Paranasal Sinus Cysts Encountered Over Twenty Years: Varieties, Management, Recommendations, and Outcome
Background: We recorded all cases presenting with paranasal sinus cysts to draw attention to those with unusual presentations and their management outcome in a retrospective original study. Methods: All patients were subjected to history-taking, ENT examination, endoscopic examination, CT scanning, and managed with endoscopic sinus surgery/or a combined approach. Results: We encountered 54 patients with paranasal sinus cysts. Mucocele/pyocele was the commonest (79.6%), followed by radicular cyst (9.3%), dentigerous cyst (5.55%), and fungocele (5.55%). The frontal sinus was the commonest sinus of cyst origin (55.6%). Maxillary sinus cysts occurred in 16.6% of cases. The sphenoid sinus was the "least" sinus of cyst origin in 7.4% of cases. Conclusion: Ethmoid mucocele occurred mostly by extension from other sinuses, predominantly frontal. With exclusive frontal sinus cysts, it is essential to look for possible underlying pathology or associated complication. Fungocele, a new nomenclature, could complicate those with allergic fungal sinusitis.
Ramadan Hashem Sayed, Khaled Gamal Dahy* and Al Hussein Awad Ali
Background
A wide variety of paranasal sinus (PNS) cysts had been reported in the literature including extrinsic, which originate in nearby structures like the dental tissues (radicular cyst, dentigerous cyst, and keratocystic odontogenic tumors), or intrinsic, which originate in the mucosa of the paranasal sinuses especially mucoceles and pyocele. Radicular cysts (apical periodontal cysts, dental root end cysts) are the most common inflammatory odontogenic cysts in tooth- bearing areas of the jaws they originate from an epithelial rest of Malassez in periodontal ligaments secondary to inflammation. They are most frequently found at the apices of the involved teeth with infected or necrotic pulps; however, they may also be found on the lateral aspects of the roots in relation to accessory root canals [1, 2]. Most commonly, radicular cysts occur between the third and the sixth decades of life with male predominance and could occur in relation to the maxillary sinus. Dentigerous cyst (DC) or follicular cyst is the second most common type of odontogenic cyst [3]. It forms during tooth development and is associated with the pressure exerted by the crown of an unerupted (or partially erupted) tooth on the fluid within the follicular space. They almost exclusively occur in permanent dentition [4]. The most common location of DC is the mandibular third molar, more rarely occurring in the maxillary sinus. Enucleation is the standard treatment [4]. Keratocystic odontogenic tumors are rare and benign lesions of odontogenic origin with a potential for aggressive and infiltrative behavior [5]. They are more common in the third to sixth decades with a male to female ratio is approximately 2:1 and the majority are found in the mandible and could occur in the maxillary sinus [6]. Mucoceles of the PNSs are benign, chronic expanding lesions that develop because of obstruction of the sinus ostium. It is the commonest cyst affecting the PNSs, and if infected, it forms pyocele. The frontal sinus is the most common sinus to be affected by a mucocele, which usually results from trauma or inflammatory processes [7], followed by ethmoid, maxillary, and to a lesser extent the sphenoid sinus. Onodi cell mucocele is extremely rare and might cause visual loss owing to its close relation to the optic nerve [8] and a higher rate of optic nerve protrusion and dehiscence [9]. Posttraumatic mucocele was the least frequent form of PNS mucoceles and was located predominantly in the frontal sinus, causing symptoms long after the forehead injury [10]. Although mucoceles are benign; yet, their expansion may lead to bony erosion and extension into the orbit and cranium, leading to ocular and visual complications, and rarely frontal lobe syndrome i.e. mass effect on the frontal lobe [11], meningitis, meningoencephalitis, intracranial abscess, seizures, or cerebrospinal fluid fistula [12]. Very rarely, they will present as a subcutaneous forehead mass or swelling [7], and more rarely they can cause frontocutaneous fistula and a forehead skin ulcer [12]. The endoscopic marsupialization technique could easily be applied even to a very large mucocele that has extended to the intracranial region, without any serious complications [13]. In-office drainage of sinus mucoceles under topical/local anesthesia is well tolerated by patients, especially for mucoceles that were accessible endoscopically in the office setting, in non-anxious patients, aiming to widely open and drain the mucoceles with high success, and low complication rates, even in large mucoceles with bone erosion. Orbital and skull base erosion are not contraindications [14]. External and radical procedures for the treatment of frontal sinus mucoceles have major complications including high surgical morbidity, esthetic concerns of postoperative scar formation, and difficulty in radiologic diagnosis of recurrence after obliteration [13]. Terranova PA, et al. [15] found a complete self-reconstruction of bone that had previously been eroded by the mucocele, in the postoperative CT scan in 66.6% of their patients [15]. There is no need to reconstruct the eroded bone, as sparing the mucoperiosteum is enough to enable the bone to regenerate. No enophthalmos, meningocele, or other facial deformities were noted, despite not having undergone surgical reconstruction of the bone [15]. Other types of cysts related to PNS include aneurysmal bone cysts, Rathke’s cleft cysts (RCC), and epidermoid cysts. An aneurysmal bone cyst is a benign multicystic mass that is locally destructive and rapidly expandable and rare in the sinuses [16]. Rathke’s cleft cyst is a benign epithelium-lined cyst containing mucoid material, typically occurring entirely intrasellar, or intrasellar with suprasellar extension (intra-suprasellar). Extrasellar location is uncommon [17]. Kasliwal MK, et al. [17] reported a rare patient with an intrasphenoidal RCC [17]. Epidermoid cysts are the commonest of head and neck cutaneous cysts Golden BA, et al. [18] found in various regions [19]. In contrast to dermoid, epidermoid cysts do not include skin appendages within their wall [20]. Ren D, et al. [21] reported a huge epidermoid cyst in the maxillary sinus with sinus cavity expansion and sinus wall thinning [21].
