A Comparative Analysis of Bacterial Diversity in Individuals Exhibiting Oral Cavity Disorders versus those in a State of Oral Health
Oral cavity is considered as main entrance of the body and our mouth encounters a large number of microorganisms from the outer environment, some of which have the potential to cause serious illnesses. Current study was designed to evaluate different ecological and behavioral factors which can positively or negatively affect normal flora of oral cavity. Behavioral information was gathered through personal interviews from 90 study subjects, out of which 45 were included in control group without any current oral disorders and other 45 were included in experimental group with current oral diseases. High rate of sugar consumption, low brushing frequency, over-use of medications, acidic food consumption, high rate of smoking, aggressive mode of brushing and lack of awareness about dental health were some of the factors observed in a higher ratio in experimental group. These behaviours can aggravate oral problems causing imbalances in normal flora of oral cavity. It was also noted that frequency of systemic diseases was higher in experimental group, and it was due to the fact that unbalanced bacterial oral flora can gain entry into blood through bacteraemia and travel to different organs, thus, intensifying systemic issues. A comparative analysis was also made between bacterial flora of healthy controls and oral patients. A total of 34 oral samples, 17 from control group and 17 from experimental group, were collected and analyzed morphologically and biochemically. A total of 12 distinct bacterial species were isolated from these collected samples. Some of the species were conserved in both groups but were present in varying proportions. But Neisseria spp. was isolated only from healthy controls while Escherichia coli, Pseudomonas aeruginosa, Corynebacterium and Actinobacteria were isolated from samples oral patients. The most abundant species in healthy controls were Staphylococcus aureus, Lactobacilli and Staphylococcus epidermidis while in oral patients were Lactococci, Actinobacteria, Corynebacterium and Streptococcus viridans group. The involvement of oral bacterial flora in systemic diseases and role of behavioral elements in aggravating oral diseases was also responsible for oral cavity disorders. Different pathogenic bacteria can alter the natural bacterial ecology of oral cavity, aggravating oral diseases. This study may provide a baseline data to develop different strategies to control pathogenic oral flora.
Hashir Khan1*, Mahnoor Ijaz1#, Sania Khan2, Ammarah Rehmat3, Nabeel Hussain4, Hammad Sultan5 and Muhammad Iliyas6
#equally contributed towards this manuscript
Introduction
Bacteria as a Normal Flora of Human Body
Every human has a unique microbial flora connected with their skin and mucous membranes [1]. 10¹³ cells are present in human body, while human body harbors around 1014 bacteria [1]. Such large bacterial population form the normal microbial flora of human body [1]. The number of cells forming human body is less than the number of bacteria colonizing mucous membranes and skin [2]. The bacteria residing human body are forming complex ecosystems with enormous diversity [2]. This bacterial flora coevolves with their hosts [2]). Age, nutrition, stress, hormonal changes, drugs, and sexual behaviors are some host-related factors that affect the natural flora’s makeup [3].
The bacterial species dominating in different parts of human body vary according to niche like vagina, intestine, oral cavity, skin, stomach, urinary tract [4]. Normal flora of oral cavity varies according to sampling site and oral health of the person [5]. The oral cavity contains a mixture of microbes and the most predominating flora found by Gagliardi et al. was Streptococcus viridians [6]. Lactobacilli and Alpha hemolytic Streptococcus species have been found residing tonsils of young children [5]. A very few number of bacteria colonize stomach because of its acidic pH [7]. When 16S rRNA oligonucleotide probes were used to identify the typical flora of the human body, Bacteroidetes made up 20% of the fecal flora, Clostridium coccids and Eubacterium recitals made up 29%, Gram Positive bacteria made up 13%, and Bifidobacterium species made up 3% [8].
The body’s normal flora participates in a number of useful processes, such as vitamins production, immune system stimulation, stimulation of cell maturation, mucosal cell development, substrate digestion and also helps in colonization resistance of intestinal tract [1]. Many important vitamins such as vitamin B12, vitamin B5, B6 and vitamin K2 are produced by members of microbial flora [5]. Members of bacterial flora produce a number of compounds which aid in activating innate and adaptive immunity of human body [3].
A number of factors including age, dietary habits, geographical distribution, use of probiotics and prebiotics, environmental factors, stress, diseased conditions and antibiotics exposure can cause disruption of normal flora [4].
Normal Flora Of Oral Cavity
A range of microbial species can be found in the human mouth cavity as part of the normal flora. Numerous parts of oral cavity, such as the teeth, tongue, hard and soft palates, tonsils, mucosa, and gingiva, are home to a variety of bacteria [9]. In different areas of the oral cavity, the composition and abundance of microbial communities differ. As a result, the physiochemical properties of the oral cavity are heterogeneous, and a variety of parameters, such as pH, oxygen, temperature, redox potential, and others, can influence the microbial community composition and settling [10].
The oral cavity, also known as the mouth, is regarded as the body’s doorway, its health should be a priority for everyone [11]. One of the most intricate microbial communities in human body is oral microbiota, which is made up of about 700 different types of bacteria [1]. The most common inhabitants of the oral cavity are bacteria, with Firmicutes, Proteobacteria, Bacteroidetes, and Actinobacteria being the most common phyla. Fusobacteria and Spirochaetes are less common phyla, while the most common bacterial genera are Streptococcus, Hemophilus, Neisseria, Prevotella, and Villanella [12].
Bacterial Flora in Oral Diseases
Humans and their oral microbiota have a lifelong relationship that starts soon after birth. The relationships between the host and oral bacteria were previously thought of as a variety of single species interactions [13]. However, the interaction between the host and the greater microbial population determines whether the mouth is healthy or ill, and it is becoming more and more obvious that the oral bacterial community is a complex community [14].
The most prevalent chronic oral illnesses worldwide are dental caries and periodontal disease, also known as gingivitis and periodontitis. Although these illnesses have been present in humans since prehistoric times, their frequency has significantly grown in recent times [15]. The frequency of dental caries is currently 60–65 percent in India, whereas the prevalence of periodontal disease is 65–100 percent [16]. The calcified tissues of the teeth can dissolve and be destroyed in certain places as a result of the infectious microbial disease known as Dental Caries. It has been very challenging to establish a causal link between a single oral flora bacteria and caries up to this point. The majority of researchers think that the development of microbial plaque in the tooth occurs before the development of enamel caries [17].
Gingivitis can be brought on by a variety of compounds formed from microbial plaque that have accumulated at or close to gingival calculi. The two microbial species that are linked to gingival health are Streptococcus sanguis and Fusobacterium naviforme, whereas specific species of Streptoccous, Fusobacterium, Actinomyces, Veilonella, and Treponema, as well as possible Bacteroides, Capnocytophaga, and Eikenella, are linked to the etiology of gingivitis [18]. Anywhere in the mouth and oropharynx, including the lips, oral mucosa, gingivae or gums, tongue, soft and hard palate, and throat, might develop an oral sore [18]. The majority of mouth sores are uncomfortable, painful, and in certain circumstances can be seriously dangerous [3]. Canker and cold sores are the two most typical mouth sores. Canker sores are extremely common, yet there is conflicting data regarding their cause. Genetics could be involved, with an immunologic predisposition occurring in 33% to 42% of cases [4].
Role of Oral Flora in Systemic Diseases
Recent case-control studies and epidemiologic investigations have discovered a strong connection between poor dental health and cardiovascular problems, early mortality from any cause, premature births and low birth weight newborns [1]. After adjusting for known risk factors for coronary disease, dental disease was found to be a significant predictor of coronary events that resulted in mortality in a 7-year prospective analysis [12]. In another study, missing teeth replaced smoking as the risk factor for ischemic heart disease [17]. In comparison to the mother’s age, race, number of live births, usage of cigarettes or alcohol, periodontal disease was seven times more likely to be associated to a premature birth with a low birth weight baby [19].
Chronic Gram-negative infections called periodontal diseases are an antecedently unknown risk factor for arteriosclerosis and thrombotic events. The risk of myocardial infarction and cerebral infarction has been linked to the extremity of periodontitis in previous studies [20]. The release and systemic appearance of pro-inflammatory cytokines in periodontitis, which can cause effects linked to atherosclerosis and coronary heart disease, is a relationship between the two disorders [21].
Numerous epidemiological studies have affirmed a connection between poor dental health and unfavorable pregnancy outcomes. Two virulence mechanisms are put forth: inflammatory mediators produced in the mouth cavity that impacts the fetal-placenta unit and direct invasion of oral bacteria or their components into the fetal-placenta unit [22]. It is believed that maternal periodontal conditions contribute to an increase in preterm births with low birth weight in newborns [23]. Pro-inflammatory cytokines are produced in considerably higher amounts by inflamed periodontal tissues, and these cytokines may affect the host mother and fetus systemically [23]. The endotoxins produced by the bacteria that cause periodontal disorders can be hazardous to the developing embryo. Maternal vitamin D level is another potential link between periodontal disorders and unfavorable pregnancy outcomes. Low vitamin D levels have been found to be a factor in the emergence of periodontal diseases [23]. Oral bacteria can relocate in the gut and alter the microbiota and perhaps the defense system of the body [18].
