Evaluating the Potential Statin-Drug Interactions among Older Patients with Chronic Diseases in Sana’a City, Yemen
Introduction
Physiological changes occur with aging in all organ functions, including renal and liver function [1], and all drug pharmacokinetic (PK) phases, from absorption to elimination, are affected [2]. Seniors suffer from chronic diseases and comorbidities and are the major consumers of drugs (40% of all elderly use > 5 drugs per week, and 12% of older patients use > 10 drugs per week) [3], thus increasing the potential risk of drug-drug interactions (DDIs) that are often not seen in practice settings and may lead to adverse drug reactions (ADRs). Elderly individuals are often managed with multiple concomitant medications (poly-pharmacy) which is defined as the use of more than 5–10 drugs than clinically indicated for the treatment of patients with multiple risks [4]. The prevalence of inappropriate drug use in the seniors ranges between 11.5% and 62.5%. ADRs account for more than 5% of hospital admissions and the elderly are represented excessively in this patients group [5]. Drug side-effects are seven times more frequent in the older adults than in younger patients [6]. So, older patients should be regularly reevaluated for the potential risk of DDIs. The incidence of DDIs is corresponding to the number of drugs prescribed. If more medications are prescribed at the same time, the risk of ADRs for concurrent medications rises from 13% to 38% and 82% [7]. ADRs may cause high morbidity and mortality and increase healthcare costs, and some ADRs are preventable such as inappropriate prescribing, unsuitable combinations of drugs, poor compliance, and errors in monitoring [8].
Statins are a well-established class of drugs for the treatment of elevated cholesterol and reduce the risk of cardiovascular morbidity and mortality in patients either in primary or secondary prevention of cardiovascular disease (CVD) [9]. Globally, most of the older patients take a statin on a long-term basis [10]. The safety and adverse effects of statins are of special concern especially in older patients with multiple chronic conditions on concomitant drugs due to risk of DDIs [11]. Statin mono-therapy is generally well tolerated but elderly patients on poly-pharmacy may experience ADRs such as statin- associated muscle symptoms due to increased exposure to statins caused by co-prescribed drugs that may lead to statin non-adherence and/or discontinuation [12], or statin induced hepatotoxicity [13].
Polypharmacy is common in older people, with over 50 % of elderly taking five or more medications [14]. As medication use and the incidence of drug-related problems increase with age [15], more vigilance to ensure the safe and proper use of medications is required. Although the use of multiple medications may be necessary in some patients, this can lead to drug-drug interactions [16]. The prevalence of drug-drug interactions in older patients has been studied extensively. A recent review of the clinical outcomes of drug- drug interactions in older patients in different healthcare settings [17] found that the prevalence of potential drug-drug interactions ranged from 1.5 to 47.4 %, and they increased the risk of hospitalization.
Statins are the most commonly prescribed drugs in many developed countries [18] and are used by more than 40 % of Australians elderly [19]. The management of cardiovascular diseases such as ischemic heart disease and heart failure, as well as co-morbidities, will often involve the use of multiple medications which can increase the risk of statin-drug interactions in older patients [20]. In addition, the long-term use of statin therapy may lead to significant potential for statin-drug interactions such as muscle-related symptoms, slow walking speed, and increased risk of falls [21].
Statin-drug interactions are primarily pharmacokinetic, involving altered drug metabolism via the cytochrome P450 system or drug transporters [22]. Drug interactions that raise the plasma concentration of statins can increase the risk of dose-dependent adverse effects including myalgia, myopathy, and rhabdomyolysis. However, the interaction potential differs between statins due to differences in their pharmacokinetics [20]. The risk of statin-drug interactions may be higher with lipophilic statins such as simvastatin, atorvastatin, and lovastatin that are extensively metabolized by CYP3A4 enzymes, than for hydrophilic statins such as rosuvastatin or pravastatin. Therefore, lipophilic statins are highly susceptible to drug interactions with CYP3A4 inhibitors/inducers [23]. Such differences in interaction potential are important to consider because medications that act on CYP450 are commonly used in older people [24].
The problem that this study addresses is that the presence of the interactions of statins will result in either increased toxicity or adverse effects, which, in turn, leads to less adherence by the patients to the medications, or decreased affectivity which results in therapeutic and prevention failure. Evaluating the prevalence and severity levels of statin-drug interactions among elderlies will lead to increased knowledge about statin-drug interactions and their severity levels and how they should be avoided and managed.
In general, the current study aims to evaluate the prevalence and severity of the potential statin-drug interactions among older adult patients (55 years or older) who have received statin therapy for a period of 18 months from January 2021 to June 2022 in Sana’a city. The main specific objectives of this study:
- To evaluate the prevalence of the potential statin-drug interactions.
- To evaluate the severity of the potential statin-drug interactions.
- To determine the most commonly interacting statin agent.
- To identify the most commonly interacting drugs with statins.