Over twenty years we recorded all cases presenting with PNS cysts, their clinical presentations, radiological findings, a management protocol, and surgical outcome to draw attention to those patients with unusual and odd presentations and their management outcomes.
Methods
A retrospective study was done with all patients presenting with PNS cysts to the outpatient clinic were included in the study. Ethical clearance was obtained from the institutional ethical board with ethics committee No. Soh-Med-22-03-30. Informed consent was obtained from all patients who agreed to participate in this study. These patients underwent history-taking, ENT examination, endoscopic examination, computed tomography (CT) scanning of the nose and PNSs, and routine laboratory investigations. They were managed with endoscopic sinus surgery/or a combined approach under general anesthesia, and the postoperative outcome was recorded. Those with serious inflammatory complications were followed up for one year.
Results
Over twenty years, between January 2002 and December 2021, we encountered 54 patients with various PNS cysts. The age range was 7-70 years, with a mean age of 28.6 years, and the male/female ratio was 3:2. Table 1 demonstrated the distribution of these cases. Mucocele/ pyocele was the commonest cyst encountered in the PNSs (43/54=79.6%), followed by radicular cyst (5/54=9.3%), dentigerous cyst (3/54=5.55%), and finally, what we termed fungocele (3/54=5.55%). Most patients presented with an insidious, painless, slowly progressive, disfiguring swelling, and diplopia. Painful swelling was the presenting symptom in 4 patients with pyocele; complicated in one of them with a left orbital pain and orbital cellulitis, and another with a left-sided orbital pain, orbital abscess, and cavernous sinus thrombophlebitis. Two patients with sphenoid fungocele presented with visual deterioration (Figures 1-11).
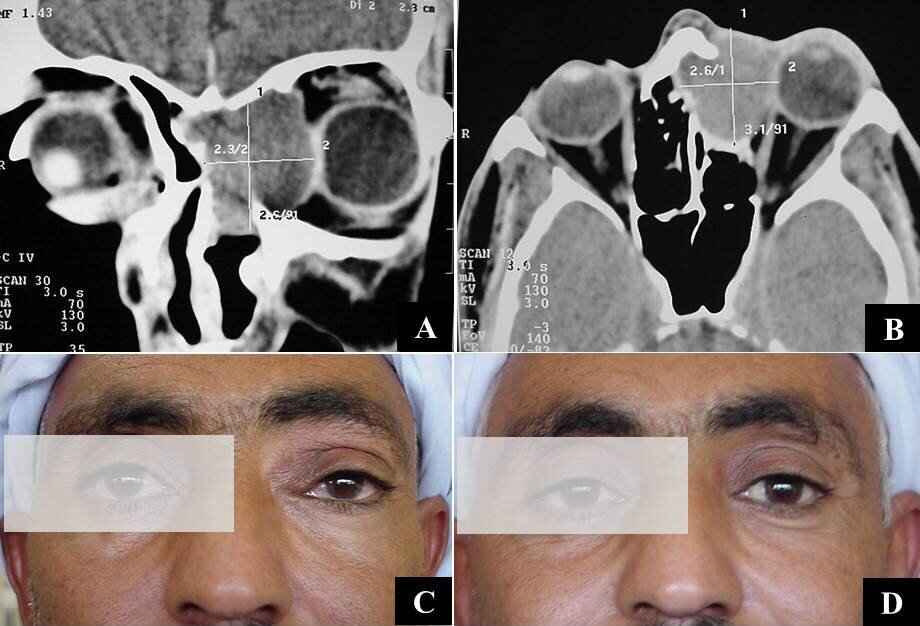
Figure 1: (A) CT scan with a coronal soft tissue cut showing a left fronto-ethmoid mucocele displacing the inter-frontal septum to the right, eroding the sinus floor, and displacing the globe; (B) CT scan with axial soft tissue cut showing the mucocele involving the anterior ethmoid air cells with eroded lamina papyracea and displaced globe; (C) Pre-operative photo showing swelling on the inner aspect of the left globe with down and out proptosis; (D) Postoperative photo 4 days following ESS.