The dysbiosis that Porphyromonas gingivalis causes in the sub-gingival microbial flora and immune system may also lead to dis-regulation in the gut. Diseases in other parts of the body may be caused by a dis-biotic gut microbiota [24]. The hypothesis that periodontal infection is a risk factor for having poor glycemic control in adults with type 2 diabetes was found to be supported by clinical and population-based affirmations in a study; however, investigations of this association had a limited representation of older people [1].
Recent investigations have suggested that many different microorganisms, including oral and non- oral Treponema species, herpes simplex type I viruses, and yeasts, are present in Alzheimer’s disease brains. Due to daily, temporary bacteremia, periodontitis has the ability to transmit live bacteria, virulence factors, and inflammatory mediators to the brain [24].
Aim and Objectives
The aim of this study is to conduct a comparative analysis of bacterial diversity in individuals exhibiting oral cavity disorders as opposed to those in a state of oral health. The primary focus is to investigate and understand the variations in the microbial composition within the oral microbiome of these two groups, shedding light on how bacterial diversity may be associated with oral health and disorders.
Materials and Methods
Study Design
Present study was conducted in the Department of Microbiology at the Kohsar University Murree, in Punjab, Pakistan, from March 2023 to September 2023. This study consisted of patients with oral cavity disorders and healthy participants. Total participants of this study were 34. Subjects were divided into two groups: Group I, The Control Group, included 17 people without oral diseases at that time, and Group II, The Experimental Group, included 17 people with oral diseases.
The criteria for inclusion in this study was healthy persons with no missing teeth, no present symptoms of periodontitis, gingivitis and no prosthetically restored teeth, while, the oral patients showing any symptom of gingivitis, periodontitis, dental caries (tooth decay), oral sores and oral thrush (candidiasis) were included in this study.
Clinical Data Collection
Before gathering samples for laboratory analysis, information about the study subjects’ clinical histories and daily activities was gathered in order to learn about their general health conditions and to determine which factors are more likely to cause oral health issues. To gather information regarding clinical history, a variety of questions about dental visits, any current or past oral disorders, any current or past systemic disorders, the mean number of decayed, missing, and filled teeth (DMFT), and daily routine behaviors that may contribute to the aggravation of oral health issues were included in the questionnaire.
Sample Collection and Processing
Total 34 samples were taken from different participants in both groups. Samples were collected using sterilized oral swabs. It is important to avoid any extrinsic components (after meal) while collecting samples. Samples were taken directly from five distinct locations of dental plaques, thrush sites, oral sores on buccal and tongue areas and dental plaques. Samples of oral patients were collected from Type D Hospital Murree, District Murree, Punjab, after granting permission from Managing Director of the Hospital. Samples of both groups were transported rapidly to Central Laboratory at the Department of Microbiology, Kohsar University Murree for further processing.
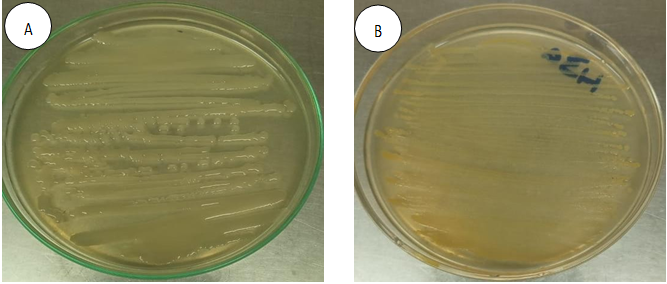
The collected samples were inoculated on general purpose medium for bacterial growth i.e., Nutrient Agar. After that, samples were maintained in an incubator for 24-48 hours at 37°C. To identify different bacterial species, pure cultures of bacterial colonies were prepared using different selective media, such as, MacConkey Agar, Mannitol Salt Agar, Blood Agar and De Man, Ragosa and Sharpe Agar (MRS). Gram staining was performed to observe bacterial morphology and to characterize gram positive and gram- negative bacteria. For further confirmation, biochemical tests (Catalase test, Coagulase test, Sugar Fermentation test, Simmons Citrate test and Methyl Red test) were performed.
Culture Medias Used
Different agar and broth culture media were used for growth, identification, and isolation of oral bacteria. Different general purpose and selective media used were Nutrient Agar, Mannitol Salt Agar, MacConkey Agar, Blood Agar and De Man, Ragosa and Sharpe Agar (MRS Agar). The uses and principles of these culture media are discussed below.
Nutrient Agar: A variety of non-fastidious microorganisms can be grown on nutrient agar, a general-purpose complex media. Nutrient agar is composed of a range of nutrients and proteins, thus, supports growth of various types of bacteria and yeasts. Various types of microorganisms ranging from fungi, like, yeasts and molds, to common bacteria, such as, Streptococci, Staphylococci, Enterobacteriaceae, etc., can grow on nutrient agar.
The nutrient agar of Oxoid UK company was used in this study. The 28g of nutrient agar were mixed in 1 liter of distilled water. The medium was autoclaved at 121°C for 15 minutes after being boiled. After sterilization, temperature was allowed to decrease up to 50°C. After cooling, media was poured in sterilized Petri dishes. Once the media in dishes was solidified, inoculation of samples was performed in biosafety cabinet. Mannitol Salt Agar: The growth, isolation, identification, and characterization of Staphylococci are all accomplished using Mannitol Salt Agar, commonly known as Chapman Agar. This growth medium will select those microorganisms to grow that can live in high salt concentration. This medium functions as a selective medium as most Gram negative and Gram-positive bacteria cannot thrive in an environment with a high Sodium Chloride content. Medium also acts as a differential medium based on ability to ferment mannitol. If bacteria are able to ferment mannitol, pH drops to < 6.9, indicating acidification, and color of medium also changes from red/pink to yellow. Mannitol non- fermenters grow on medium without causing any color change.
The MSA media of Oxoid UK company was used in this study. 111g of MSAs medium were mixed with 1-liter distilled water. Boiling was done to completely mix ingredients in the medium. Medium was then autoclaved at 121°C for 15 minutes to sterilize it. The medium was sterilized, allowed to cool to 50°C and then, put in sterilized Petri dishes. After solidification, bacterial cultures were inoculated on dishes and Petri dishes were maintained in an incubator at 37°C for 24-48 hours.
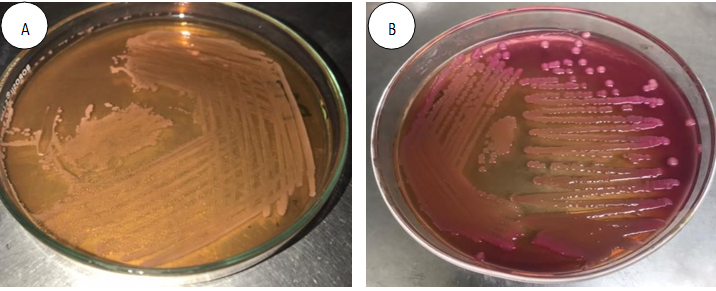
Macconkey Agar: Alfred Theodore MacConkey created the first solid differential medium in 20th century. A variety of non-fastidious Gram-negative bacteria are grown, isolated, identified and differentiated using the selective and differential media known as MacConkey Agar. It acts as a selective medium by allowing only Gram-negative enteric bacteria to grow. The majority of Gram-positive bacterial species are inhibited from growing because medium contains crystal violet and bile salts. By causing a color shift, the medium also distinguished lactose fermenters from lactose non- fermenters. Colonies made by lactose-fermenting bacteria are red or pink, while those made by lactose non- fermenting bacteria are colorless.
49.53 grams of media of Oxoid company UK was dissolved in 1 liter distilled water. Boiling was done to ensure complete mixing and media was autoclaved for 15 minutes at 121°C. When temperature of medium reaches to 50°C, media was transferred to sterilized Petri dishes. Media was left for a little time to completely be solidified in dishes. Inoculation of bacterial cultures was performed and left to incubate at 37°C for 24-48 hours.
Blood Agar: Blood agar is enrichment media which is used to grow, isolate and identify those bacteria that don’t grow easily (fastidious), as they require special, enriched environment to grow. It allows growth of a number of pathogens such as Streptococci, Staphylococci, Neisseria sp, Haemophilus influenzae, etc. It also acts as a differential medium due to three types of hemolysis (Alpha, Beta and Gamma) produced by bacteria.
Ingredients in Blood Agar Base were dissolved in 1000ml distilled water. Media was boiled to ensure complete mixing and sterilization was done by autoclaving media for 15 minutes at 121°C. When temperature of media was lowered to 45-50°C, 5% vol/vol sterile defibrinated blood was added and mixed well avoiding any air bubbles. Media was transferred immediately to autoclaved Petri dishes and after the media was solidified, inoculation step was performed. Petri dishes were placed in incubator to provide standard conditions for bacterial growth.
