Coblation Versus Microdebrider Assisted Adenoidectomy - Analysis of Post-Operative Outcome
Aims and Objectives: To compare the postoperative results in coblation assisted adenoidectomy versus microdebrider assisted adenoidectomy. Materials & Methods: The current prospective project was conducted in 100 patients from Jan 2017 to Dec 2019. 50 patients each were enrolled in the coblation and microdebrider group and their postoperative analysis was done on basis of their pain scoring and their length of hospital stay. Results: Postoperative pain scores as assessed by Wong Baker pain scale (where 0 is no pain and10 showed maximum pain) at various intervals showed significantly higher pain scores at all times in coblation assisted adenoidectomy as compared to microdebrider assisted surgery (p<0.000). The children in microdebrider group had faster recovery and were discharged earlier from the hospital as compared to the coblation group (p<0.05). Conclusion: In this study we concluded that microdebrider had better postoperative outcome in terms of lesser pain and early patient recovery in comparison to coblation group.
Introduction
Adenoid, which forms the uppermost limit of Waldeyer’s ring is an important component of the lymphoid system and is generally hypertrophied in children with frequent upper respiratory catarrh. It is the main culprit which leads to obstruction and frequent respiratory and breathing problem in paediatric population.
Adenoidectomy is a routinely performed procedure in children experiencing obstructive symptoms due to its enlargement. The technique of performing this procedure has evolved over the years from the application of cold steel instruments to powered instruments like microdebrider and coblation.
The main limitation faced while performing adenoidectomy with a curette was the lack of exposure of adenoids as it was performed in a blind fashion, also due to the shape of the curette it was unable to access certain areas of nasopharynx like choanal part and roof area leading to inadequate removal and other complications such as bleeding, eustachian tube scarring etc. Many workers started to use endoscopes, so that the surgery could be performed precisely without traumatising the surrounding tissues. Later, instruments such as electrocautery, coblation and microdebrider etc. were used for better surgical results and fewer complications [1, 2, 3, 4].
Microdebrider assisted adenoidectomy commonly known as powered adenoidectomy has been a popular technique since the introduction of debrider for the use of nasal procedures such as endoscopic sinus surgery. The postoperative results achieved have been quiet promising. But many surgeons became fascinated by the technology of coblation as it has been introduced recently in ENT practice for the removal of tonsils. Gradually, coblation found its way from tonsillectomy to adenoidectomy, turbinectomy, laryngeal procedures etc. The principle on which it worked was non-heat-driven process and it works at a lower temperature, that is, 40°C to 70°C [5, 6]. Energy produced is used to excite electrolytes in a conductive medium to create a precisely focused plasma that has a cutting as well as coagulation action. Very few studies have been conducted in the literature comparing the microdebrider and coblation as a technique for adenoidectomy as both have been recently introduced in ENT surgical practice, hence we planned this study with the basic idea of establishing the better technique. Coblation has gained popularity among the surgeons due to its dual action of cutting and coagulating the tissue in comparison to microdebrider which has a cutting action alone. In the present study the primary aim was to compare the intensity of postoperative pain associated with both the techniques that is coblation versus microdebrider assisted adenoidectomy. Comparison was also made of the duration of hospitalisation required following the use of both the techniques.
Methods and Material
This study was conducted at our ENT and Head & Neck Centre from the year Jan 2017 to Dec 2019 on a total of 100 children within the age group of 4-12 years of age. Ethical clearance was obtained from the institutional ethical committee and an informed written consent was taken from the attendants of all the patients.
Children presenting with the signs of adenoid hypertrophy and getting recurrent episodes of adenoiditis and who were especially planned for adenoidectomy alone, were included in the study. Patients of craniofacial malformations like Down’s syndrome, cleft palate, palatal insufficiency, severe anemia and those requiring tonsillectomy with adenoidectomy were excluded from the study.
After obtaining detailed history and conducting clinical examination, assessment of adenoid size was carried out by X-ray nasopharynx lateral view. Patients planned for adenoidectomy were divided into two groups of fifty children each, microdebrider group and coblation group, by using the computerised generated table of randomisation viz: if the last digit of the random number was from 0 to 4, the patient was assigned to microdebrider assisted adenoidectomy (group M) while if the last digit was from 5 to 9 the child was assigned to coblation assisted adenoidectomy (group C).
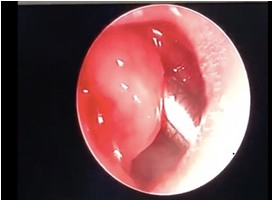
The procedure was performed transorally with endoscopic visualization of the adenoid. In patients of microdebrider adenoidectomy, a microdebrider with a 90° curved blade was used (Figure 1). The instrument was connected to an aspirator and was programmed to alternate rotations, with a rotational speed of 1200 rpm.