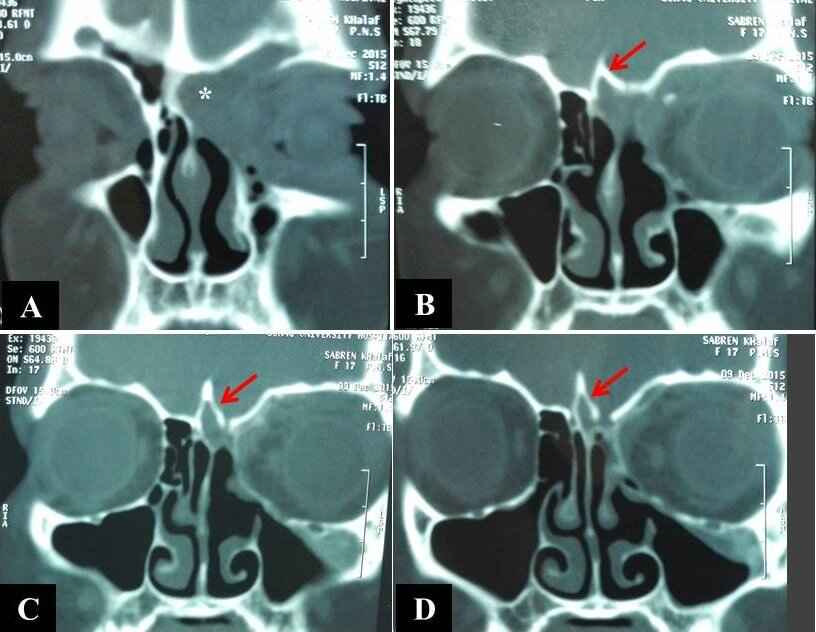
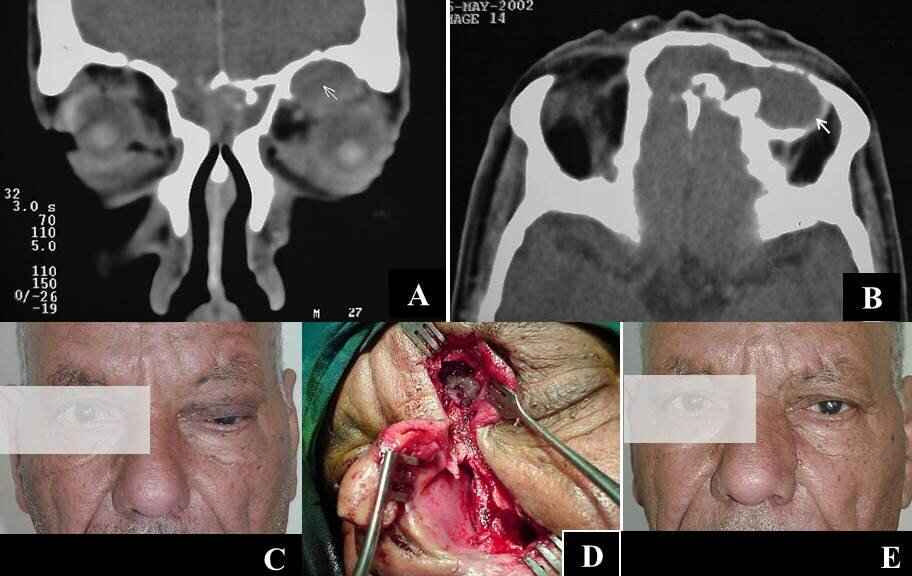
Figure 3: CT scan with coronal (A) and axial (B) soft tissue cuts showing a soft tissue shadow involving both frontoethmoid complexes with an absent inter-frontal septum and eroded posterior wall of right frontal sinus due to inverted papilloma, and a well-defined localized swelling in the medial orbital roof (white arrow) that is in continuity with the soft tissue shadow in the frontal complex (B) that proved to be pyocoele; (C) A preoperative photo showing a left-sided upper lid dusky swelling with a down displacement of the globe and orbital cellulitis; (D) Extended Moure’s lateral rhinotomy with localized frontal osteotomy to facilitate removal of the inverted papilloma that could be seen through the osteotomy; (E) Postoperative photo of the patient two weeks after surgery.
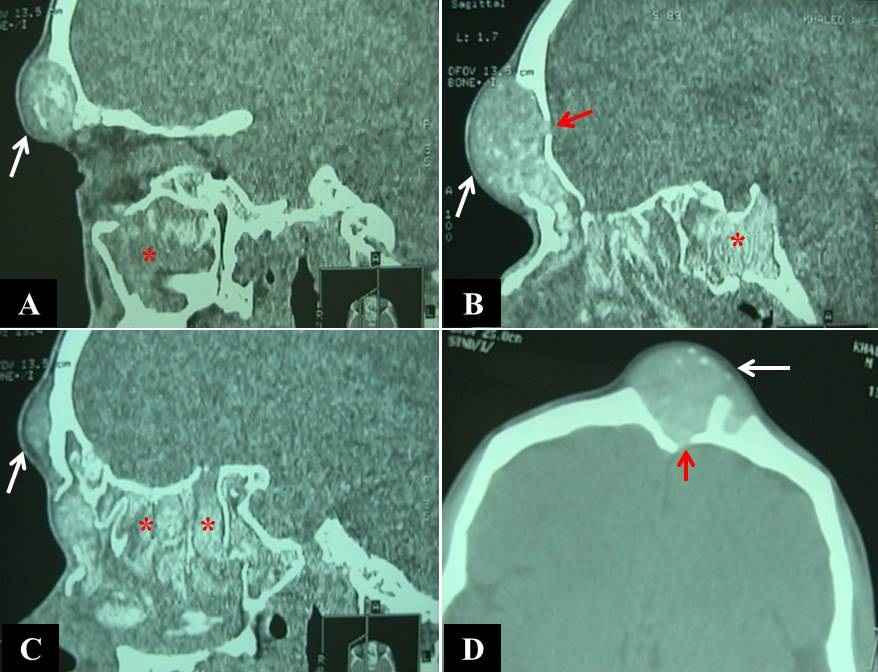
Figure 4: CT scan with sagittal (A, B, C) and axial (D) soft tissue cuts showing a well-defined frontal subcutaneous isodense soft tissue shadow (white arrows), with scattered high-density shadows of AM, with absent anterior walls of frontal sinuses, involving both frontal sinuses (D) with a localized erosion of the posterior wall of the right frontal sinus (red arrows in B, D), that proved to be a fungocele. Note the pan-sinus opacity with scattered high-density shadows of AM (red asterisks) in the maxillary sinus (A), sphenoid sinus (B), and ethmoid air cells (C)
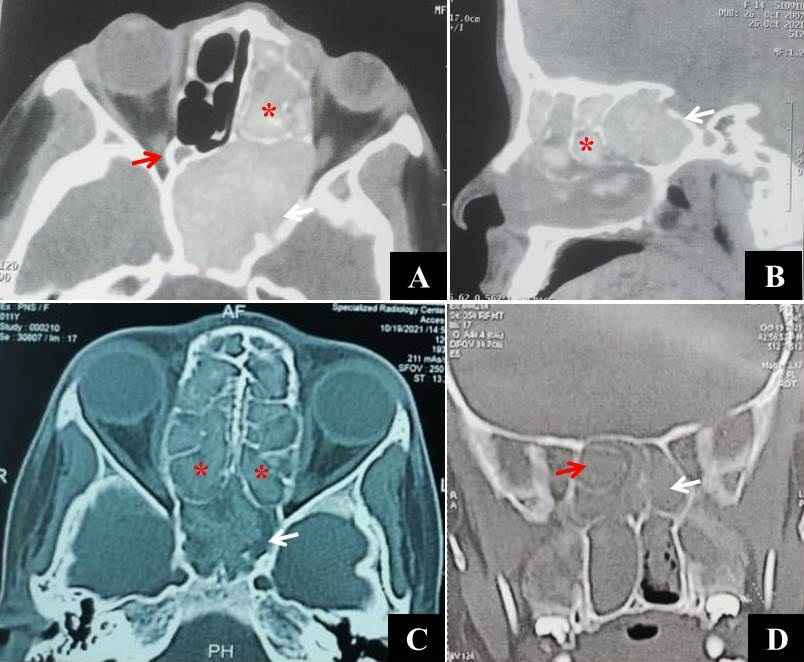