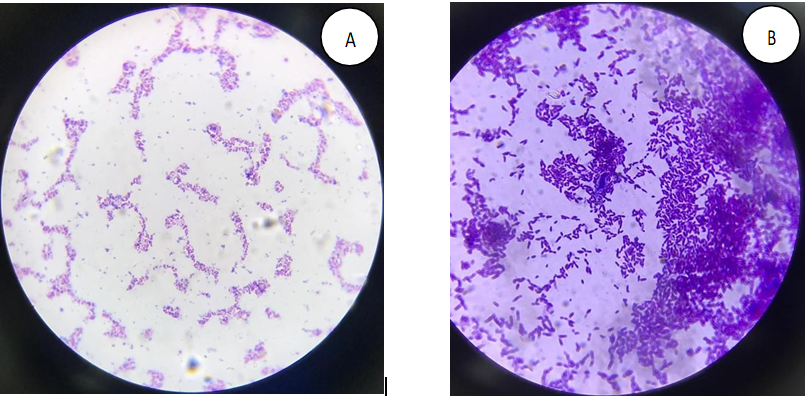
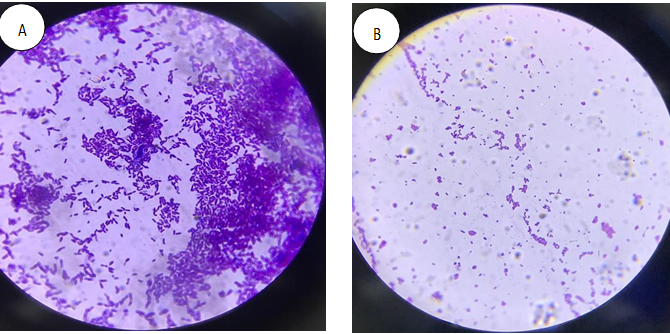
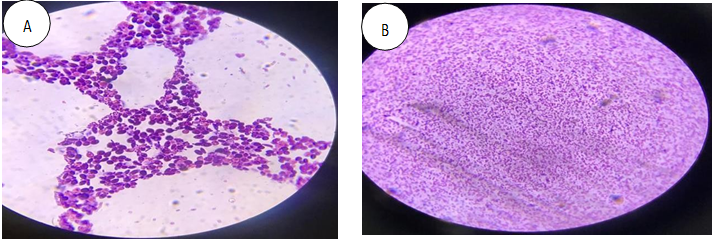
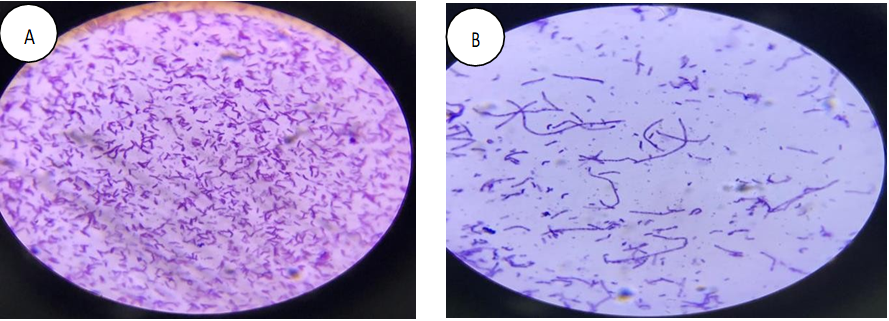
De Man, Ragosa and Sharpe Agar (MRS): De Man, Ragosa and Sharpe Agar, abbreviated as MRS, is a selective media which supports the growth of Lactobacilli found in clinical, food and dairy samples. The medium was developed in 1960 and was named after its inventors. It has a clear brown color and contains sodium acetate which inhibits growth of many competing bacteria. Some other Lactobacillales like Leuconostoc and Pediococcus may also gain opportunity to grow. 233.35g of media of Oxoid company UK was dissolved in 1000ml distilled water. Media was boiled to completely dissolve ingredients. Media was autoclaved at 121°C for 15 minutes to sterilize. Temperature was decreased to 50°C and transferred to sterilized Petri dishes. After the media was solidified in petri dishes, samples were inoculated with the help of wire loop. After inoculation, Petri dishes were placed in incubator at 37°C for 24-48 hours. Gram Staining Hans Christian Gram first introduced the process of differential staining known as Gram staining. Gram staining procedure is used to identify bacteria on the basis of Gram Positive or Gram-negative cell walls. Thick Peptidoglycan layer is present in cell wall of some bacteria due to which these bacteria are stained purple or blue. These bacteria are called Gram Positive bacteria. Gram Negative bacteria lose crystal-violet stain when decolorizer is added. In Gram Negative bacteria, peptidoglycan in cell wall is thinner and when decolorizer is added, crystal violet-iodine complexes dissolve and removed from cell walls on rinsing. Thus, Gram negative bacteria appear pink in color when secondary stain safranin is added (Figure 1).
- A clean and sterile glass slide was taken and a drop of water was added in the center.
- Using a wire loop, smear was prepared by taking bacterial colonies from fresh culture.
- The smear was heat fixed using a spirit lamp.
- Primary stain, Crystal violet dye was added and was left for 50-60 seconds.
- Slide was washed with water and mordant iodine was added for 30 seconds.
- After rinsing, decolorizer (alcohol) was added for 15-30 seconds.
- Secondary stain, Safranin was added after rinsing slide with water.
- After 60 seconds, slide was air dried after rinsing.
- The prepared gram stain slides were observed under light microscope using 100X magnification.
Catalase Test: The catalase test was performed to detect catalase enzyme produced by different bacterial species. The enzyme catalase has the ability to degrade hydrogen peroxide yielding water and oxygen.
2H₂O₂→2H₂O+O₂ To perform catalase test, bacterial colonies form 24- hour fresh were taken on a clean glass slide and a drop of hydrogen peroxide (Catalase Reagent) was added to the slide to make a smear. Bubble formation indicated positive test while no bubbles indicated negative test (Figure 2).

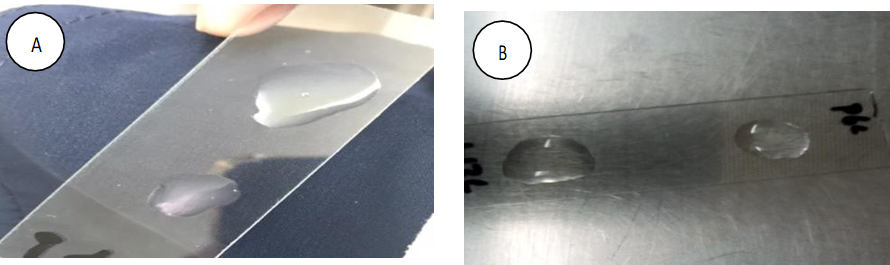
Coagulase Test: Coagulase test was performed to detect the production of coagulase enzyme by bacterial isolates. The coagulase enzyme clots plasma by converting fibrinogen to fibrin. This test is specifically used to differentiate Staphylococcus aureus from other Staphylococcal species, as Staphylococcus aureus is coagulase positive. A drop of saline was placed on a sterile glass slide. With the help of wire loop, bacterial colonies were added to saline in order to make a thick suspension. A drop of human plasma was added to the suspension. Clumping of colonies indicated positive test while negative test was interpreted by no clumping (Figure 3).
Sugar Fermentation Test: Bacteria can be identified based on property to produce organic compounds using different carbohydrates as substrates. Sugar fermentation test can be used to identify different bacterial species based on the ability to ferment carbohydrates. Different fermentation medias which provide carbohydrates can be used for this purpose. The organism ferments carbohydrates which result in lowering of pH of the medium, detected by a pH indicator dye.
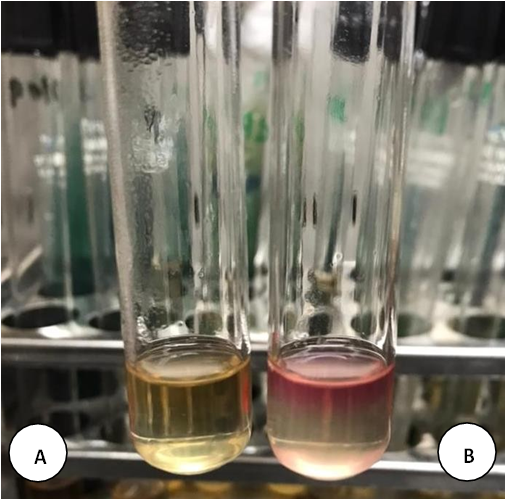
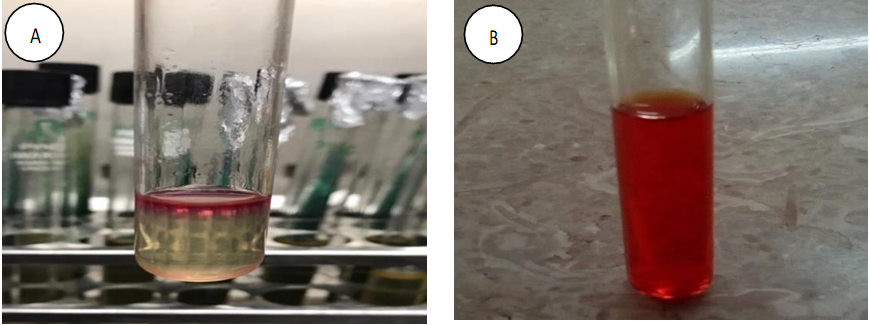
Phenol Red Glucose Broth was used as fermentation medium which contained peptone, phenol red (pH indicator dye), Durham tube and glucose carbohydrate. The bacterial colonies to be tested were inoculated in each test tube containing Broth. The tubes were allowed to incubate at 35- 37ºC for 18-24 hours. Yellow color of Broth indicated positive tests showing ability of bacteria to ferment carbohydrates. No color change indicated negative test showing inability of bacterial species to ferment carbohydrates (Figure 4).