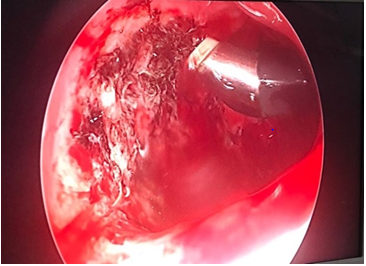
The coblation procedure was performed at a power of 7 and 3 with an Evac70 wand (Smith & Nephew Inc., London, UK) in children less than 5 years of age, and a Procise Max wand (Figure 2) (Smith & Nephew Inc., London, UK) in children over 5 years of age. No electrocautery was used in both the procedures, bleeding was controlled using packing in Group 1(M) patients and in Group 2 (C) coblation wand itself was used to control the bleeding. The patients of Group I (M) in which cautery and coblation wand was used to control bleeding were excluded from the study. Postoperative assessment for intensity of pain was done at 8hours, 24 hours while the child was still in the hospital, then at 72 hours and 1 week at follow up visit in both the groups. On the basis of their timing of discharge patients were categorised as early (24 hours) and late discharge (more than 24 hours) (Figure 3).
The postoperative pain assessment was based on the Wong-Baker FACES pain rating scale. This pain scale model was found to be the most appropriate as compared to others as it encompassed all the age categories children included in the study (Figure 1). The 0 on the scale represented no pain, 2 and 4 represented mild pain, 6 and 8 moderate intensity pain and 10 were the worst pain possible. This scale was designed by Donna Wong and Connie Baker in 1983.
Results
The statistical analysis of both the groups was carried out using IBM spss software, version 21. Data was analysed as categorical variables using Pearson Chi-square test and Fisher’s exact test. Level of significance (α) was set at 5%. Hence, a p<0.05 was accepted as statistically significant.
Patients were analysed according to their age group, gender, timing of discharge (early or late) and pain score. In a total of 100 patients 70 were male and 30 were female. The demographic evaluation revealed the age groups of patient presenting in both the groups were similar 7.86 ± 3.201(group 1) and 8.46± 3.418 (group 2) (Table 1) (p<0.367). The preoperative assessment of adenoid size on the basis of X-ray was compared and it was seen that in both the groups the maximum patients operated had an adenoid size of grade 3 (group 1 – 31, group 2 -34), (p value 0.52)
| Group | N | Mean | Std. Deviation | Std. Error Mean | |
|---|---|---|---|---|---|
| Age | 1 (M) | 50 | 7.86 | 3.201 | 0.453 |
| 2 (C) | 50 | 8.46 | 3.418 | 0.483 |
Table 1: Mean Age Distribution in the Two Groups.
Patients were categorized according to their length of stay at the hospital, patients discharged within 24 hours’ time frame after performing the procedure were categorised as early discharge and patients who were discharged 72 hours or more postoperatively were labelled as late discharge. In group 1 (M) 45 patients were discharged early and 5 were discharged late and in group 2 (C) out of 50 around 35 patients were discharged early and 15 were discharged late as seen in (Table 2) (p value < 0.05)
| Group | Total | ||||||
|---|---|---|---|---|---|---|---|
| 1 (M) | 2 (C) | ||||||
| Chi-Square Tests | |||||||
| Early_Late_discharge | E | Count | 45 | 35 | 80 | ||
| % within Group | 90.00% | 70.00% | 80.00% | ||||
| L | Count | 5 | 15 | 20 | |||
| % within Group | 10.00% | 30.00% | 20.00% | ||||
| Total | Count | 50 | 50 | 100 | |||
| % within Group | 100.00% | 100.00% | 100.00% | ||||
| Value | df | Asymp. Sig. 2-sided) | Exact Sig. (2-sided) | Exact Sig. (1-sided) | |||
| Pearson Chi-Square | 6.250a | 1 | 0.012 | ||||
| Continuity Correction | 5.063 | 1 | 0.024 | ||||
| Likelihood Ratio | 6.486 | 1 | 0.011 | ||||
| Fisher's Exact Test | 0.023 | 0.011 | |||||
| N of Valid Cases | 100 | ||||||
| a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 10.00. | |||||||
| b. Computed only for a 2x2 table | |||||||
Table 2: Distribution of Patients According to Early and Late Discharge in two Groups.
