Rosai-Dorfman Disease with Neck Swelling: Case Report of a Child
Rosai-Dorfman disease (RDD) is a rare disease, particularly in children characterized by histiocyte proliferation within the sinusoids of lymph nodes and in extranodal tissue that progresses with extensive lymphadenopathy. Massive cervical lymphadenopathy as the initial manifestation tends to raise the initial suspicion of lymphoma. We report a 12-yearold boy presented with right-sided extensive neck swelling, Initial lymph node biopsy, and S 100, CD68 positive in immunohistochemistry confirming the diagnosis of Rosai-Dorfman disease. Although spontaneous resolution occurs, in our case, even after chemotherapy the child presented with recurrent neck swelling, and needed neck dissection.
Abbreviation
RDD: Rosai-Dorfman Disease
Introduction
Rosai-Dorfman disease (RDD) was described by Rosai and Dorfman in 1969, as a rare benign histiocytic disorder [1]. Classically, it presents as painless cervical lymphadenopathy but is increasingly showing extranodal involvement [1]. Recent studies have pointed out the diverse clinical presentations and their evolving understanding. It affects every age group, with mostly children and young adults being primarily affected, though the exact pathogenesis remains unknown, hence the various theories of infectious and genetic predisposition [2]. The most characteristic histological feature here is the presence of classical emperipolesis, wherein intact lymphocytes are phagocytosed by the histiocytes [3, 4]. Recent genetic findings indicate that MAP2K1 pathway mutations may contribute to certain cases, enabling targeted therapies [2]. Histiocytosis, sinus, and non-Langerhans-cell histiocytosis are key features distinguishing this disease. This study reviews the clinical, histological, and radiological features of RDD while addressing differential diagnoses and therapeutic progress. It also presents the statistical analysis of prevalence and outcomes, hence offering insights into the prognostic trajectory of the disease. The involvement of lymph nodes is a critical hallmark, particularly in pediatric cases, which makes understanding RDD in children essential.
Case Report

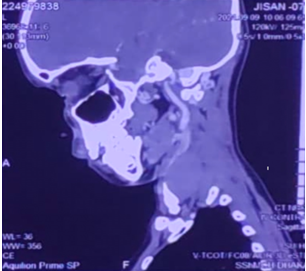
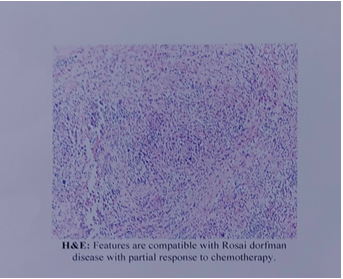
A seven-year-old boy Figure 1 presented with a 4-month history of progressive right cervical lymphadenomegaly without signs of inflammation, fever, weight loss, or night sweats. The lab tests revealed Hb 11.7g/dl, WBC 3.83k/Ul, ESR 29 mm/h. a high blood sedimentation rate (BSR: 103 mm/h), An Ultrasound scan of the neck showed multiple right-sided cervical nodes at levels I II, III, and IV, the largest one measuring about 4.15X2.15 cm. The CT scan of the neck showed a similar picture (Figure 2). On physical examination, the child was found to be in good overall condition but presented with a cervical mass of elastic consistency, without signs of adherence or inflammation. No pathologies were observed in the lungs, heart, abdomen, or extremities. The child was submitted to cervical lymph node biopsy, the histopathological analysis of which revealed a lymph node measuring 4.5X3 cm. Embedded 4 blocks. Microscopic pictures showed multiple matted lymph nodes, these revealed diffuse proliferation of histocytes with enlarged round nucleoli and abundant eosinophilic cytoplasm (Figure 3). The immunohistochemical examination was positive for PS100, and CD68, and negative for CD1alfa, thus compatible with Rosai-Dorfman disease. The child was referred to oncology for medical treatment with chemotherapy, after having 27 cycles of vinblastine, the child presented to our hospital with recurrent right-sided cervical lymph nodes. He underwent selective neck dissection. At present, he has been sent for medical oncology support.