- To identify the most commonly prescribed drugs along with statins.
- To determine the most common type of statin-drug interactions mechanism.
- To give an average of the number of drugs the elderly take.
- To determine the most common comorbidities associated with statin therapy.
Materials and Methods
A retrospective cross-sectional study was carried out from January 2021 to June 2022 in Sana’a, Science and Technology University hospital. All elderly (age 55 years and above) patients’ medical records of cardiovascular disease and diabetes mellitus type 2 and with adequate documentation were included in the study. All cardiovascular patients’ medical records of age 54 years and below as well as charts recording non-cardiovascular and non-DM2 disease were excluded from the study. Data were collected from 200 patients’ medical records using a structured data collection format. The format was prepared with different sections important to fill basic demographic information like age and sex, drugs administered, and co-morbidities or diseases identified. The interactions between the drugs were assessed using Medscape and Lexicomp online drug interaction checkers.
Study Design
A retrospective cross-sectional study of all patients who attended the clinic; Data were collected through a retrospective electronic medical records review of all of the patients who were managed at the clinic between January 2021 and June 2022.
Study Period and Setting
This study was carried out from January 2021 to June 2022 for a period of 18 months; the samples of this study were collected from discharged patients in Science and Technology University hospital in Sana’a city. The hospital of Science and Technology University is a general hospital that provides comprehensive, high-quality health care to people of all ages. The available care includes emergency care, general medicine, surgery, and highly specialized treatments.
Sample Size
The total numbers of patients with complete medical records was 1053 out of which 200 patients aged 55 years old and above were discharged from the hospital over duration of 18 months. The selection criteria included patients aged 55 years and older that received statin therapy in the last 18 months.
Inclusion Criteria
Medical records in the hospital database were filtered by diagnosis and time of discharge. Medical records of patients that were discharged from the hospital between January 2021 and June 2022 were included. Medical records of patients with cardiovascular disease or type 2 diabetes mellitus were included. Medical records of male and female patients aged 55 years old and above were included.
Exclusion Criteria
Medical records of male and female patients younger than 55 years old and medical records of patients who didn’t receive statin therapy.
Data Collection
Findings were recorded in a predesigned data-collecting format, data collected included name, age, gender, weight, diagnosis, medications with their dosages and frequencies of dosing, most recently available BP, HbA1c, Sr.cr, lipid profile (including total cholesterol, triglyceride, LDL, and HDL), and liver function (including AST and ALT) and the presence of drug interactions was found using Medscape as well as Lexicomp software and recorded in the bottom of the format.
Principally, electronic medical records of older adult patients receiving statin therapy were used for collecting the required data for the study. The obtained data were written down in a predesigned data-collecting format. The medications found to be used by the patients-including an agent from statin drugs-were checked for the presence of any drug interaction using the interaction checkers of both Medscape and Lexicomp and written down in the same format of the patient.
Statistical Analysis
Statistical analysis was done by SPSS software version 21.0 by using Pearson’s Chi-square & the bivariate Pearson correlation test. Categorical variables were presented as frequencies and percentages.
Ethical Approval
Ethical clearance was obtained from the qualified authorities. The study protocol was approved by the ethics committee of hospital of university sciences and technology and the university.
Results
Demographic Data
A total of 1086 patient records were examined, out of which 200 prescriptions of statins were identified. The mean age was 66.5 years old (± SD 6 years). 103 (51.5%) were male and 97 (48.5%) were female. 104 (52%) had two comorbidities, while 37 (18.5%) had three comorbidities. The vast majority of patients were diagnosed with type 2 diabetes mellitus. Demographic characteristics of the patients receiving statins are presented in Table 1.
| Item | Number of prescriptions | Percentage | |
|---|---|---|---|
| Age | 55-60 | 61 | 30.50% |
| 61-65 | 59 | 29.50% | |
| 66-70 | 50 | 25.00% | |
| 71-75 | 22 | 11.00% | |
| 76-80 | 5 | 2.50% | |
| 81-85 | 2 | 1.00% | |
| >85 | 1 | 0.50% | |
| Gender | Male | 103 | 51.50% |
| Female | 97 | 48.50% | |
| Diagnosis | Hypertension | 53 | 15.50% |
| IHD | 37 | 10.90% | |
| Stroke | 49 | 14.40% | |
| Diabetes mellitus 2 | 132 | 38.70% | |
| Others | 70 | 20.50% |
Table 1: Demographic characteristics of the patients receiving statin
Blood Pressure
As this study analyzed the blood pressure readings of the patients, it found that the majority of the patients had high blood pressure. 48.1% of them had high blood pressure, while 38.0 % of patients had normal blood pressure. It was also found that 14% of the patients had low blood pressure.
Heart Rate
Heart rate readings showed that 92.9% of the patients had normal heart rates, while 7.1% of them had increased heart rates.