Another important and the most vital parameter that was analysed in terms of efficacy of the procedure was the pain score. Using the Wong baker scale pain score was divided into three main categories (mild, moderate and severe), where the pain score of 2 and 4 on the chart was labelled as mild pain, score of 6 and 8 as moderate and score of 10 on chart represented severe type of pain. The pain score was evaluated at 24 hours, 72 hours and 1 week postoperatively. The assessment revealed that during the first initial 24 hours, severe pain score of 10 was noted in
84% patients of group 1(M), 94% patients in group 2 ( C) respectively (Table 3). In the next 72 hours a moderate pain score of 6 was noted in 96% patients in group 1(M) while in group 2 (C), we witnessed a severe pain score of 10 in 84%, (p< 0.0001 highly significant) (Table 4). At the end of 1 week, group 1 (M) 90% patients revealed a pain score of 2 (mild) and in group 2 (C), 78% patients had a moderate score of 6 and 14% with a mild score of 2. (table 5) (p<0.000 highly significant)
| Group | Total | ||||
| 1(M) | Total | 2(C) | |||
| Wong baker 24 | 8 | Count | 8 | 3 | |
| % within Group | 16.00% | 6.00% | |||
| 10 | Count | 42 | 47 | ||
| % within Group | 84.00% | 94.00% | |||
| Total | Count | 50 | 50 | 100 | |
| % within Group | 100.00% | 100.00% | 100.00% |
| Chi-Square Tests | |||
|---|---|---|---|
| Value | df | Asymp. Sig. (2-sided) | |
| Pearson Chi-Square | 81.507a | 2 | 0 |
| Likelihood Ratio | 101.954 | 2 | 0 |
| Linear-by-Linear Association | 69.89 | 1 | 0 |
| N of Valid Cases | 100 | ||
| a. 2 cells (33.3%) have expected count less than 5. The minimum expected count is 4.00. | |||
Table 4: Postoperative Distribution of Patients According to their Pain Score in First 24 Hour Period in two Groups.
| Group | Total | ||||
| 1(M) | Total | 2(C) | |||
| WONG BAKER 72 | 6 | Count | 48 | 0 | |
| % within Group | 96.00% | 0.00% | |||
| 8 | Count | 2 | 8 | ||
| % within Group | 4.00% | 16.00% | |||
| 10 | Count | 0 | 42 | ||
| % within Group | 0.00% | 84.00% | |||
| Total | Count | 50 | 50 | 100 | |
| % within Group | 100.00% | 100.00% | 100.00% |
| Chi-Square Tests | |||
|---|---|---|---|
| Value | df | Asymp. Sig. (2-sided) | |
| Pearson Chi-Square | 100.000a | 3 | 0 |
| Likelihood Ratio | 138.629 | 3 | 0 |
| Linear-by-Linear Association | 94.395 | 1 | 0 |
| N of Valid Cases | 100 | ||
| a. 4 cells (50.0%) have expected count less than 5. The minimum expected count is 2.00. | |||
Table 6: Postoperative Distribution of Patients According to their Pain Score in 72 Hour Period in two Groups.
Discussion
Adenoid hypertrophy leads to clinical manifestations in the form of recurrent upper respiratory catarrh and sleep disorders in the paediatric population. Hence, adenoidectomy has been a very popular surgical procedure performed in the younger age group. Recently the application of coblation and microdebriders has been widely tested in numerous ENT procedures ranging from tonsillectomy, FESS, laryngeal web and adenoidectomy. The limitation of cold steel dissection using curettes lead to the introduction of endoscopes, microdebriders and coblation to achieve better results and reduce the postoperative complications.
In this study we compared the coblation and microdebrider in terms of efficacy, postoperative pain and hospital stay in patients undergoing adenoidectomy. In each group 50 patients were assigned, group 1 patients underwent microdebrider assisted adenoidectomy and group II underwent coblation adenoidectomy. The hospital stay in both the groups was compared and group 1 (M) patients revealed an early postoperative recovery as compared to the coblation group (2) (Table 2, p < 0.05). The postoperative recovery time depends on various factors such as systemic antibiotic consumption, patient discomfort, oral intake and patient mobilisation. In coblation since the hemostasis part was taken care by the wand itself which in turn resulted in charring of tissues and large slough formation (Figure 2). Hence, prolonged use of intravenous antibiotics was required in group 2(C) patients. On the contrary in microdebrider group the hemostasis part was achieved by packing, leading to zero thermal injury to the tissues and hence reducing the requirement of injectables and resulting in early patient mobilisation and early hospital discharge. In a study by El Rahman, et al. [7], coblation was compared with conventional curette technique and an early resolution and recovery was seen in coblation group children. Another study where coblation was compared to microdebrider in patients undergoing adenoidectomy revealed similar recovery time in both the groups of patients. They found similar recovery pattern in both the techniques due to the use of electrocautery for achieving hemostasis in microdebrider patients, hence resulting in thermal injury which occurred in coblation group as well [8].