Discussion
RDD is a complex condition that necessitates comprehensive evaluation and treatment. Over 40% of patients appear as asymptomatic, bulky cervical lymphadenopathy [5, 6]. Recent literature suggests a near 43% prevalence of extranodal involvement, complicating diagnosis and therapy [7, 8]. Common extranodal sites include the skin, orbit, and central nervous system, though the involvement of the respiratory or gastrointestinal tracts is not unknown [9]. Indeed, some of these extranodal manifestations may be similar to other diseases, cancers, autoimmune diseases, and infective conditions that mostly present delayed diagnosis of the disease. The histiocytosis associated with RDD, especially non-Langerhans-cell histiocytosis, provides a key diagnostic marker.
Radiological findings in RDD are frequently nonspecific, posing challenges for definitive diagnosis. CT and MRI commonly show well-defined, non-enhancing soft tissue masses or lymphadenopathy, which may appear similar in neoplastic conditions or inflammatory disorders. Research shows that several cases revealed soft tissue mass with the need for histopathology confirmation [10, 11]. Histologically, the disease features large histocytes with emperipolesis and immune-histochemical markers like S-100 positivity, with negativity to CD1a [2, 8]. These constitute important features in the differentiation of RDD from some disorders like Langerhans cell histiocytosis. The involvement of lymph nodes remains a prominent feature in the presentation of RDD, emphasizing the need for detailed histological evaluation.
The etiology of RDD remains speculative, with infectious agents like Epstein-Barr virus and Klebsiella pneumoniae implicated but not definitively proven [6, 4]. Some MAPK/ERK pathway mutations in RDD patients show clonal histiocytic proliferation, relating it to neoplastic illnesses rather than reactive circumstances [12, 13]. The concept of Rosai- Dorfman disease pathogenesis has increased, evolved, and reshaped the understanding of its underlying pathogenesis. This progress enables the possibility of targeted therapies, with MEK inhibitors among others indicated for refractory cases [14]. Such treatments make promising outcomes, given that they target the molecular pathology of the disease. Consequently, they represent an overwhelming shift in therapeutic approaches to RDD. Such developments usher in a new era in the effective management of this rare histiocytic disorder. The role of sinus histiocytosis is highlighted in recent studies as a critical aspect of RDD’s pathology.
RDD could also be caused by immune dysregulation. Sickness progression in affected individuals might be attributed to cytokine increases, including IL-6 and TNF-α, in affected individuals. The association of RDD further with autoimmune diseases, notably systemic lupus erythematosus, points to the immunological origin of the disorder [15, 16, 17]. In light of these findings, immunomodulatory drugs targeting cytokine pathways that act in combination with current treatments are under investigation. Insight into the immunological system of RDD will provide new therapeutic modalities and better management. Understanding the prevalence of histiocytosis and its implications for lymph node pathology in children highlights the complexity of RDD.
Treatment strategies for RDD vary according to disease severity and site involvement. Many cases are asymptomatic and self-limiting; therefore, the illness can resolve itself [18]. Systemic or symptomatic illness requires corticosteroids, immunosuppressants, and chemotherapy [19, 20]. New MEK inhibitor trials have shown potential, especially in refractory cases [21]. Surgical treatment is effective only in localized disease, and the inability to address systemic manifestations is a limitation [2]. Despite these advances, relapses occur in some cases, thus necessitating protracted follow-up. The impact of lymph nodes and their histiocytic involvement is a major focus in surgical and systemic treatment planning.
The prognosis of RDD is generally favorable, with survival rates exceeding 90% across most cohorts [15, 22, 23]. However, systemic involvement the more so in vital organs like the lungs far worsens the prognosis [11]. Ongoing development of imaging, histopathology, and molecular studies will improve diagnosis and treatment of this disease. The involvement of lymph nodes and extranodal manifestations underscores the need for continued exploration of sinus histiocytosis and non-Langerhans-cell histiocytosis in prognosis and treatment [24].