Laboratory Test Results
Lipid Profile
This study analyzed the laboratory result of the most recently available; total cholesterol, triglyceride, low-density lipoprotein and high-density lipoprotein. For the total cholesterol, 65.4% of the patients had normal levels and 34.6% of them had high total cholesterol levels. However, the results of triglyceride were 57.8% normal and 42.2% high test results. Additionally, low-density lipoprotein test results were normal in 66.1% of the patients and 33.9% of the patients had high levels of low-density lipoprotein. Furthermore, high-density lipoprotein levels were 53.7% had normal levels of high-density lipoprotein, whereas 46.3% of them had low levels of high-density lipoprotein. The percentage of the results of these laboratory tests is illustrated in Table 2.
| Lipid Profile Test | Normal | High | Low |
|---|---|---|---|
| Total cholesterol | 65.40% | 34.60% | 0% |
| Triglyceride | 57.80% | 42.20% | 0% |
| Low-density lipoprotein (LDL) | 66.10% | 33.90% | 0% |
| High-density lipoprotein (HDL) | 53.70% | 0% | 46.30% |
Table 2: The percentage of the results of lipid profile laboratory tests HbA1c
After analysis, the result of the most recently available HbA1c shows that only 18.4% of the patients had normal HbA1c levels and 81.6% of them had high levels of HbA1c.
Serum Creatinine
The levels of serum creatinine were normal in 47.7% of the patients and high in 15% of them. It was found that 37.3% of the patients had low levels of serum creatinine.
Liver Function Tests
This study included two tests, ALT and AST. The results show that 86.8% of the patients had normal ALT levels; whereas 13.2% of them had high ALT levels. AST levels were normal in 78% of the patients and high in 22% of them Table 3.
| Variable | Normal | High | Low |
|---|---|---|---|
| HbA1c | 18.40% | 81.60% | 0% |
| Serum creatinine | 47.70% | 15% | 37.30% |
| ALT | 86.80% | 13.20% | 0% |
| AST | 78% | 22% | 0% |
Table 3: The readings of HbA1c, S.cr, ALT, and AST
Statin Drugs
Two statins have been identified in analyzed pharmacotherapies: atorvastatin 120 (60%) and rosuvastatin 80 (40%).
Concomitant Drugs
The average number of other concomitant drugs was 5.49 (±SD 2.585). The most commonly prescribed co- medications were aspirin, oral antidiabetics, pantoprazole, beta-blockers, and clopidogrel. All co-administered drugs and their percentages are listed in Table 4.
| Concurrently used drug | Concurrently used drug | Concurrently used drug | ||||||
|---|---|---|---|---|---|---|---|---|
| Medication | No. | % | Medication | No. | % | Medication | No. | % |
| Aspirin | 115 | 57.50% | Enoxaparin | 7 | 3.50% | Lactulose | 2 | 1.00% |
| Metformin | 93 | 46.50% | Dapagliflozin | 7 | 3.50% | Magnesium | 2 | 1.00% |
| Pantoprazole | 52 | 26.00% | Olmesartan | 7 | 3.50% | Ciprofloxacin | 2 | 1.00% |
| Bisoprolol | 38 | 19.00% | Enalapril | 6 | 3.00% | Cefixime | 2 | 1.00% |
| Clopidogrel | 38 | 19.00% | Spironolactone | 6 | 3.00% | Amoxicillin | 1 | 0.50% |
| Glibenclamide | 36 | 18.00% | Thioctic lipoic acid | 6 | 3.00% | Alendronate | 1 | 0.50% |
| Hydrochlorothiazide | 29 | 14.50% | Tamsulosin | 6 | 3.00% | Imipenem | 1 | 0.50% |