Figure 5: CT scan with axial (A) and sagittal (B) soft tissue cuts showing a left-sided sphenoid fungocele (white arrows), very small right sphenoid sinus (red arrow), and scattered high-density shadows of AM in ethmoid air cells (red asterisks); CT scan with axial (C) and coronal (D) bone window cuts showing a bilateral sphenoid fungocele with an absent inter-sphenoid septum and merged sinuses (white arrows), bilateral AFS involving ethmoid air cells (red asterisks) and left Onodi cell invading the right sphenoid sinus (red arrow in D)
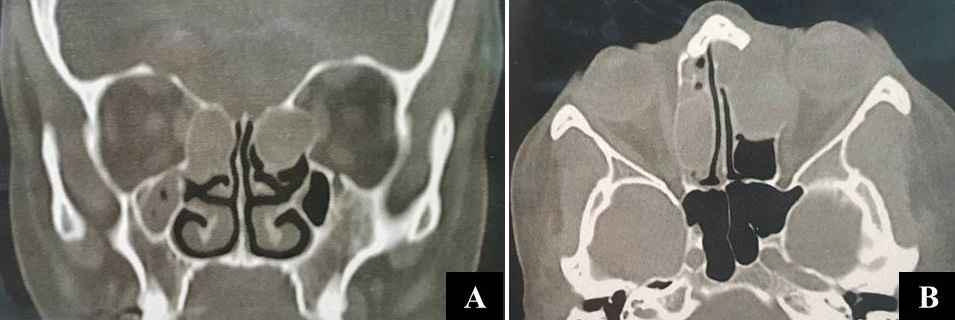

Figure 7: A 50-year-old female having left-sided total ophthalmoplegia due to cavernous sinus thrombophlebitis presented with ptosis and lid edema (A); a left-sided proptosis, orbital cellulitis, and ophthalmoplegia on looking to the right (B), and on looking to the left (C); (D) CT scan with coronal soft tissue cut showing a left-sided ethmoid pyocoele involving a concha bullosa and anterior ethmoid cells (white asterisk) with an erosion of the lamina papyracea, and a well-defined soft tissue shadow on the upper medial wall and roof of the orbit (red asterisk) due to sub-periosteal abscess; (E, F) Postoperative photos of the patient showing resolution of orbital cellulitis and regain of ocular motility on looking to the right and left.
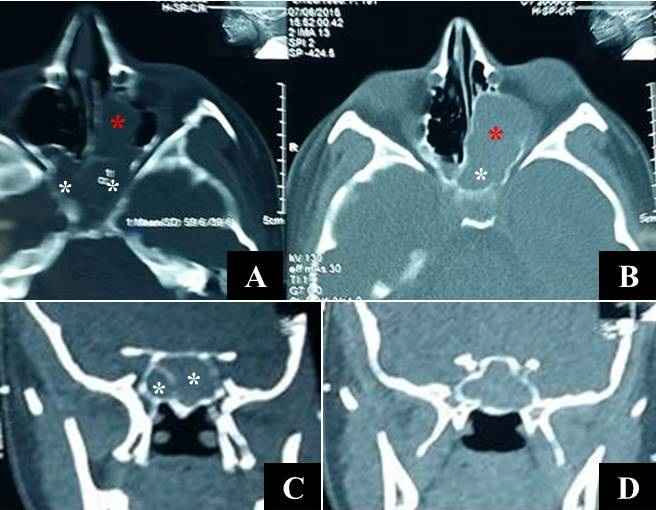
Figure 8: CT scan with axial bone window cut (A) and axial soft tissue cut (B) showing a mucocele involving both sphenoid sinuses with a smaller right and a larger left sphenoid sinus (white asterisks), and involving the left posterior ethmoid air cells (red asterisks). Note the partially eroded inter-sphenoid septum and anterior face of the left sphenoid sinus; CT scan with coronal soft tissue cuts showing mucocele involving both sphenoid sinuses (white asterisks) with a partially eroded inter- sphenoid septum and a smaller right sphenoid (C), and merged both sphenoid sinuses with an absent inter-sinus septum and distended both lateral walls (D).