The postoperative pain score and early pain resolution is an important indicator of efficacy of a procedure and group 1 (M) patients showed a declining trend in pain score from day 1 to the end of 1 week (Table 3-5) with 90 percent patients attaining a score of 2 (mild pain) (p<0.000 HS) and in the coblation group (2) the pain score persistently remained high. These observations were in a total contrast to a study conducted by Chris Mularczyk et al who found a better pain control in patients of coblation adenoidectomy as compared to the microdebrider group [9]. Similar results were observed in another study where coblation showed superior results than microdebrider in terms of postoperative pain score which could be attributed again to the application of electrocautery in microdebrider group for hemostatsis.8The prolonged pain duration noted in the present study in coblation could be due to the thermal injury occurring with the coblation wand used for the hemostasis, leading to fibrosis and contraction of the underlying tissue [10] In microdebrider group simple packing technique for haemostasis avoids the tissue thermal injury hence leading to less postoperative pain and early tissue healing.
| Group | Total | ||||
| 1(M) | Total | 2(C) | |||
| WONG BAKER 1wk | 2 | Count | 45 | 7 | |
| WONG BAKER 1wk | 2 | % within Group | 90.00% | 14.00% | |
| WONG BAKER 1wk | 4 | Count | 5 | 4 | |
| WONG BAKER 1wk | % within Group | 10.00% | 8.00% | ||
| WONG BAKER 1wk | 6 | Count | 0 | 39 | |
| % within Group | 0.00% | 78.00% | |||
| Total | Count | 50 | 50 | 100 | |
| % within Group | 100.00% | 100.00% | 100.00% |
| Chi-Square Tests | |||
|---|---|---|---|
| Value | df | Asymp. Sig. (2-sided) | |
| Pearson Chi-Square | 68.269a | 3 | 0 |
| Likelihood Ratio | 86.957 | 3 | 0 |
| Linear-by-Linear Association | 66.545 | 1 | 0 |
| N of Valid Cases | 100 | ||
| a. 4 cells (50.0%) have expected count less than 5. The minimum expected count is 1.50. | |||
Table 8: Postoperative Distribution of Patients According to their Pain Score in 1 Week Period in two Groups.
The basic aim of this study was to compare and determine an effective approach for adenoidectomy. The microdebrider and coblation both have been recently explored in performing adenoidectomy and limited data is present in literature comparing the two interventional modalities. On comparing the procedures for cost effectiveness the coblation technique was more expensive as the wand cost was higher as compared to the microdebrider and the wand also requires an early replacement as compared to microdebrider wand.
The microdebrider in terms of postoperative patient outcome had better results as children were able to resume normal activity early and were discharged early due to reduced pain scores, they had good oral intake and less systemic antibiotic requirement in comparison to coblation. In terms of recurrence both procedures left no residual tissue, the coblation had the advantage of a better hemostasis as the wand itself coagulated the tissues which was not possible with the microdebrider. The timing and blood loss in both the procedures was also comparable with no major differences seen. The limitation of our study was the number of patients as a larger group needs to be studied to elucidate and confirm the findings of the present study.
References
-
Kay DJ, Mehta V, Goldsmith AJ (2003) Perioperative adenotonsillectomy management in children: current practices. Laryngoscope 113(4): 592-597.
-
Palmer JM (2006) Bipolar radiofrequency for adenoidectomy. Otolaryngology Head Neck Surg 135(2): 323-324.
-
Walner DL, Parker NP, Miller RP (2007) Past and present instrument use in pediatric adenotonsillectomy. Otolaryngology Head Neck Surg 137(1): 49-53.
-
Rodriguez K, Murray N, Guarisco JL (2002) Power- assisted partial adenoidectomy. Laryngoscope 112 (8 pt 2 S100): 26-28.
-
Belloso A, Chidambaram A, Morar P, Timms MS (2003) Coblation tonsillectomy versus dissection tonsillectomy: postoperative haemorrhage. Laryngoscope 113(11): 2010-2013.
-
Temple RH, Timms MS (2001) Paediatric coblation tonsillectomy. Int J Pediatr Otorhinolaryngol 61 (3): 195- 198.
-
El Rahman AAAA, EI Shehaly ABEA, Dawood YM, El Sharkawy MA, Shalaby IT (2018) Comparative study between radiofrequency coblation and traditional adenoidectomy. Al-Azhar Assiut Medical Journal 16(2): 211-218.
-
Singh J, Bhardwaj B (2020) The Comparison between Microdebrider Assisted Adenoidectomy and Coblation Adenoidectomy: Analyzing the Intraoperative Parameters and Post-operative Recovery. Indian J Otolaryngology Head Neck Surg 72(1): 59-65.
-
Mularczyk C, Walner DL, Hamming KK (2018) Coblation versus microdebrider in pediatric adenoidectomy. International Journal of Pediatric Otorhinolaryngology 104: 29-31
-
Swibel-Rosenthal LH, Benninger MS, Stone CH, Zacharek MA (2010) Wound healing in the paranasal sinuses after Coblation, Part II: evaluation for endoscopic sinus surgery using a sheep model. Am J Rhinol Allergy 24(6): 464-466.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?