| Amlodipine | 27 | 13.50% | Ceftriaxone | 6 | 3.00% | Alfacalcidol | 1 | 0.50% |
| vitB1B6B12 | 27 | 13.50% | Vinpocetine | 5 | 2.50% | Carbamazepine | 1 | 0.50% |
| Sitagliptin | 25 | 12.50% | Betahistine | 5 | 2.50% | Amiodarone | 1 | 0.50% |
| Ramipril | 22 | 11.00% | Nitroglycerine | 5 | 2.50% | Isosorbide mononitrate | 1 | 0.50% |
| Citicoline | 18 | 9.00% | Azithromycin | 4 | 2.00% | Eprosartan | 1 | 0.50% |
| Paracetamol | 18 | 9.00% | Vitamin C | 4 | 2.00% | Cholecalciferol | 1 | 0.50% |
| Glimepiride | 17 | 8.50% | Dipyridamole | 4 | 2.00% | Domperidone | 1 | 0.50% |
| Carvedilol | 16 | 8.00% | Folate + vitB6B12 | 4 | 2.00% | Carbamazepine | 1 | 0.50% |
| Vildagliptin | 15 | 7.50% | Ezetimibe | 4 | 2.00% | Prednisolone | 1 | 0.50% |
| Lisinopril | 15 | 7.50% | sulpride/ mebeverine | 3 | 1.50% | Lansoprazole | 1 | 0.50% |
| omega3 | 14 | 7.00% | Nebivolol | 3 | 1.50% | Chondroitin | 1 | 0.50% |
| Gabapentin | 14 | 7.00% | Caffeine | 3 | 1.50% | Glucosamine | 1 | 0.50% |
| Losartan | 13 | 6.50% | Piracetam | 3 | 1.50% | Alprazolam | 1 | 0.50% |
| vitB12 | 13 | 6.50% | Secnidazole | 3 | 1.50% | HCG | 1 | 0.50% |
| Candesartan | 13 | 6.50% | amoxicillin/ clavulanic | 3 | 1.50% | Pentoxifylline | 1 | 0.50% |
| Esomeprazole | 13 | 6.50% | Chlorzoxazone | 3 | 1.50% | Risperidone | 1 | 0.50% |
| Torsemide | 12 | 6.00% | Gliclazide | 3 | 1.50% | Diclofenac Na | 1 | 0.50% |
| Vitamin E | 12 | 6.00% | Omeprazole | 3 | 1.50% | Fluphenazine | 1 | 0.50% |
| Insulin | 12 | 6.00% | Levothyroxine | 2 | 1.00% | Ketoprofen | 1 | 0.50% |
| Fenofibrate | 11 | 5.50% | Calcitriol | 2 | 1.00% | mg.al silicate simethicone | 1 | 0.50% |
| Pregabalin | 11 | 5.50% | Formoterol | 2 | 1.00% | Nifedipine | 1 | 0.50% |
| Pioglitazone | 11 | 5.50% | Quetiapine | 2 | 1.00% | Nitrofurantoin | 1 | 0.50% |
| Levofloxacin | 11 | 5.50% | Cefuroxime | 2 | 1.00% | Nortriptyline | 1 | 0.50% |
| Allopurinol | 9 | 4.50% | Levetiracetam | 2 | 1.00% | Tramadol | 1 | 0.50% |
| Vitamin D | 8 | 4.00% | Ondansetron | 2 | 1.00% | Trimebutine | 1 | 0.50% |
| Empagliflozin | 8 | 4.00% | Perindopril | 2 | 1.00% | Valsartan | 1 | 0.50% |
| Furosemide | 7 | 3.50% | Budesonide | 2 | 1.00% | Warfarin | 1 | 0.50% |
Table 4: Concomitant Medications Co-prescribed with Statins
Statin-Drug Interactions
The Prevalence of Potential Statin-Drug Interactions (According to Lexicomp)
Generally speaking, out of 200 patients, there were 175 (87.5%) individuals had a total of 865 clinically significant drug-drug interactions. 767 (88.67%) of which were category C, 95 (10.98%) were category D, and 3 (0.35%) category X. Specifically speaking, given that only categories C, D, and X are clinically significant, the results show that, out of 200 patients, there were 55 (27.5%) individuals had a total of 72 clinically significant statin-drug interactions.
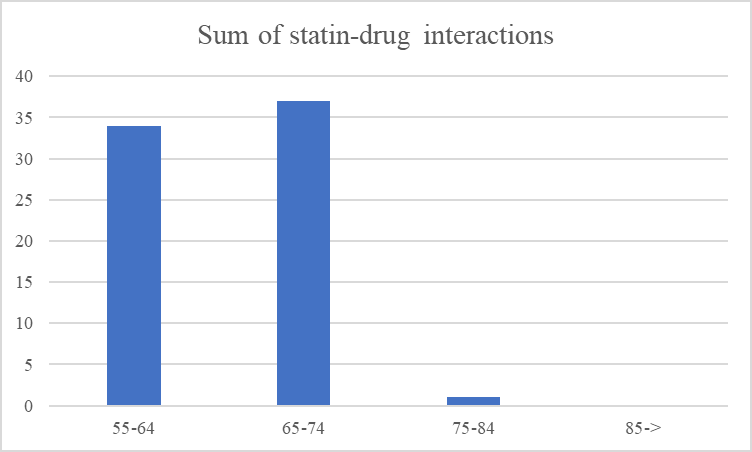
Statin-drug interactions represented (8.3%) of the total drug-drug interactions and out of 72 statin drug interactions, atorvastatin accounted for 51 (70.8%) of them and rosuvastatin accounted for 21 (29.2%). It was shown that the age group 66 to 70 is associated with the most statin-drug interactions (Figure 1).