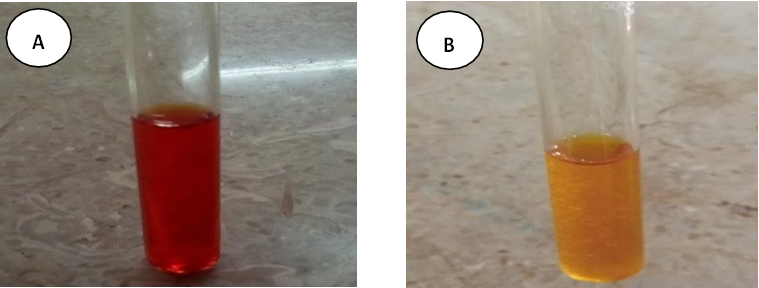
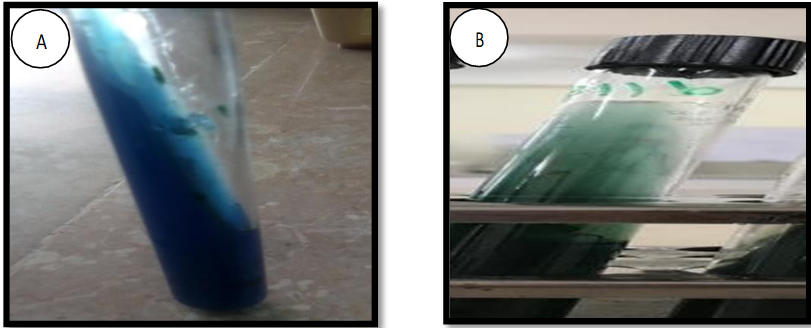
Figure 4: Sugar Fermentation Test- (A) Negative Control and (B) Positive Control. Simon Citrate Test: Simon citrate test is used to identify Enterobacteriaceae based on property to use citrate as a carbon source. Simon citrate agar is the differential medium used for this purpose. Bacteria capable of utilizing citrate will grow unrestricted on citrate media. Ammonium salts in medium are broken down into ammonia, it causes the pH to increase and the color of medium changes from green to blue due to color shifting of bromothymol blue. Inoculation of bacterial cultures was performed by stabbing in all test tubes after preparing agar slants in tubes. Tubes were allowed to incubate at 35-37ºC for 5-7 days. Positive result was obtained when color shift from green to blue occurs, but no color shift indicated negative result (Figure 5).
Methyl Red Test: Some bacteria have the ability to ferment glucose producing stable acids and this property can be detected by methyl red test. The bacteria initially convert glucose into pyruvate, which is further metabolized into stable acids such as, formic acid, lactic acid or acetic acid. Acid production decreases the pH to 4.5 or below, which can be detected by a color shift from yellow to red. MRVP Broth medium was prepared and inoculation of 18-24 hours pure cultures was performed in all the broth tubes. Tubes were placed in incubator for 24 hours at 35-37ºC. After transferring 1ml broth to a fresh tube, 2-3 drops of methyl red were added. Positive result was observed through color shift from yellow to green while no color shifting indicated negative result (Figure 6).
Hemolysis Test: Hemolysis test can be used to identify bacterial species based on type of hemolysis. Blood agar cultures are used for this purpose. Blood agar contains general nutrients and 5% defibrinated blood and is used for the growth of fastidious microorganisms and to differentiate microorganisms on the basis of hemolytic capabilities. Bacteria produce enzymes called hemolysins which have the ability to break down red blood cells. There are three types of hemolysins: Beta hemolysin, Alpha hemolysin, and Gamma hemolysin.
Blood agar was prepared, and bacterial cultures were inoculated on blood agar plates. Plates were allowed to incubate for 24-48 hours and observed for hemolysis. The clear zones around bacterial colonies showed complete hemolysis (Beta-hemolysis) of red blood cells and ability of bacteria to produce Beta-hemolysins. Greenish zones around bacterial colonies showed partial hemolysis (Alpha- hemolysis) of red blood cells and the ability of bacteria to produce Alpha hemolysins (Figure 7). No clearing showed that bacterial colony could not produce hemolysins (Gamma hemolysis) (Figure 8).
Preservation of Samples
The isolated samples were preserved using PBS and Glycerol. The preservative media was prepared by mixing together 70% Phosphate Buffer Saline (PBS) and 30% Glycerol in reagent bottle. The medium was autoclaved for 15 minutes at 121ºC to avoid any contamination. 1ml preservative media was transferred in each Eppendorf tube and isolated samples were inoculated in each tube. The preserved samples were stored at -20ºC until further processing.
Results and Discussion
Analysis of Clinical and Behavioural Data
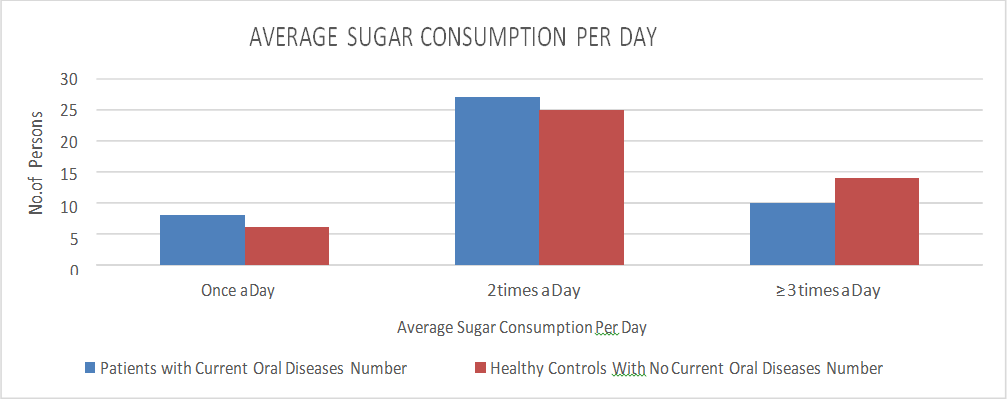
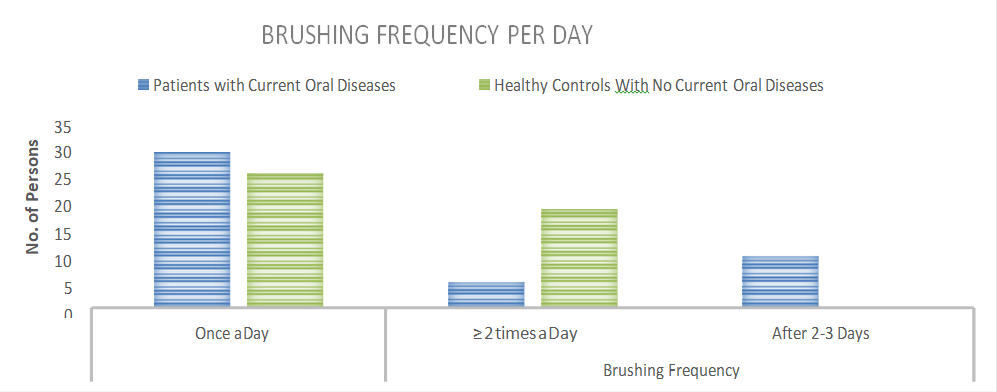
In the current study, information about clinical history and daily routine activities was gathered to find out which factors are more responsible for increased risks of oral disorders. Table 1 shows the behaviors adopted by respondents regarding their oral health. The information shows that increased frequency of oral health related behaviours resulted in poor oral health. Increased sugar consumption, low brushing frequency, over use of medications which are affecting oral normal flora, aggressive brushing, more consumption of acidic foods and soft drinks and smoking are the factors which were being adopted in a higher ratio in oral patients as compared to healthy respondents. Table 2 shows the frequency of past oral disorders in respondents of both groups. Respondents with current oral disorders showed greater frequency of oral problems as compared to healthy respondents. Table 3 shows frequency of average DMFT (Decayed, Missing, and Filled Teeth) of oral patients is greater than healthy subjects. Table 4 shows that increased oral disorders can increase the risk of systemic diseases. Ratio of systemic diseases was higher in oral patients as compared to healthy respondents, as, pathogenic microbes can get entry into bloodstream and can damage different organs.