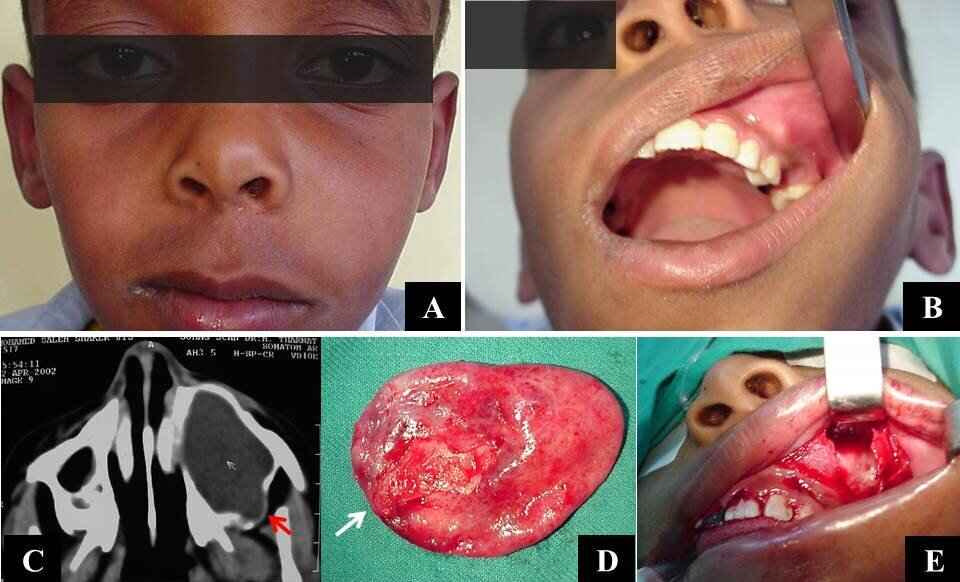
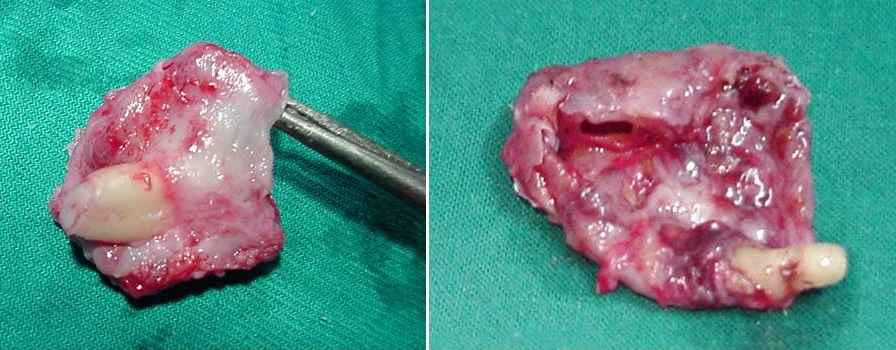
Figure 10: A nine-year-old boy with a left-sided cheek swelling caused by a radicular cyst (A), with obliteration of the left buccoalveolar sulcus, expansion of the anterior maxillary wall, and a carious upper left 2nd premolar tooth seen through the open mouth (B); (C) CT scan with axial soft tissue cut showing distension of the left maxillary sinus by the cyst with thinning out and erosion of the posterolateral maxillary wall (red arrow); (D) A photo of the removed cyst by enucleation; note the site of tooth reaction in the cyst wall (white arrow); (E) Operative photo showing a distended anterolateral maxillary wall with a window created in it through a sub-labial approach, with the cyst removed, and the sinus cavity seen.
| Cyst type | Site of origin | Number | Males | Females | Approach |
|---|---|---|---|---|---|
| Mucocele | Frontal | 3 | 2 | 1 | ESS |
| Frontoethmoid | 24 | 16 | 8 | ||
| Ethmoid | 9 | 5 | 4 | ||
| Maxillary | 1 | 0 | 1 | ||
| Sphenoid (bilateral in one) and left posterior ethmoid | 2 | 0 | 2 | ||
| Pyocoele | Frontal | 2 | 2 | 0 | 1 ESS |
| 1 CA | |||||
| Ethmoid (bilateral in one) | 2 | 0 | 2 | ESS | |
| Fungocoele | Bilateral frontal sinuses | 1 | 1 | 0 | ESS |
| Bilateral sphenoid sinuses | 1 | 0 | 1 | ||
| Left sphenoid sinus | 1 | 0 | 1 | ||
| Radicular cyst | Maxillary | 5 | 4 | 1 | CA |
| Dentigerous cyst | Maxillary | 3 | 2 | 1 | |
| Total | 54 | 32 | 22 |
Table 1: Distribution of patients with PNS cysts over twenty years.
ESS: endoscopic sinus surgery; CA: combined approach. Table 1: Distribution of patients with PNS cysts over twenty years.
The frontal sinus was the commonest sinus of PNS cyst origin in 30/54 cases (55.6%), being exclusively frontal in 6/30 cases (20%), and extending to involve the anterior ethmoid air cells forming frontoethmoid mucocele (FEM) in 24/30 (80%) cases (Figure 1). One of our patients with FEMs presented with a right-sided FEM at the age of 7 years that was managed with ESS, and eleven years later developed a left-sided FEM. A pneumatized crista Galli was involved as a part of FEM in one patient (Figure 2). Among the six patients with exclusive frontal sinus cysts, three had mucocele;
two had pyocele, and one of them developed secondary to inverted papilloma involving both frontoethmoid complexes with a left frontal pyocoele and orbital cellulitis (Figure 3). This patient was managed with a combined extended Moure’s lateral rhinotomy and endoscopic sinus surgery (ESS) to facilitate the removal of the neoplasm and drainage of the pyocele. The patient achieved an excellent postoperative outcome with the resolution of the orbital cellulitis. The last case with exclusive frontal cyst presented by January 2014 with bilateral extensive allergic fungal sinusitis (AFS)
with pan-sinus involvement, and a large, non-tender, frontal subcutaneous doughy cystic swelling originating from both frontal sinuses, with absent anterior frontal walls, and an erosion in the right posterior frontal wall (Figure 4). He was managed with ESS, and the swelling was found to contain a viscid gelled mucoid discharge admixed with allergic mucin (AM); hence we termed it a fungocele, a nomenclature that was recorded for the first time in the literature. By 2001, we faced another 2 cases with sphenoid fungocele. The first was an 11-year female child who presented with bilateral deterioration of vision down to 6/24, bilateral AFS involving all PNSs, and a fungocele involving both sphenoid sinuses that merged. The second was a 14-year female child who presented with a left-sided AFS involving all the PNSs, a left sphenoid fungocele, a left proptosis, and left deterioration of vision down to 1/60 (Figure 5).