It was also shown that the number of comorbidities was associated with more concomitant drugs (P-value < .001) and also, the number of concomitant drugs was shown to be strongly associated with more statin-drug interactions (P-value < .001) (Table 5).
| Variable | Age | No. of statin-DDIs | No. of comorbidities | No. of drugs | |
|---|---|---|---|---|---|
| Age | Pearson Correlation | 1 | 0.087 | -0.064 | 0.089 |
| Sig. (2-tailed) | 0.22 | 0.367 | 0.208 | ||
| N | 200 | 200 | 200 | 200 | |
| No. of Statin- DDIs | Pearson Correlation | 0.09 | 1 | -0.056 | 0.365 |
| Sig. (2-tailed) | 0.22 | 0.432 | 0 | ||
| N | 200 | 200 | 200 | 200 | |
| No. of comorbidities | Pearson Correlation | -0.06 | -0.056 | 1 | 0.228 |
| Sig. (2-tailed) | 0.37 | 0.432 | 0.001 | ||
| N | 200 | 200 | 200 | 200 | |
| No. of Drugs | Pearson Correlation | 0.09 | 0.365 | 0.228 | 1 |
| Sig. (2-tailed) | 0.21 | 0 | 0.001 | ||
| N | 200 | 200 | 200 | 200 |
Table 5: The correlation between the most important factors that might affect the occurrence of statin-drug interactions It was f
| Interacting drug | Number of prescriptions | Percent | The higher Severity |
|---|---|---|---|
| Clopidogrel | 17 | 23.61% | C |
| Sitagliptin | 14 | 19.44% | C |
| Amiodarone | 10 | 13.89% | C |
| Carvedilol | 8 | 11.11% | C |
| fenofibrate | 5 | 6.94% | C |
| Colchicine | 5 | 6.94% | D |
| Carbamazepine | 4 | 5.56% | D |
| Spironolactone | 2 | 2.78% | C |
| Itraconazole | 2 | 2.78% | D |
| Telithromycin | 2 | 2.78% | D |
| Cyclosporine | 1 | 1.39% | X |
| Warfarin | 1 | 1.39% | C |
| Verapamil | 1 | 1.39% | D |
| Total | 72 | 100.00% |
Table 6: The potentially interacting drug with statins according to Lexicomp
The Severity of the Potential Statin-Drug Interactions (According to Lexicomp)
Out of 72 statin-drug interactions, this study found 57
(79.17%) category C interactions, 14 (19.44%) category D interactions and only 1 (1.39) category X interaction (Table 7).
| Severity Level | Number of prescriptions | Percent |
|---|---|---|
| C (Monitor therapy) | 57 | 79.17% |
| D (Consider therapy modification) | 14 | 19.44% |
| X (Avoid combination) | 1 | 1.39% |
| Severity level | No. of DDIs | Percent (%) |
| Serious | 15 | 18.75% |
| Monitor closely | 63 | 78.75% |
| Minor | 2 | 2.50% |
Table 7: The percentage of the severity levels of statin-drug interactions Potentially Interacting Drugs with Statins (According
9).
The results show that the medicines potentially interacting with statins were prescribed to 54 patients (27% of all patients who received statin treatment). A total of 80 statin-drug interactions, 62 of those interactions which represent (77.5%) were with medicines that potentially interacted with atorvastatin and 18 which represent (22.5%) of those interactions were with medicines that potentially interacted with rosuvastatin. Drugs that were mainly involved in statin-drug interactions were glyburide, fenofibrate, pioglitazone, carbamazepine, and others. Glyburide accounted for the majority of statin-drug interactions. The numbers and frequencies of the drugs that potentially interact with statins are illustrated in Table 8.
| Interacting Drug | Atorvastatin | Rosuvastatin | ||
|---|---|---|---|---|
| No. of DDIs | Percent | No. of DDIs | Percent | |
| Amitriptyline | 1 | 1.30% | 0 | 0% |
| Carbamazepine | 4 | 5.00% | 0 | 0% |
| Fenofibrate | 9 | 11.30% | 2 | 2.50% |
| Glyburide | 35 | 43.80% | 8 | 10.00% |
| Metronidazole | 1 | 1.30% | 0 | 0% |
| Pioglitazone | 8 | 10.00% | 6 | 7.50% |
| Prednisolone | 1 | 1.30% | 0 | 0% |
| Risperidone | 1 | 1.30% | 0 | 0% |
| Valsartan | 2 | 2.50% | 0 | 0% |
| Niacin | 0 | 0% | 1 | 1.30% |
| warfarin | 0 | 0% | 1 | 1.30% |
Table 9: The Potentially Interacting Drugs with Statins according to Medscape
The results show that 156 (78%) of the patients’ prescriptions contain at least one clinically significant potential interaction and 54 (27%) contain at least one clinically significant potential statin-drug interaction. 80 statin-drug interactions were found, 62 (77.5%) of which involved atorvastatin and 18 (22.5%) of which involved rosuvastatin.