Analyzing Rosai-Dorfman’s disease epidemiology and clinical features provides insights into its natural history and therapeutic outcomes [8, 25]. In a retrospective review, 150 cases showed slight male predominance, as the male- to-female ratio was 1:5. This result is consistent with other studies also [2]. The median age at the onset was noted to be 50 years, though all age groups, from infancy to well- advanced adulthood, could be affected [2].
In other cases, cervical lymphadenopathy remains the most common symptom, occurring in 83% of cases, and thus presents as a hallmark feature. Of the 64 patients, 8% had classical (nodal only) and 92% had the extra-nodal disease (67% extra-nodal only). About 43% of the patients experience Extranodal involvement, mainly in the skin 52%, followed by lymph nodes (33%) [8, 26]. Systemic symptoms include fever, night sweats, and weight loss identified in about 20% of the cases; most of them can present similarly to lymphoma or tuberculosis among other conditions.
Radiological findings further highlight the disease’s complexity. Among the imaged patients, 68% had soft tissue masses, and 32% of the patients had isolated lymphadenopathy. These imaging findings, however, are nonspecific and have to be confirmed histologically to enable an appropriate diagnosis. All cases examined in histopathology showed the characteristic features of RDD, such as emperipolesis and S-100 positivity [8, 27, 28]. Immunohistochemistry was especially valuable for diagnosing RDD among other histiocytic disorders, thus signifying the importance of tissue biopsy for diagnosis [1]. The frequent involvement of lymph nodes and sinus histiocytosis is evident from the histological and immunohistochemical findings.
Treatment outcomes varied significantly depending on disease presentation and severity. About 32% were cases of spontaneous remission without intervention, while in a percentage of patients with RDD, the disease tends to be self-limiting [8, 29, 30]. Corticosteroid therapy was necessary in about 21%, primarily in patients with systemic or symptomatic disease, and surgical excision in 12%, mostly in those with localized extranodal disease causing functional impairment [2]. Targeted therapies include the use of MEK inhibitors in 5% of refractory cases, which induced partial or complete remission in these patients [30]. Despite such therapeutic advances, 14% of cases relapsed, indicating that for a subset of patients, this is a chronic active disease with the tendency to relapse. Histiocytosis of the sinus and its role in prognosis, especially in pediatric cases, are areas of active investigation.
Survival analysis revealed a favorable five-year survival rate of 94%, consistent with the generally benign course of RDD [31, 32]. However, this number considerably went down to an extremely low level in the cases of systemic organ involvement that implicate vital organs like the lungs or kidneys. The poor prognostic factors include advanced age, systemic symptoms, and more extensive organ involvement; early intervention and personalized treatment are justified [8, 33, 34]. These results again underline timely diagnosis and long-term management for better outcomes for the patients. The involvement of lymph nodes in children remains a consistent feature, guiding therapeutic decisions. Larger cohort studies with extended follow-up are essential to validate findings and improve prognostic models. Research should be directed toward the development of novel therapies for refractory or relapsing cases to optimize outcomes. Such efforts will also deepen the understanding of the natural history and progression of RDD.
Conclusion
Rosai-Dorfman disease, though rare, is a unique histiocytic disorder with diverse clinical and pathological manifestations. Advances in imaging studies, histopathology, and molecular genetics have enormously improved both diagnostic skills and treatment. Also, although self-limiting with systemic involvement, it can cause great morbidity requiring timely interventions pertinent to all patients for a universally optimal outcome. Statistical analyses reveal a slight male predominance, a broad age range of onset, and survival rates exceeding 90%. The systemic involvement of vital organs is a big challenge and carries a poor prognosis; it always requires continued follow-up and management. Newer therapies, especially MEK inhibitors, do hold promise in cases of refractory or relapse. This provides optimism for better outcomes and improved patient care. The variable clinical course of the disease necessitates a major multidisciplinary diagnosis and management. Further research is required since there is a need not only to understand its etiology properly but also to develop targeted treatment modalities. Patients in this difficult condition will receive state-of-the-art outcomes as model prognostics improve.