The ethmoid air cells were the sinus of cyst origin in 11/54 cases (20.4%). In all of them, the anterior ethmoid cells were involved, with 9 mucoceles and two pyoceles. One of the latter cases presented with bilateral ethmoid pyoceles and left-sided proptosis (Figure 6). The second presented with a left-sided pyocele complicated with orbital abscess and cavernous sinus thrombophlebitis (Figure 7). This patient was managed with ESS with a dramatic postoperative improvement, resolution of orbital abscess, and regain of ocular motility. We observed that 26/37 (70.3%) of ethmoid involvement occurred by extension from other PNSs, mostly the frontal sinus (24/26=92.3%), and only two from the sphenoid sinus. Among the ethmoid air cells, the anterior ethmoid cells were involved in 35/37 cases (94.6%), while the posterior ethmoid cells were involved in only 2/37 cases (5.4%) by extension from the sphenoid sinuses (Figure 8).
The maxillary sinus was involved with cystic swelling in 9/54 (16.6%) cases, one of them was a mucocele expanding the sinus, and presenting with a right cheek swelling and proptosis (Figure 9). This patient was managed with ESS. The remaining 8 cases were cysts of dental origin; 5 were radicular cysts related to a carious upper tooth and expanding the maxillary sinus with a disfiguring cheek swelling (Figure 10) and 3 were dentigerous cysts expanding the sinus with a missed tooth included in the cyst wall (Figure 11). All odontogenic cysts were managed with a Caldwell-luc’s approach combined with ESS to facilitate cyst enucleation, extraction of the offending carious tooth in case of radicular cysts, and performing a middle meatal antrostomy.
The sphenoid sinus was the ‘least’ sinus of cyst origin in 4/54 (7.4%) of our cases; 2 were mucoceles, and in one of them, the cyst involved both sphenoid sinuses mainly the left (Figure 8). In both cases, the sphenoid mucocele extended to involve the left posterior ethmoid cells forming spheno-ethmoid mucocele. The other 2 sphenoid cysts were fungoceles, in one of them involved both sphenoid sinuses that merged (Figure 5).
Discussion
There are several types of PNS cysts that have been recorded in the literature; mucocele/pyocele is by far the most prevalent, followed by cysts with a dental origin [22, 23, 24]. In our series, mucocele/pyocele formed 79.6% of PNS cysts, followed by odontogenic cysts in 14.8% of cases, with the radicular cysts being commoner than PNS dentigerous cysts (5:3) this coincides with previous studies about the prevalence of the cysts of the jaw [25, 26, 27]; lastly, fungocele in only 5.6%. The frontal sinus was the commonest sinus of cyst origin (30/54=55.6%), owing to its distinct ostium anatomy that is vulnerable to obstruction by various pathologies including inflammatory, traumatic, and neoplastic lesions, with the inflammatory one being the commonest cause of ostium obstruction and cyst formation as stated previously by Wilkerson [28]. In 88.9% of our cases with frontal sinus mucocele (24/27 cases), it extended to involve the anterior ethmoid air cells forming FEM. This involvement could be explained by the close vicinity of the anterior ethmoid cells to the frontal sinus ostium this is in accordance with other published articles reporting the anatomic distribution of mucoceles [29, 30, 31]. According to several reports, isolated sphenoid mucoceles may occur in 1% - 3% of cases, this resembles our series in which, there were 2 sphenoid mucoceles (3.7%) [32, 33]. Fungocele is a nomenclature that is recorded for the first time in the literature. It also involved the sphenoid sinus in 2 of our cases. Sphenoid fungocele was more serious and presented in a young age group with visual deterioration.
Paranasal sinus cysts of unusual sites of origin were observed in 6 of our cases. Interestingly enough, all were females. Four of these were mucoceles, one involving a pneumatized crista Galli as a part of FEM, one involving the maxillary sinus, and two involving the sphenoid sinuses and left posterior ethmoid. Few previous reports of mucocele involving a pneumatized crista Galli were found in the literature [34, 35]. The remaining two were fungocele involving sphenoid sinus. We could find no sound explanation for this gender predilection. Despite the rarity of bilateral involvement, Only a few reports have been recorded in the literature [36, 37, 38, 39], in the present study bilateral PNS cysts were encountered in five patients, one had bilateral frontal fungocele, the second had bilateral ethmoid pyoceles, the third had bilateral sphenoid mucocele, the fourth had bilateral sphenoid fungocele and the fifth had a right-sided FEM, followed eleven years later by a left-sided one.
Among our series, we met no case with post-traumatic mucocele contrary to Kojima, et al. [10] who reported posttraumatic mucocele in 5/68 (7%) of their patients [40].