| Oral Health Related Behaviors | Patients with Current Oral Diseases | Healthy Controls With No Current Oral Diseases | |||
|---|---|---|---|---|---|
| Number | Percentage | Number | Percentage | ||
| Average Sugar Consumption Per Day | Once a Day | 8 | 17.77% | 6 | 13.33% |
| 2 times a Day | 27 | 60% | 25 | 55.55% | |
| ≥ 3 times a Day | 10 | 22.22% | 14 | 31.11% | |
| Once a Day | 30 | 66.66% | 26 | 57.77% | |
| ≥ 2 times a Day | 5 | 11.11% | 19 | 42.22% | |
| Brushing Frequency | After 2-3 Days | 10 | 22.22% | 0 | 0 |
| Over-use of Medications | 30 | 66.66% | 11 | 24.44% | |
| Aggressive Mode of Brushing | 14 | 31.11% | 10 | 22.22% | |
| Acidic Food Consumption | 15 | 33.33% | 22 | 48.88% | |
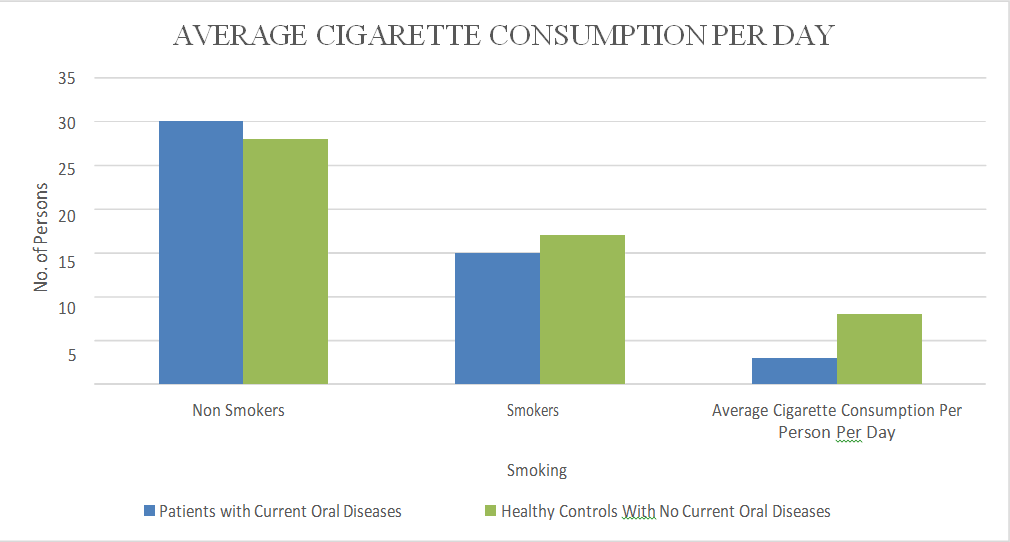
| Smoking | Non Smokers | 30 | 66.66% | 28 | 62.22% |
| Smokers | 15 | 33.33% | 17 | 37.77% | |
| Average Cigarette Consumption Per Person Per Day | 3 | 8 | |||
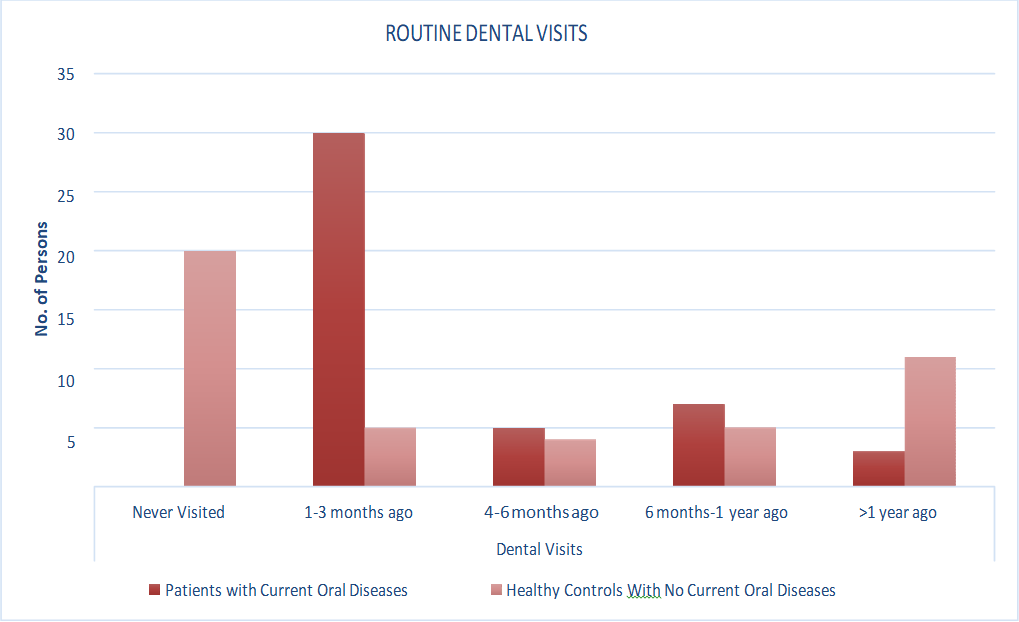
| Dental Visits | Never Visited | 0 | 0 | 20 | 44.44% |
| 1-3 months ago | 30 | 66.66% | 5 | 11.11% | |
| 4-6 months ago | 5 | 11.11% | 4 | 8.88% | |
| 6 months-1 year ago | 7 | 15.55% | 5 | 11.11% | |
| >1 year ago | 3 | 6.66% | 11 | 24.44% |
Table 1: Distribution of Respondents by Frequency of Oral Health Related Behaviours.
The analysis in Table 1 shows that more than 50% respondents in both groups consume white sugar 2 times a day while 22% oral patients have average sugar consumption of more than 3 times a day. 31% healthy respondents consume white sugar more than 3 times a day (Figure 9). This could increase the risk of dental caries, moreover, if the brushing frequency is once daily, this could aggravate these oral problems. 22% oral patients brush their teeth after 2-3 days and this behaviour resulted in serious oral problems. Over-use of mediations which disturb the normal oral flora can also increase frequency of oral problems, it is because, in the current analysis, 66% oral patients were habitual of over use of medicines. 22% of healthy respondents were also involved in this behaviour which could increase their risk of oral diseases. 31% oral patients and 22% of healthy respondents were used to aggressive brushing which can damage tissues and aggravate oral problems (Figure 10). Percentage of acidic food consumption was higher in healthy respondents as compared to oral patients. Smoking ratio was also greater in healthy respondents with average 8 cigarettes consumed per person per day (Figure 11). This could aggravate problems of dental stains and dental caries. Routine dental check-ups are necessary to maintain normal oral health. 66% oral patients had last visited dentist around 1-3 months ago while 44% healthy respondents had never visited dentist which put them on a risk of encountering oral problems.
| Oral Disorders | Patients With Current Oral Health Problems | Healthy Controls With No Current Oral Disorders | ||
|---|---|---|---|---|
| No. of Cases | Percentage | No. of Cases | Percentage | |
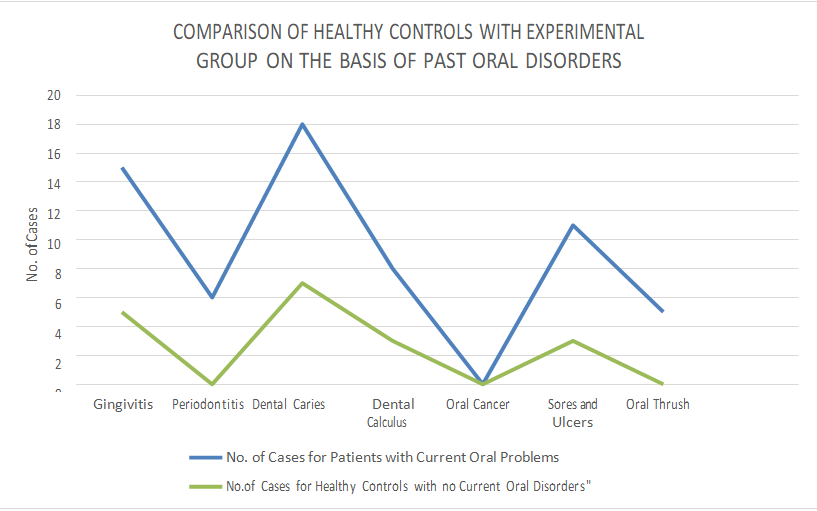
| Gingivitis | 15 | 27.27% | 5 | 11.11% |
| Periodontitis | 6 | 10.90% | 0 | 0 |
| Dental Caries | 18 | 32.72% | 7 | 15.55% |
| Dental Calculus | 8 | 14.54% | 3 | 6.66% |
| Oral Cancer | 0 | 0 | 0 | 0 |
| Sores and Ulcers | 11 | 24.44% | 3 | 8.57% |
| Oral Thrush | 5 | 11.11% | 0 | 0 |
Table 2: Distribution of respondents by Frequency of Past Oral Disorders.