References
-
Xiao C, Jing-Liang C, An-Kang G (2018) A study on clinical characteristics and magnetic resonance imaging manifestations on systemic Rosai-Dorfman disease. Chinese Medical Journal 131(04): 440-447.
-
Gulwani H, Bhalla S, Srivastava A (2008) Isolated lacrimal gland involvement in Rosai-Dorfman-Destombes disease. Indian Journal of Ophthalmology 56(6): 507-509.
-
Pradhananga, Bhakta R, Dangol K, Shrestha A, Kanta Baskota D (2014) Sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease): A case report and literature review. International archives of otorhinolaryngology 18: 406-408.
-
Xianfeng R, Kang Z, Chen J, Cai C, Wang B, Zhang Q (2023) Cervical spine Rosai–Dorfman disease: A case report and literature review. Medicine 102(43): e35654.
-
Abla O, Jacobsen E, Picarsic J, Krenova Z, Jaffe R, et al. (2018) Consensus recommendations for the diagnosis and clinical management of Rosai-Dorfman-Destombes disease. Blood 131(26): 2877-2890.
-
AlKuwaity, Waleed K, Hamoud Alosaimi M, Tariq Alsahlawi K, Abdullatif Alomair M et al. (2019) Unusual presentation of Rosai-Dorfman disease: Report of a rare case. The American Journal of Case Reports 20: 91.
-
Gaurav A, ChandrashekharR, Parmar H (2016) Rare case of Rosai Dorfman disease involving paranasal sinuses in pediatric patient: A case report. Egyptian Journal of Ear, Nose, Throat and Allied Sciences 17(1): 43-46.
-
Pan-pan H, Wei F, Xiao-guang L, Zhong-jun L (2021) Diagnosis and treatment of Rosai-Dorfman disease of the spine: A systematic literature review. Systematic Reviews 10: 1-10.
-
Daniele Cristine Gomes P, de Aguiar Vidigal T, de Castro B, Hollanda dos Santos B, José Alves de Sousa N (2008) Rosai-Dorfman disease in the differential diagnosis of cervical lymphadenopathy. Revista Brasileira de Otorrinolaringologia 74: 632-635.
-
Brenn T, Calonje E, Granter SR, Leonard N, Grayson W, et al. (2002) Cutaneous rosai-dorfman disease is a distinct clinical entity, The American Journal of Dermatopathology 24(5): 385-391.
-
Cooper SL, Jenrette JM (2012) Rosai-Dorfman disease: management of CNS and systemic involvement, Clinical Advances in Hematology and Oncology 10(3): 199-202.
-
Cracolici V, Gurbuxani S, Ginat DT (2019) Head and neck sinus histiocytosis with massive lymphadenopathy radiology–pathology correlation, Head and Neck Pathol 13(4): 656-660.
-
Saubhagya D, Katwal S, Ghimire A, Bhusal A, Nath Yogi T (2024) Uncommon presentation of Rosai-Dorfman disease: Nasal and nasopharyngeal involvement: A case report and discussion. Radiology Case Reports. 19(3): 956-960.
-
Duval M, Nguyen VH, Daniel SJ (2009) Rosai-Dorfman disease: an uncommon cause of massive cervical adenopathy in a two-year-old female, Otolaryngology. Head and Neck Surgery 140(2): 274-275.
-
Emmanuella A, Apeadu Danso K, Sefakor Akuaku R, Ulzen-Appiah K (2022) A Report of Rosai–Dorfman Disease in an Adolescent. Case Reports in Pediatrics. 1: 9571400.
-
Dio S, Ilaria Mariotti F, Coccolini E, Bruzzi P, Predieri B, et al. (2016) Unusual presentation of Rosai-Dorfman disease in a 14-month-old Italian child: A case report and review of the literature. BMC paediatrics 16: 1-7.
-
Gaurav G, Ravindran A, Young JR, Shah MV, Bennani NN, et al. (2019) Clinicopathological features, treatment approaches, and outcomes in Rosai-Dorfman disease. Haematologica 105(2): 348.