Paranasal sinus cysts have a benign course, presenting with painless disfiguring swelling in most cases, frequently with diplopia; yet, serious complications could occur if get infected and with those with sphenoid fungocele. We faced four serious cases, one with an ethmoid pyocele complicated with orbital abscess, cavernous sinus thrombophlebitis, and total ophthalmoplegia. The second patient had an underlying unusual, high-up, inverted papilloma involving both fronto- ethmoid complexes with a left-sided frontal pyocele that extended into the orbit with orbital cellulitis. Both cases could be controlled, with rapid postoperative recovery and resolution of all deficits. To our knowledge, this is the first reported case in the literature of inverted papilloma involving bilateral frontoethmoid complex, and complicated with frontal pyocele and orbital cellulitis. The remaining two serious cases had sphenoid fungocele with visual deterioration that reached 1/60 in one of them.
Odontogenic cysts presented with painless slowly progressive maxillary sinus expansion with a disfiguring cheek swelling, related to a carious tooth in those with radicular cysts (5 cases) or a missed tooth in those with dentigerous cysts (3 cases). These odontogenic cysts could easily be enucleated through Caldwell-Luc’s approach combined with ESS with a good outcome.
In contrast to obliterative techniques, endoscopic marsupialization is now the surgical method of choice for treating most paranasal sinus cysts [40, 41, 42]. This study, which shows no complication recorded and low recurrence rates (1/54=1.9%, with FEM that could be controlled with revision marsupialization with ESS ), are similar to those of the previously published series, supporting the idea that the endoscopic approach is still a successful and safe mode of treatment and ought to be used for the majority of these patients. The endoscopic method reduces morbidity while also restoring mucociliary clearance, which permits ongoing endoscopic and radiographic evaluation of the operated sinus until the sinus returns to normal function.
Conclusion
The frontal sinus was the commonest sinus of PNS cyst origin. With exclusive frontal sinus involvement, it is essential to look for possible underlying pathology or associated complication. Fungocele, a new nomenclature, could complicate those with AFS. Sphenoid fungocele could lead to serious deterioration of vision. Ethmoid air cells are involved with mucocele mostly by extension from other sinuses, predominantly the frontal sinus. The anterior ethmoid cells were the commonest to be involved with mucocele/pyocele in 94.6% of cases, while the posterior ethmoid cells were involved in 5.6% of cases by extension from the sphenoid sinus. Patients with mucocele should be followed up for possible development of another cyst on the contralateral side. All cases of PNS cysts could be controlled successfully with ESS except those with an underlying neoplastic lesion (one case) or odontogenic cysts; both required a combination of the external approach with ESS.
Acknowledgments: Not applicable.
Author Contributions: RHS: Contributed to overall study design and ethics application. AAA: data collection and overall statistical analysis of the data. KGD: complete paper write-up, including the development of manuscript figures. All authors read and approved the final manuscript.
Funding
There were no financial sources of funding to declare by any of the authors. Availability of data and materials: The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declarations
Ethics Approval and Consent to Participate: Study design and methodology were reviewed and affirmed by the local Institutional Review Boards No. Soh-Med-22-03-30, Faculty of Medicine. Consent for Publication: All presentations of case reports must have consent for publication. Competing Interests: The authors declare no competing financial or non-financial interests
References
-
Krishnamurthy V, Haridas S, Garud M, Vahanwala S, Nayak CD, et al. (2013) Radicular cyst masquerading as a multilocular radiolucency. Quintessence Int 44(1): 71- 73.
-
Pekiner FN, Borahan O, Ugurlu F, Horasan S, Sener BC, et al, (2012) Clinical and radiological features of a large radicular cyst involving the entire maxillary sinus. Clinical and Experimental Health Sciences 2(1): 31.
-
Önay O, Süslü AE, Yılmaz T (2019) Huge dentigerous cyst in the maxillary sinus: a rare case in childhood. Turk Arch Otorhinolaryngol 57(1): 54.
-
Guruprasad Y, Chauhan DS, Kura U (2013) Infected dentigerous cyst of maxillary sinus arising from an ectopic third molarJ Clin Imaging Sci 3(S1): 7.
-
Marcotullio D, Iannella G, Zelli M, Marinelli C, Magliulo G (2014) Rare and massive odontogenic parakeratotic cyst treated by endoscopic sinus surgery: a case report. J Med Case Rep 5(8): 293.
-
Tkaczuk AT, Bhatti M, Caccamese JF, Ord RA, Pereira KD (2015) Cystic lesions of the jaw in children: a 15-year experience. JAMA Otolaryngol Head Neck Surg 141(9): 834-839.
-
Carmichael RA, Kang DR (2015) Frontal sinus mucopyocele presenting as a subcutaneous forehead mass. Journal of Oral and Maxillofacial Surgery 73(11): 2155-2161.
-
Cheon YI, Hong SL, Roh HJ, Cho KS (2014) Fungal ball within Onodi cell mucocele causing visual loss. J Craniofac Surg 25(2): 512-514.
-
Rimmer J, Beale T, V Lund (2015) Visual loss in patients with sphenoethmoidal cells. J Laryngol Otol 129(2): 198-201.
-
Kojima Y, Tsuzuki K, Yukitatsu Y, Oka H, Takebayashi H, et al. (2015) Clinical features of patients treated with endoscopic sinus surgery for posttraumatic paranasal sinus mucocele. ORL J Otorhinolaryngol Relat Spec 77(3): 162-170.
-
Weidmayer S (2015) Frontal mucocele with intracranial extension causing frontal lobe syndrome. Optom Vis Sci 92(6): e138-e142.
-
Altıntaş Kakşi S, Kakşi M, Balevi A, Özdemir MH, Erdoğan Çakır A (2014) Unusual case of frontal mucocele presenting with forehead ulcer. Dermatol Online J 20(11): 13030.
-
Aydin S, Demir MG (2014) Complicated giant mucoceles of the frontal sinus: approach to endoscopic marsupialization technique. J Craniofac Surg 25(5): e461-e463.
