology 116: 455-478.
-
Lindgren S, Janzon L (1991) Prevalence of swallowing complaints and clinical findings among 50-79-year-old men and women in an urban population. Dysphagia 6: 187-192.
-
Bloem BR, Lagaay AM, Van Beek W (1990) Prevalence of subjective dysphagia in community residents aged over 87. BMJ 300: 721-722.
-
Perry L, Love CP (2001) Screening for dysphagia and aspiration in acute stroke: a systematic review. Dysphagia 16: 7-18.
-
Kuhlemeier KV (1994) Epidemiology and dysphagia. Dysphagia 9: 209-217.
-
Curtis JL, Langmore SE (1997) Respiratory functions and complications related to deglutition. In: Perlman AL, Schulze-Delrieu K (Eds.), Deglutition and its disorders. San Diego, Singular Publishing, pp: 125-52.
-
McHorney CA, Robbins J, Lomax K (2002) The SWAL- QOL and SWAL-CARE outcomes tool for oropharyngeal dysphagia in adults: III. Documentation of reliability and validity. Dysphagia 17: 97-114.
-
Woisard V, Sordes F (2014) Health related quality of life and oropharyngeal dysphagia. Ann Phys Rehabil Med 57(1): e264.
-
Eltrigham SA, Kilner K, Gee M (2018) Impact of dysphagia assessment and management in risk of stroke-associated pneumonia: a systematic review. Cerebrovasc Dis 46: 99- 107.
-
Paris G, Martinaud O, Hannequin D (2012) Clinical screening of oropharyngeal dysphagia in patients with ALS. Ann Phys Rehabil Med 55(9-10): 601-608.
-
Bours GJ, Speyer R, Lemmens J (2009) Bedside screening tests vs. videofluoroscopy or fibreoptic endoscopic evaluation of swallowing to detect dysphagia in patients with neurological disorders: systematic review. J Adv Nurs 65(3): 477-493.
-
Kertscher B, Speyer R, Palmieri M (2014) Bedside screening to detect oropharyngeal dysphagia in patients with neurological disorders: an updated systematic review. Dysphagia 29: 204-212.
-
Mann G (2002) The Mann Assessment of Swallowing Ability. Clifton Park: Singular, Thompson, Delmar Learning, pp: 56.
-
Nakadate A, Otaka Y, Kondo K (2016) Age, body mass index, and white blood cell count predict the resumption of oral intake in subacute stroke patients. J Stroke Cerebrovasc Dis 25: 2801-2818.
-
Gilardone M, Fussi F (2007) BLB, Bilancio logopedico breve. Torino: Edizioni Libreria Cortina.
-
Han H, Shin G, Jun A (2016) The Relation Between the Presence of Aspiration Penetration and the Clinical Indicators of Dysphagia in Poststroke Survivors. Ann Rehabil Med 40: 88-94.
-
Chun SW, Lee SA, Jung IY (2011) Inter-rater Agreement for the Clinical Dysphagia Scale. Ann Rehabil Med 35: 470-476.
-
Giraldo-Cadavid LF, Leal-Leano LR, Leon-Basantes GA (2017) Accuracy of endoscopic and videofluoroscopic evaluations of swallowing for oropharyngeal dysphagia. Laryngoscope 127(9): 2002-2010.
-
McCullough GH, Wertz RT, Rosenbek JC (2001) Sensitivity and specificity of clinical/bedside examination signs for detecting aspiration in adults subsequent to stroke. J Commun Disord 34(1-2): 55-72.
-
Xu Z, Gu Y, Li J, Wang C, Wang R, Huang Y, et al. (2019) Dysphagia and aspiration pneumonia in elderly hospitalization stroke patients: Risk factors, cerebral infarction area comparison. J Back Musculoskelet Rehabil 32(1): 85-91.
-
Daniels SK, Huckabee ML, Gozdzikowska K (2019) Dysphagia following stroke. Plural Publishing pp: 132- 133.
-
Takeda C, Yoshida M, Nakamori M (2020) Delayed Swallowing Reflex is Overlooked in Swallowing Screening Among Acute Stroke Patients. J Stroke Cerebrovasc Dis 29(12): 105303.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?