The Severity of the Potential Statin-Drug Interactions (According to Medscape)
Out of the 80 statin-drug interactions, 15 (18.75%) were ‘serious’ interactions, 63 (78.75%) were ‘monitor closely’ interactions, and 2 (2.5%) were ‘minor’ interactions (Table
The Severity of the Potential Statin-Drug Interactions
46 (57.5%) were pharmacokinetic 32 (40%) were pharmacodynamic and 2 (2.5%) were unknown mechanism (Table 10).
| No. of DDIs | Percent (%) | |
|---|---|---|
| Pharmacodynamics | 32 | 40% |
| Pharmacokinetics | 46 | 57.50% |
| Unknown/unclear | 2 | 2.50% |
Table 8: The Mechanism of Statin-Drug Interactions
Discussion
The results of blood pressure readings of the patient were supporting the idea that most of the patient who took statin therapy has high blood pressure. This study found that out of the 200 patients, 104 (52%) had two comorbidities, while 37 (18.5%) had three comorbidities. The vast majority were diagnosed with type 2 diabetes mellitus.
It was also found that the mean number of concomitant prescribed medications along with statin agents was 5.49 (±SD 2.585). And the most commonly co-prescribed medications were aspirin, clopidogrel, oral antidiabetics, pantoprazole, beta blockers, and CCBs. This is also supported by the reported results of a recent study that stated that the mean number of concomitant medicines prescribed to patients receiving statin therapy was 5.4 (SD=1.9) and ranged from 2 to 18 [25, 26].
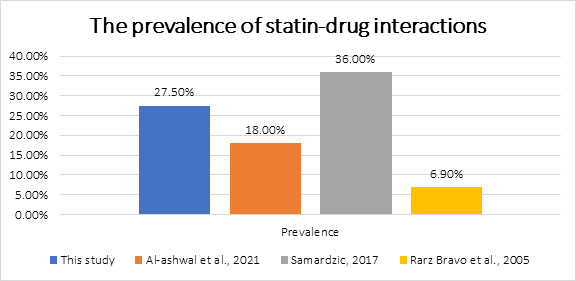
It was found that around 27% of the patients had at least one clinically significant potential statin-drug interaction. A total of 72 statin-drug interactions were found in 55 prescriptions out of 200 prescriptions. This is consistent with the findings of a recent study in Bulgaria that reported (26.1% at hospital admission, and 24.4% at discharge [27].
A comparison of the prevalence of statin-drug interactions between this study and other three studies is illustrated in Figure 2.
This study also revealed that as the number of comorbidities increases the potential statin-drug interactions increases as well (.228, p value < .001). And as the number of concomitant drugs increases, the number of interactions increases too (.365 p value < .001). These statistics were supported by Al-Ashwal, et al. [27].
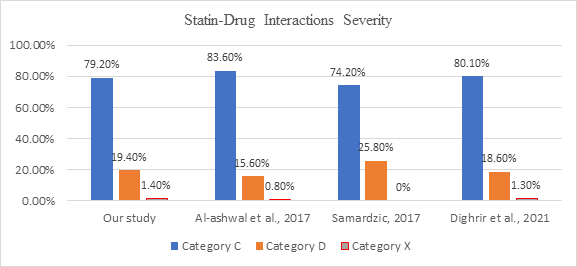
Most statin interactions are classified as category C (79.17 %) meaning that the patient’s medication should be monitored, and category D (19.44%) meaning that the patient should be considered for therapy modification. Additionally, the patient has a substantial chance of an adverse drug reaction, which increases the likelihood of hospitalization. Only (1.39%) of the interactions were category X which indicates that the medication should be avoided. Not to mention the interactions that were category B and A, because only categories C, D, and X were considered clinically significant.
Several similar studies support these statistics, the results of this study are in accordance with previously reported results that claimed that (83.6%) DDIs were class C (monitor therapy), (15.6%) were class D (therapy modification), and only one (0.8%) class X (avoid combination) [27].
Another study was conducted in Saudi Arabia by Dighrir, et al. [28] says that statin-drug interactions category C were about (80.13%) and those in category D were (18.59%) and (1.28%) represented category X.
A study was conducted in Croatia in 2016 by Samardzic, et al. [29] showed that statin-drug interactions category C represented (74.2%) and statin-drug interactions category D represented (25.8%). however, in that study there was not any category X statin-drug interactions. A comparison of the severity levels of statin-drug interactions of this study and three other studies is demonstrated in Figure 3.
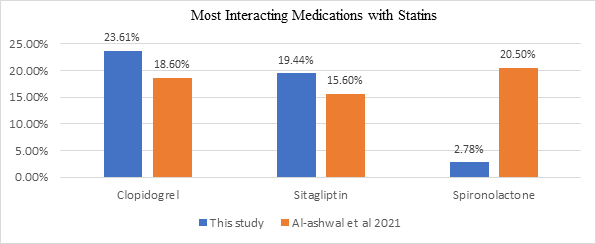
It was found that the most frequently reported statin-drug interactions were with clopidogrel, sitagliptin, amiodarone, and carvedilol because these drugs are regularly prescribed to treat chronic diseases. These findings are also consistent with the findings of the recent study of Al-Ashwal, et al. [27]. A comparison of the most three medications involved in statin-drug interactions between this study and another study is showed in Figure 4.