The analysis of Table 2 shows that ratio of past oral disorders is greater in oral patients as compared to healthy respondents. Lack of proper treatment or lack of awareness about oral health related behaviors could be a reason of recurring infections in oral patients. Furthermore, many behavioral elements can play a significant role in aggravating these oral issues. People usually living in low socioeconomic conditions or have limited access to health care units are more prone to oral illnesses (Figure 13).
| Patients with Current Oral Diseases | Healthy Controls With No Current Oral Disorders | |||
|---|---|---|---|---|
| Male | Female | Male | Female | |
| No. of Study Subjects | 15 (33.3%) | 28 (62.22%) | 24 (53.33%) | 21 (46.66%) |
| Average DMFT | 05-Jun | 06-Jul | 01-Feb | 02-Mar |
Table 3: Distribution of Respondents by Frequency of Average DMFT.
The analysis of Table 3 shows that average DMFT in male oral patients is 5-6 while in female oral patients is 6-7. In healthy respondents, average DMFT in male is 1-2 while in female is 2-3. This represents that ratio of oral problems is higher in women as compared to men (Figure 14).
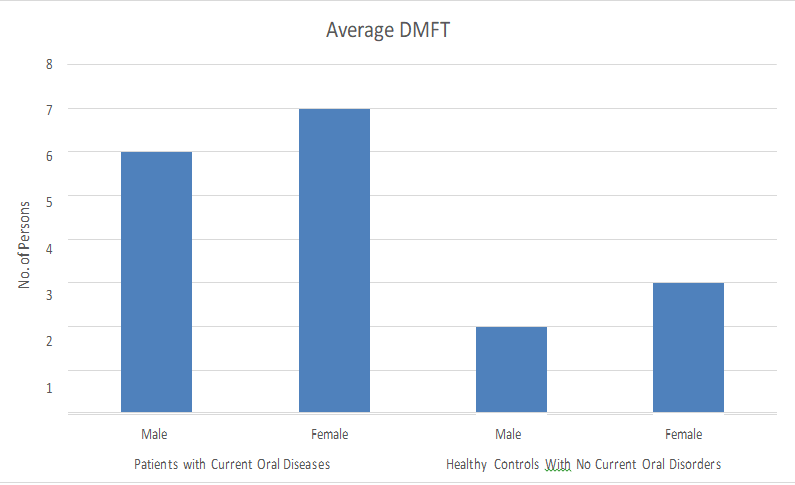
| Patients With Current Oral Health Problems | Healthy Controls With No Current Oral Disorders | |
|---|---|---|
| No. of Cases | No. of Cases | |
| Cardiovascular Diseases | 3 | 1 |
| Diabetes | 4 | 1 |
| Osteoporosis | 2 | 2 |
| Metabolic Syndromes | 11 | 5 |
| Adverse Pregnancy Outcomes | 5 | 1 |
| Bacterial Pneumonia | 0 | 0 |
| Atherosclerotic Disease | 0 | 0 |
Table 4: Distribution of Respondents by Frequency of current systemic diseases.
The analysis of Table 4 shows that the frequency of systemic disorders was greater in oral patients as compared to healthy respondents. The ratio of cardiovascular diseases, diabetes, metabolic syndromes and adverse pregnancy outcomes was higher in oral patients as compared to healthy controls. The highest frequency was showed for metabolic syndromes and adverse pregnancy outcomes. Thus, it was concluded from clinical data that oral pathogenic flora might be involved in systemic diseases through bacteremia or eternal routes. Pathogenic bacteria residing oral cavity can gain entry into blood and can infect number of organs by transmitting through blood circulation. Microbes in oral cavity can invade the gut and can cause number of metabolic syndromes (Figure 15).
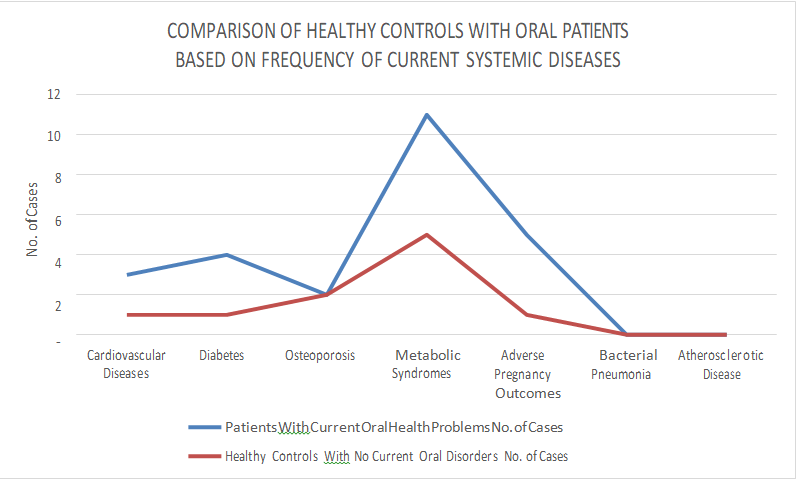
Figure 15: Comparison of Healthy Controls with Oral Patients on the basis of Frequency of Current Systemic Diseases. Isolation and Identification of Bacterial Isolates In the current study, a total of 34 different samples were collected from oral cavity of control and experimental groups. 17 samples were collected from healthy subjects with no current oral problems Figure 20 while 17 other samples were collected from oral patients suffering from different oral disorders (Figure 26). A total of 8 different bacterial species were isolated from samples of healthy controls while 10 different species were isolated from samples of oral patients. 7 bacterial species were identical in both groups while Escherichia coli, Pseudomonas aeruginosa, Corynebacterium, Actinobacteria and Streptococcus mutans were present only in samples of experimental group. This identification is Enterobacter isolated from 5 healthy controls and 5 oral patients as well. Escherichia coli were isolated from 6 oral patients, Actinobacteria from 6 oral patients, Pseudomonas aeruginosa from 4 and Corynebacterium from 6 oral pateints (Figures 16-19) (Figures 21-25). Tables 5-8 shows results of these biochemical tests.
| S.No | Colony Morphology | Gram Staining | |||||
|---|---|---|---|---|---|---|---|
| Shape | Edge | Elevation | Color | Texture | Gram Positive or Negative | Cell Shape | |
| 1 | Circular | Sharp | Convex | Golden- Yellow | Moist | Gram Positive | Cocci |
| 2 | Circular | Smooth | Convex | Greyish- White | Moist | Gram Negative | Cocci |
| 3 | Circular | Smooth | Convex | White | Moist | Gram Positive | Cocci |
| 4 | Circular | Smooth | Convex | Golden Yellow | Mucoid | Gram Positive | Cocci |
| 5 | Circular | Smooth | Convex | White | Mucoid | Gram Positive | Bacilli |
| 6 | Circular | Smooth | Umbonate | White | Dry | Gram Positive | Cocci |
| 7 | Circular | Smooth | Convex | Creamy White | Mucoid | Gram Negative | Bacilli |
| 8 | Circular | Entire | Convex | Creamy Yellow | Moist | Gram Positive | Cocci |
Table 5: Colony Morphology and Gram Staining of Bacterial species isolated from Healthy Controls.

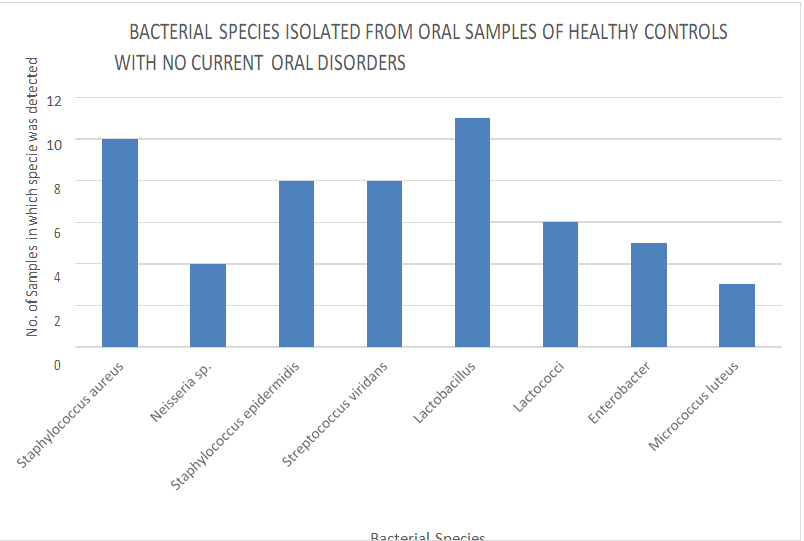
| Catalase Test | Coagulase Test | Sugar Fermentation Test | Simons Citrate Test | Methyl Red Test | Hemolysis Test | Bacterial Specie | No. of samples in which specie was detected | |
|---|---|---|---|---|---|---|---|---|
| Positive | Positive | Positive | Positive | Positive | β hemolysis | Staphylococcus aureus | 10 | |
| Positive | Negative | Positive | Positive | Negative | Neisseria sp. | 4 | ||
| Positive | Negative | Positive | Negative | Negative | γ- hemolysis | Staphylococcus epidermidis | 8 | |
| Negative | Negative | Positive | Positive | Negative | α hemolysis | Streptococcus viridans | 8 | |
| Negative | Negative | Positive | Negative | Negative | γ hemolysis | Lactobacillus | 11 | |
| Positive | Negative | Positive | Negative | Positive | γ hemolysis | Lactococci | 6 | |
| Positive | Negative | Positive | Positive | Negative | γ hemolysis | Enterobacter | 5 | |
| Positive | Negative | Negative | Positive | Negative | γ hemolysis | Micrococcus luteus | 3 |
Table 6: Biochemical Tests of Bacterial species isolated from Oral Samples of Healthy Controls.