-
Ling L, Huang Y, Zeng C (2020) Infantile Rosai-Dorfman disease: An unusual case of neck swelling and a literature review. International Journal of Clinical and Experimental Pathology 13(12): 3187.
-
Aastha G, Arora P, Batrani M, Kumar Sharma P (2018) Multifocal cutaneous Rosai-Dorfman disease masquerading as lupus vulgaris in a child. Anais brasileiros de dermatologia 93(5): 766-768.
-
Felipe Barbosa L, Samuel de Valões Barcelos P, Paula Nunes Constânci A, Dantas Nogueira C, Aldo Melo-Filho A (2011) Rosai-Dorfman disease with spontaneous resolution: Case report of a child. Revista brasileira de hematologia e hemoterapia 33: 312-314.
-
Rosai J, Dorfman RF (1969) Sinus histiocytosis with massive lymphadenopathy: a newly recognized benign clinicopathological entity, Archives of Pathology 87: 63- 70.
-
Lu D, Estalilla OC, Manning JT, Medeiros LJ (2000) Sinus histiocytosis with massive lymphadenopathy and malignant lymphoma involving the same lymph node: A report of four cases and review of the literature, Modern Pathology 13(4): 414–419.
-
Maia RC, de Meis E, Romano S, Dobbin JA, Klumb CE (2015) Rosai-Dorfman disease: A report of eight cases in a tertiary care center and a review of the literature, Brazilian Journal of Medical and Biological Research 48(1): 06-12.
-
Tanvi V, Mahajan A, Rane S (2020) Multimodality imaging manifestations of Rosai-Dorfman disease. Acta Radiologica Open 9(8): 2058460120946719.
-
Xingshu Z, Yin W, Guo W, He Y, Jiang Z, et al. (2022) Rosai–Dorfman disease of the central nervous system: A clinical, radiological, and prognostic study of 12 cases. Frontiers in Oncology 12: 1013419.
-
Winnie A, Jonathan H, Gracia Knuttinen M, Horowitz JM, David O, et al. (2017) Rosai-Dorfman disease: Manifestations outside of the head and neck. American Journal of Roentgenology 208(4): 721-732.
-
Francis Ikechukwu U, Obiora Ezomike U, Uchenna Ezenwosu O, Bismarck Eke C, Onyekachi Nwokoro C (2018) Rosai-Dorfman Disease: A clinico-pathological presentation of three cases and review of literature. Blood Pressure (BP) 90: 60.
-
Aishwarya R, Rech KL (2023) How I Diagnose Rosai- Dorfman Disease. American Journal of Clinical Pathology 160(1): 1-10.
-
Shi Y, Griffin AC, Zhang PJ, Palmer JN, Gupta P (2011) Sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman Disease): A case report and review of 49 cases with fine needle aspiration cytology, CytoJournal 8.
-
Kirti S, Doraisamy D, Niazi M, Kronfeld G, Hagmann S, et al. (2014) Sinus histiocytosis and massive lymphadenopathy (Rosai-Dorfman disease) mimicking cervical lymphadenitis. The Journal of Pediatrics 164(4): 943-943.
-
Lungren MP, Petrella JR, Cummings TJ, Grant GA (2009) Isolated intracranial Rosai-Dorfman disease in a child. American Journal of Neuroradiology 30(10): E148-E149.
-
Destombes P (1965) Adénites avec surcharge lipidique, de l’enfant ou de l’adulte jeune, observées aux Antilles et au Mali (Quatre observations), Bulletin de la Société de Pathologie Exotique 58: 1169-1175.
-
Osama A, Schellingerhout D, Fuller GN, Ketonen LM (2011) Rosai-Dorfman disease in neuroradiology: imaging findings in a series of 10 patients. American Journal of Roentgenology 196(2): W187-W193.
-
Alessandro P, Anghel G, Falcucci P, Matera R, Pescarmona E, et al. (2002) Treatment of sinus histiocytosis with massive lymphadenopathy (Rosai‐Dorfman disease): Report of a case and literature review. American journal of hematology 69(1): 67-71.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?