-
Barrow EM, DelGaudio JM (2015) In‐office drainage of sinus mucoceles: An alternative to operating‐room drainage. Laryngoscope 125(5): 1043-1047.
-
Terranova P, Karligkiotis A, Digilio E, Basilico F, Bernardini E, et al. (2015) Bone regeneration after sinonasal mucocele marsupialization: What really happens over time? Laryngoscope 125(7): 1568-1572.
-
Hashemi SM, Heidarpour M, Eshaghian A, Ansari P, Hashemi MS, et al., (2015) A rare case of aneurysmal bone cyst in the paranasal sinus. Iran J Otorhinolaryngol 27(82): 395-399.
-
Kasliwal MK, Dua SG, Harbhajanka A, Nag S, Jhaveri MD, et al. (2015) Intrasphenoidal Rathke’s cleft cyst. J Clin Neurosci 22(10): 1678-1682.
-
Golden BA, Zide MF (2005) Cutaneous cysts of the head and neck. J Oral Maxillofac Surg 67(1): 52-57.
-
Yanai A, Okabe K, Nakamura Y (1987) Epidermal cyst originating from the preauricular sinus. Plast Reconstr Surg 79(2): 265-266.
-
Yılmaz I, Yılmazer C, Yavuz H, Bal N, Ozluoglu LN (2006) Giant sublingual epidermoid cyst: a report of two cases. J Laryngol Otol 120(3): 1-4.
-
Ren D, Pan H, Zheng X (2014) Right maxillary sinus epidermoid cyst huge: report of 1 case. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 28(15): 1179-1180.
-
SCHUKNECHT HF, LINDSAY JR (1949) Benign cysts of the paranasal sinuses. Archives of Otolaryngology 49(6): 609-630.
-
Moon IJ, Kim SW, Han DH, Shin JM, Rhee CS, et al. (2011) Mucosal cysts in the paranasal sinuses: long-term follow- up and clinical implications. Am J Rhinol Allergy 25(2): 98-102.
-
Pierse JE, Stern A (2012) Benign cysts and tumors of the paranasal sinuses. Oral Maxillofac Surg Clin North Am 24(2): 249-264.
-
Shear M, Speight P (2008) Cysts of the oral and maxillofacial regions, John Wiley & Sons: 549-575.
-
Lee HK, Ryu KS, Kim MG, Park KW, Kim RG, et al. (2014) Retrospective Study of Cysts in the Oral and Maxillofacial Regions: Statistical and Clinical Analysis. J Korean Assoc Maxillofac Plast Reconstr Surg 36(1): 1-6.
-
Fomete B, Osunde OD, Ogbeifun J, Agbara R, Ononiwu CN (2016) A 10-year retrospective analysis of 64 cases of cystic lesions of the oral and maxillofacial region in a Nigerian tertiary hospital. Oman Med J 31(6): 434.
-
Wilkerson Jr W (1945) Mucocele of the nasal accessory sinuses. The Laryngoscope 55(6): 294-308.
-
Natvig K, Larsen TE (1978) Mucocele of the paranasal sinuses: A retrospective clinical and histological study. J Laryngol Otol 92(12): 1075-1082.
-
Lloyd G, Lund VJ, Savy L, Howard D (2000) Optimum imaging for mucoceles. J Laryngol Otol 114(3): 233-236.
-
Lee TJ, Li SP, Fu CH, Huang CC, Chang PH, et al. (2009) Extensive paranasal sinus mucoceles: a 15-year review of 82 cases. Am J Otolaryngol 30(4): 234-238.
-
Stankiewicz JA (1989) Sphenoid sinus mucocele. Archives of Otolaryngology–Head & Neck Surgery 115(6): 735-740.
-
Barat J, Marchal J, Bracard S, J Auque S, Lepoire J (1990) Mucoceles of the sphenoidal sinus. Report of six cases and review of the literature. J Neuroradiol 17(2): 135- 151.
-
Cervantes SS, Lal D (2014) Crista galli mucocele: endoscopic marsupialization via frontoethmoid approach. Int Forum Allergy Rhinol 4(7): 598-602.
-
Shidanshid M, Taghi AS, Kuchai R, Saleh HA (2015) Endoscopic resection of a mucocele of the crista galli. Ear Nose Throat J 94(9): E23-25.
-
Malhotra R, Wormald PJ, Selva D (2003) Bilateral dynamic proptosis due to frontoethmoidal sinus mucocele. Ophthalmic Plast Reconstr Surg 19(2): 156-157.
-
Caylakli F, Yavuz H, Cagici AC, Ozluoglu LN (2006) Endoscopic sinus surgery for maxillary sinus mucoceles. Head Face Med 2(1): 29.
-
Sakae FA, Araújo Filho BC, Lessa M, Voegels RL, Butugan O (2006) Bilateral frontal sinus mucocele. Revista Brasileira de Otorrinolaringologia 72(3): 428.
-
Bahgat M, Bahgat Y, Bahgat A (2012) Sphenoid sinus mucocele. Case Reports 2012: bcr2012007130.
-
Har El G (2001) Endoscopic management of 108 sinus mucoceles. Laryngoscope 111(12): 2131-2134.
-
Khong JJ, Malhotra R, Selva D, Wormald PJ (2004) Efficacy of endoscopic sinus surgery for paranasal sinus mucocele including modified endoscopic Lothrop procedure for frontal sinus mucocele. J Laryngol Otol 118(5): 352-356.
-
Woodworth BA, Harvey RJ, Neal JG, Palmer JN, Schlosser RJ (2008) Endoscopic management of frontal sinus mucoeceles with anterior table erosion. Rhinology 46(3): 231-237.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?