| S.No | Colony Morphology | Gram Staining | |||||
|---|---|---|---|---|---|---|---|
| Shape | Edge | Elevation | Color | Texture | Gram Positive or Negative | Cell Shape | |
| 1 | Circular | Sharp | Convex | Golden- Yellow | Moist | Gram Positive | Cocci |
| 2 | Irregular | Smooth | Convex | White | Dry | Gram Positive | Bacilli |
| 3 | Circular | Smooth | Convex | White | Moist | Gram Positive | Cocci |
| 4 | Circular | Smooth | Convex | Golden- Yellow | Mucoid | Gram Positive | Cocci |
| 15 | Circular | Smooth | Convex | White | Mucoid | Gram Positive | Bacilli |
| 6 | Circular | Smooth | Umbonate | White | Dry | Gram Positive | Cocci |
| 7 | Circular | Smooth | Convex | Creamy- White | Mucoid | Gram Negative | Bacilli |
| 8 | Circular | Entire | Convex | Creamy Yellow | Moist | Gram Positive | Cocci |
| 9 | Circular | Smooth | Convex | Greyish- White | Moist | Gram Negative | Bacilli |
| 10 | Irregular | Smooth | Flat | Greenish | Moist | Gram Negative | Bacilli |
| 11 | Circular | Smooth | Flat | White | Dry | Gram Positive | Cocci |
Table 7: Colony Morphology and Gram Staining of Bacterial species isolated from Oral Patients.
| Catalase Test | Coagulase Test | Sugar Fermentation Test | Simons Citrate Test | Methyl Red Test | Hemolysis Test | Bacterial Specie | No. of samples in which specie was detected |
|---|---|---|---|---|---|---|---|
| Positive | Positive | Positive | Positive | Positive | β hemolysis | Staphylococcus aureus | 6 |
| Positive | Negative | Positive | Negative | Positive | γ hemolysis | Corynebacteria | 6 |
| Positive | Negative | Positive | Negative | Negative | γ- hemolysis | Staphylococcus epidermidis | 5 |
| Negative | Negative | Positive | Positive | Negative | α hemolysis | Streptococcus viridans | 11 |
| Negative | Negative | Positive | Negative | Negative | γ hemolysis | Lactobacillus | 7 |
| Positive | Negative | Positive | Negative | Positive | γ hemolysis | Lactococci | 9 |
| Positive | Negative | Positive | Positive | Negative | γ hemolysis | Enterobacter | 5 |
| Positive | Negative | Negative | Positive | Negative | γ hemolysis | Micrococcus luteus | 1 |
| Positive | Negative | Positive | Negative | Positive | γ hemolysis | Escherichia coli | 6 |
| Positive | Negative | Positive | Positive | Negative | β hemolysis | Pseudomonas aeruginosa | 4 |
| Negative | Negative | Positive | Negative | Positive | γ hemolysis | Actinobacteria | 6 |
Table 8: Results of different Biochemical tests of Bacterial species isolated from samples of oral Patients.
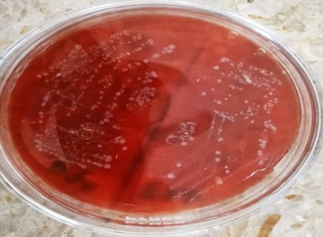
![Figure 26: Detection of Bacterial Samples from Patients with Oral Cavity Disorders. Discussion According to WHO definition of health, being healthy is a condition of whole social, physical and mental well-being rather than just the absence of disease or infirmity. Each person should be concerned about their oral health because it is an essential component of their overall well-being [25]. Many people consider mouth to be the entrance to the body. As a result, it’s critical to take necessary precautions to ensure oral health [26]. There are a number of behavioral factors which influence oral health of the people. Some of these include socioeconomic position, oral hygiene habits and lack of oral health education [27].](/fulltextimages/12071/fig_26.png)
Figure 26: Detection of Bacterial Samples from Patients with Oral Cavity Disorders. Discussion According to WHO definition of health, being healthy is a condition of whole social, physical and mental well-being rather than just the absence of disease or infirmity. Each person should be concerned about their oral health because it is an essential component of their overall well-being [25]. Many people consider mouth to be the entrance to the body. As a result, it’s critical to take necessary precautions to ensure oral health [26]. There are a number of behavioral factors which influence oral health of the people. Some of these include socioeconomic position, oral hygiene habits and lack of oral health education [27].
The ratio of past oral infections was higher in oral patients as compared to healthy controls. Among healthy controls, gingivitis 5 cases, periodontitis 0 case, dental caries 7 cases, dental calculus 3 cases, oral cancer 0 case, sores and ulcers 3 cases and oral thrush 0 case while among oral patients (experimental group) gingivitis 15 cases, periodontitis 6 cases, dental caries 18 cases, dental calculus 8 cases, oral cancer 0 case, sores and ulcers 11 cases and oral thrush 5 cases were observed. Similar study was conducted by some researchers who evaluated the oral health status of public and private school students . They identified eleven oral problems and the ratio of these problems varies highly among students of both schools. The study showed that there was a significant difference between oral health status of public and private school students and the factors involved were low socioeconomic status of public school students, lack of awareness about oral health, lifestyle and financial statuses [27].
In the current study, the link of oral infections to systemic diseases was also studied based on epidemiological information of study subjects. Large numbers of systemic diseases were observed in oral patients as compared to healthy controls. Cardiovascular diseases, diabetes, metabolic syndromes and adverse pregnancy outcomes were identified in high ratio in oral patients as compared to healthy controls. The highest frequency was showed for metabolic syndromes and adverse pregnancy outcomes. The most probable reason could be invasion of oral pathogenic bacteria in the gut through bacteremia or transfer of pathogenic microbes from placenta to fetus through bacteremia. In a related study, the association between oral health status and hygiene practices among adults and elderly with a history of coronary artery disease was investigated [28]. In adults, periodontal diseases were identified in 25.1% of healthy group and 41.9% of the cardiovascular risk group [28]. An elderly population at cardiovascular risk reported chewing and speaking issues to the tune of 40.0 and 17.5 percent, respectively [28]. In comparison to the healthy group, the risk group had a significantly greater prevalence of periodontal problems [28].
Strong evidence link systemic illnesses like cardiovascular diseases, diabetes and adverse pregnancy outcomes to periodontal diseases [29]. A 19% increase in the risk of cardiovascular disease is expected to result from periodontal disease [29]. Pre-term birth, low birth weight and preeclampsia are all linked to periodontitis [29]. When periodontal disease incidence and prevalence declines, so do the related systemic diseases and the financial burdens they place on the health care systems [29].
In the current study, a total of 34 different samples were collected from oral cavity of control and experimental groups. 17 samples were collected from healthy subjects with no current oral problems while 17 other samples were collected from oral patients suffering from different oral problems. A total of 8 different bacterial species were isolated from samples of healthy controls while 10 different species were isolated from samples of oral patients.
Out of isolated species, 7 bacterial species were identical in both groups while Escherichia coli, Pseudomonas aeruginosa, Corynebacterium, Actinobacteria and Streptococcus mutans were present only in samples of experimental group and Neisseria spp. were present only in samples of healthy controls. The bacterial species similar in both groups were Staphylococcus aureus, Staphylococcus epidermidis, Lactobacilli, Lactococci, Streptococcus viridans, Micrococcus luteus and Enterobacter. Bacterial species abundant in healthy controls were Lactobacilli and Staphylococci while in oral patients were Streptococci, Corynebacterium, Actinobacteria and Lactococci. A study was conducted by some researchers to detect bacterial flora of oral cavity based on 16SrRNA sequencing and the most predominant species identified belong to genera Streptococci, Neisseria, Fusobacterium, Actinomyces, Campylobacter and Veillonella [5].
Research was conducted to detect composition of oral bacterial flora from 10 healthy individuals with healthy oral tissues using culture-independent methods [29]. 9 different bacterial phyla were identified and 15 bacterial genera were conserved in all the study subjects [29]. Most abundant phyla identified were Proteobacteria, Actinobacteria and Bacteroidetes while less abundant phyla were Fusobacteria and Spirochaetes [29]. Thus, it was concluded that although each person’s mouth contains a distinct community of bacterial species, these communities are more comparable when grouped at the genus level [29].