Concurrent use of statin and other medications may increase or decrease the effectiveness of some medications. Also, increases statin toxicity such as myopathy, rhabdomyolysis, and renal failure. The use of statin in conjunction with clopidogrel, clarithromycin, amiodarone, and colchicine may cause myopathy and rhabdomyolysis. Therefore, carefully monitor for signs of muscle pain or weakness with concomitant therapy.
In this study, statin agents were prescribed with clopidogrel in 17 (23.61 %) of 55 prescriptions. statins may impair clopidogrel’s antiplatelet action. The postulated mechanism for this potential interaction was that the CYP3A4 substrate atorvastatin or other statins inhibited clopidogrel metabolism to its active metabolite via CYP3A4. In a study of 44 patients undergoing stent placement who were receiving clopidogrel alone or in combination with atorvastatin or pravastatin, concurrent atorvastatin treatment reduced platelet inhibition in a dose-dependent manner (% platelet aggregation=34%, 58%, 74%, and 89 % with atorvastatin doses of zero, 10mg, 20mg, and 40mg, respectively) [30].
According to the medical advice for amiodarone, lower starting and maintenance dosages of CYP3A4 substrates, such as atorvastatin, may be required because amiodarone enhances exposure to these medications. A case report details a 55-year-old patient who began on high-dose atorvastatin (80 mg daily), progressed to amiodarone loading dose (400 mg three times a day) a week later, and then progressed to high-dose ciprofloxacin six days later (750 mg twice daily). He developed rhabdomyolysis, increased urine myoglobin, and renal failure three days after receiving this triple medication and nine days after receiving atorvastatin and amiodarone combined [31].
Concurrent use of cyclosporine with a statin is contraindicated due to an increased risk of atorvastatin- related adverse events such as myopathy and rhabdomyolysis. Instead, consider switching to a statin that is less susceptible to this interaction, such as pravastatin or Fluvastatin, or another type of LDL-lowering medicine. According to the American Heart Association, these medicines may be combined if the atorvastatin dose is limited to no more than 10 mg daily and patients are closely monitored for signs or symptoms of muscle-related toxicity [32]. This interaction is presumably the result of both cyclosporine inhibition of statin’s CYP3A4 metabolism and cyclosporine impairment of statin’s hepatic absorption via the OATP1B1/SLCO1B1 pathway. According to published case studies, patients treated with atorvastatin suffered rhabdomyolysis after initiating or increasing the dose of cyclosporine [33, 34].
The majority of atorvastatin medication interactions may be avoided by adhering to best practices in clinical care and clinical pharmacology, such as avoiding complicated treatment regimens, utilizing a single pharmacy for all prescriptions, and recognizing patient risk factors.
This study showed that statin-drug interactions were mostly observed among those whose age was between 66 and 70 years old. Because nearly at this age and older a patient usually has several chronic diseases especially CVD
and diabetes mellitus both of which require statin therapy as prevention from further worsening or other CVD.
This study revealed that most of the statin-drug interactions 57.5% were on a pharmacokinetic basis and around 40% were on a pharmacodynamics basis while the other 2.5% of the interactions were with unknown/unclear mechanisms.
Conclusion and Recommendations
Around 27% of patients have had clinically significant statin-drug interactions. The majority of those interactions were in category C followed by category D. Most statin- drug interactions were on a pharmacokinetic basis. Factors that contribute to Statin-drug interactions were; advanced age, increased number of concomitant medications, and comorbidities. According to the results obtained in this study, we recommend:
- Adhering to best practices in clinical care and clinical pharmacology, such as avoiding complicated treatment regimens, utilizing a single pharmacy for all prescriptions, and recognizing patient risk factors.
- In addition, health care professionals should use drug- drug interaction checkers such as Lexicomp, Medscape, and Micromedex and a book such as the Handbook of Drug Interactions.
- More studies should be done on all departments of Yemen’s hospitals.
- Physicians should be aware and give more attention during prescribing medications.
- Clinical pharmacists should be present in all branches of the hospital to correct any errors.
- A distance should be placed between the administrations of drugs to reduce drug interactions.
- Statin doses should be reduced.
- The combination is acceptable to use if clinically indicated, rosuvastatin and fenofibrate (or fenofibric acid) are not an option.
- Closer monitoring for muscle-related toxicity is recommended when used in combination.
- Using alternatives to statin medications, if necessary and possible, to avoid their adverse effects.
References
-
Kinirons MT, Crome P (1997) Clinical Pharmacokinetic Considerations in the Elderly. Clin Pharmacokinet 33(4): 302-312.
-
Collins R, Reith C, Emberson J, Armitage J, Baigent C, et al. (2016) Interpretation of the Evidence for the Efficacy and Safety of Statin Therapy. Lancet 388(10059): 2532- 2561.