In the present study, a comparison was made between oral flora of healthy controls and oral patients. Some of the species were present in both study groups but ecological disturbances can cause a shift in indigenous bacteria to increase in number and cause oral infections. Lactococci, Streptococci, Corynebacterium, Actinobacteria, Escherichia coli and Pseudomonas aeruginosa were found to be abundant in oral patients. These bacterial species could be causation of dental caries, periodontitis, gingivitis and oral lesions. Some more specific oral flora associated with different types of periodontal diseases include Porphyromonas gingivalis, Tannerella forsythia and Aggregatibacter actinomycetemcomitans [30]. The main indicators of oral health are Streptococci and Actinomyces [30]. Streptococci mutans are more closely realted with initiation of denta caries while enamel and dental lesions progression may be more related to Lactobacilli [30]. The behavioral and environmental factors play the most important role in maintaining oral health. Ecological disturbances can cause shifts in indigenous flora of oral cavity, thus, leading to a number of oral diseases [12].
Conclusion
High rates of sugar consumption, infrequent brushing, excessive medication use, consumption of acidic foods, high rates of smoking, aggressive brushing style, and lack of dental health knowledge are some of the factors which can play a role in exacerbating oral health problems. Unbalanced bacterial flora of oral cavity can play a significant part in systemic illnesses. Comparative study of bacterial diversity between healthy controls and oral patients revealed the presence of total 12 different bacterial species. Species conserved in both groups were Staphylococcus aureus, Staphylococcus epidermidis, Micrococcus luteus, Lactococci, Enterobacter, Lactobacilli and Streptococcus viridans group, but these were present in varying proportions. Escherichia coli, Pseudomonas aeruginosa, Corynebacterium, and Actinobacteria were recovered from samples taken from oral patients whereas Neisseria spp., were only isolated from healthy controls. Staphylococcus aureus, Lactobacilli, and Staphylococcus epidermidis were the most prevalent species in healthy controls, but Lactococci, Actinobacteria, Corynebacterium, and Streptococcus viridans group were more prevalent in oral patients.
References
-
Deo PN, Deshmukh R (2019) Oral microbiome: Unveiling the fundamentals. Journal of oral and maxillofacial pathology 23(1): 122-128.
-
Santacroce L, Man A, Charitos IA, Haxhirexha K, Topi S (2021) Current knowledge about the connection between health status and gut microbiota from birth to elderly. A narrative review. Frontiers in Bioscience 26(6): 135-148.
-
Bashir H, Bawa A, Kumar R (2022) Human microbiome: implication of age and external factors. In: Thomas S (Ed.), Human Microbiome. Springer, Singapore, pp: 1-12.
-
Dekaboruah E, Suryavanshi MV, Chettri D, Verma AK (2020) Human microbiome: an academic update on human body site specific surveillance and its possible role. Archives of microbiology 202(8): 2147-2167.
-
Requena T, Velasco M (2021) The human microbiome in sickness and in health. Revista Clinica Espanola 221(4): 233-240.
-
Sharma T, Gupta A, Chauhan R, Bhat AA, Nisar S, et al. (2022) Cross-talk between the microbiome and chronic inflammation in esophageal cancer: Potential driver of oncogenesis. Cancer and Metastasis Reviews 41: 281- 299.
-
Engstrand L, Lindberg M (2013) Helicobacter pylori and the gastric microbiota. Best practice & research Clinical gastroenterology 27(1): 39-45.
-
Jandhyala SM, Talukdar R, Subramanyam C, Vuyyuru H, Sasikala M, et al. (2015) Role of the normal gut microbiota. World journal of gastroenterology 21(29): 8787-8803.
-
Samaranayake L, Matsubara VH (2017) Normal oral flora and the oral ecosystem. Dental Clinics 61(2): 199-215.
-
Chen H, Xiao T, Ning Z, Li Q, Xiao E, et al. (2020) In-situ remediation of acid mine drainage from abandoned coal mine by filed pilot-scale passive treatment system: Performance and response of microbial communities to low pH and elevated Fe. Bioresource Technology 317: 123985.
-
Gustafsson A, Skogsberg J, Rejno A (2021) Oral health plays second fiddle in palliative care: an interview study with registered nurses in home healthcare. BMC palliative care 20: 1-11.
-
Dong L, Yin J, Zhao J, Ma SR, Wang HR, et al. (2018) Microbial similarity and preference for specific sites in healthy oral cavity and esophagus. Frontiers in microbiology 9: 1603.
-
Baker JL, Bor B, Agnello M, Shi W, He X (2017) Ecology of the oral microbiome: beyond bacteria. Trends in microbiology 25(5): 362-374.
-
Radaic A, Kapila YL (2021) The oralome and its dysbiosis: New insights into oral microbiome-host interactions. Computational and Structural Biotechnology Journal 19: 1335-1360.
-
Jepsen S, Blanco J, Buchalla W, Carvalho JC, Dietrich T, et al. (2017) Prevention and control of dental caries and periodontal diseases at individual and population level: consensus report of group 3 of joint EFP/ORCA workshop on the boundaries between caries and periodontal diseases. Journal of clinical periodontology 44: S85-S93.
-
Phipps KR, Ricks TL (2016) The oral health of American Indian and Alaska native adult dental patients: results of the 2015 IHS oral health survey. Indian Health Service data brief.
-
Aurlene N, Manipal S, Prabu D, Rajmohan (2020) Prevalence of oral mucosal lesions, dental caries, and periodontal disease among patients with systemic lupus erythematosus in a teaching hospital in Chennai, Tamil Nadu. Journal of Family Medicine and Primary Care 9(7): 3374.
-
He J, Li Y, Cao Y, Xue J, Zhou X (2015) The oral microbiome diversity and its relation to human diseases. Folia microbiologica 60(1): 69-80.
-
Johnson CD, Jones S, Paranjothy S (2017) Reducing low birth weight: prioritizing action to address modifiable risk factors. Journal of Public Health 39(1): 122-131.
-
Hansen GM, Egeberg A, Holmstrup P, Hansen PR (2016) Relation of periodontitis to risk of cardiovascular and all-cause mortality (from a Danish nationwide cohort study). The American journal of cardiology 118(4): 489- 493.
-
Genco RJ, Sanz M (2020) Clinical and public health implications of periodontal and systemic diseases: An overview. Periodontology 83(1): 7-13.
-
Peng X, Cheng L, You Y, Tang C, Ren B, et al. (2022) Oral microbiota in human systematic diseases. International journal of oral science 14: 14.
-
Uwitonze AM, Uwambaye P, Isyagi M, Mumena CH, Hudder A, et al (2018) Periodontal diseases and adverse pregnancy outcomes: Is there a role for vitamin D?. The Journal of steroid biochemistry and molecular biology 180: 65-72.
-
Olsen I, Yamazaki K (2019) Can oral bacteria affect the microbiome of the gut?. Journal of oral microbiology 11(1): 1586422.
-
Glick M, Williams DM, Kleinman DV, Vujicic M, Watt RG, et al. (2016) A new definition for oral health developed by the FDI World Dental Federation opens the door to a universal definition of oral health. British dental journal 221: 792-793.
-
Iyer P (2023) Oral Cavity is the Gateway to the Body: Role of Oral Health Professionals: A Narrative Review. Journal of the California Dental Association 51(1): 2193372.
-
Spanemberg J, Cardoso J, Slob E, Lopez-Lopez J (2019) Quality of life related to oral health and its impact in adults. Journal of stomatology, oral and maxillofacial surgery 120(3): 234-239.
-
Lee SK, Hwang SY (2021) Oral health in adults with coronary artery disease and its risk factors: a comparative study using the Korea National Health and Nutrition Examination Survey data. BMC Cardiovascular Disorders 21: 71.
-
Nazir MA (2017) Prevalence of periodontal disease, its association with systemic diseases and prevention. International journal of health sciences 11(2): 72-80.
-
Durand R, Roufegarinejad A, Chandad F, Rompre PH, Voyer R, et al. (2019) Dental caries are positively associated with periodontal disease severity. Clinical Oral Investigations 23(10): 3811-3819.
- Evaluation of Proximate and Mineral Compositions of Momordica charantia L. (Cucurbitaceae)
- Targeting Superbugs: Efficacy of Bacteriophage Therapy against Antibiotic-Resistant Pseudomonas Aeruginosa in Urinary Tract Infections
- Genetic Insights into Prepubertal Gynecomastia: A Comprehensive Analysis of a Rare 45,X[2]/ 46,X, + mar[28] Karyotype
- The Efficiency of Biological Treatment Plants in Some Private Hospitals in the City of Basra, Iraq
- Exploring the Combined Efficacy of Carvacrol and Friedelin against Multi-Drug Resistant Bacteria in Upper and Lower Respiratory Tract Infections
- Isolation, Identification and Comparative Analysis of Oral Microbial Communities in Smokers and Non-Smokers: A Scientific Investigation