-
Wynne HA, Blagburn J (2010) Drug Treatment in an Ageing Population: Practical Implications. Maturitas 66(3): 246-250.
-
Maher RL, Hanlon J, Hajjar ER (2014) Clinical Consequences of Polypharmacy in Elderly. Expert Opin Drug Saf 13(1): 57-65.
-
Einarson TR (1993) Drug-Related Hospital Admissions. Ann Pharmacother 27(7-8): 832-840.
-
Vrdoljak D, Borovac JA (2015) Medication in the Elderly- Considerations and Therapy Prescription Guidelines. Acta Med Acad 44(2): 159-168.
-
Goldberg RM, Mabee J, Chan L, Wong S (1996) Drug-Drug and Drug-Disease Interactions in the ED: Analysis of a High-Risk Population. Am J Emerg Med 14(5): 447-450.
-
McDonnell PJ, Jacobs MR (2002) Hospital Admissions Resulting from Preventable Adverse Drug Reactions. Ann Pharmacother 36(9): 1331-1336.
-
Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, et al. (2020) 2019 ESC/EAS Guidelines for the Management of Dyslipidaemias: Lipid Modification to Reduce Cardiovascular Risk. Eur Heart J 41(1): 111-188.
-
Gu Q, Paulose-Ram R, Burt VL, Kit BK (2014) Prescription Cholesterol-Lowering Medication Use in Adults Aged 40 and Over: United States, 2003-2012. NCHS Data Brief 2014(177): 1-8.
-
ABIM Foundation (2017) Cholesterol Drugs for People 75 and Older.
-
Bellosta S, Corsini A, Ferri N (2020) Risk Factors for SAMS. In: Thompson P, (Eds.), Statin-Associated Muscle Symptoms. Contemporary Cardiology. Springer pp: 51- 61.
-
Benes LB, Bassi NS, Davidson MH (2016) The Risk of Hepatotoxicity, New Onset Diabetes and Rhabdomyolysis in the Era of High-Intensity Statin Therapy: Does Statin Type Matter? Prog Cardiovasc Dis 59(2): 145-152.
-
Morgan TK, Williamson M, Pirotta M, Stewart K, Myers SP, et al. (2012) A National Census of Medicines Use: A 24-Hour Snapshot of Australians Aged 50 Years and Older. Med J Aust 196(1): 50-53.
-
Elliott RA (2006) Problems with Medication Use in the Elderly: An Australian Perspective. Geriatric Therapeutics 36(1): 58-66.
-
Doan J, Zakrzewski-Jakubiak H, Roy J, Turgeon J, Tannenbaum C (2013) Prevalence and Risk of Potential Cytochrome P450-Mediated Drug-Drug Interactions in Older Hospitalized Patients with Polypharmacy. Ann Pharmacother 47(3): 324-332.
-
Gnjidic D, Johnell K (2013) Clinical implications from drug-drug and drug-disease interactions in older people. Clin Exp Pharmacol Physiol 40(5): 320-325.
-
Wallach-Kildemoes H, Stovring H, Holme Hansen E, Howse K, Petursson H (2016) Statin Prescribing According to Gender, Age and Indication: What About the Benefit-Risk Balance? J Eval Clin Pract 22(2): 235- 246.
-
Morgan TK, Williamson M, Pirotta M, Stewart K, Myers SP, et al. (2012) A National Census of Medicines Use: A 24-Hour Snapshot of Australians Aged 50 Years and Older. Med J Aust 196(1): 50-53.
-
Bellosta S, Corsini A (2012) Statin Drug Interactions and Related Adverse Reactions. Expert opin Drug Saf 11(6): 933-946.
-
Ho CKM, Walker SW (2012) Statins and their Interactions with Other Lipid-Modifying Medications: Safety Issues in the Elderly. Ther Adv Drug Saf 3(1): 35-46.
-
Bottorff MB (2006) Statin Safety and Drug Interactions: Clinical Implications. Am J cardiol 97(8a): 27-31.
-
Corsini A, Ceska R (2011) Drug–Drug Interactions with Statins: Will Pitavastatin Overcome the Statins’ Achilles’ heel? Curr Med Res Opin 27(8): 1551-1562.
-
Cabrera MA, Dip RM, Furlan MO, Rodrigues SL (2009) Use of Drugs That Act on the Cytochrome P450 System in the Elderly. Clinics (Sao Paulo) 64(4): 273-278.
-
Gavronski M, Volmer D, Hartikainen S, Zharkovsky A (2015) Potential drug interactions with statins: Estonian register-based study. Open Med (Wars) 10(1): 254-260.
-
Zhelyazkova-Savova M, Gancheva S, Sirakova V (2014) Potential Statin-Drug Interactions: Prevalence and Clinical Significance. Springerplus 3: 168.
-
Al-Ashwal F, Sulaiman SAS, sheikh GSM, Kubas MA, Halboup A (2022) Prevalence and Predictors of Clinically Significant Statin-Drug Interactions among Yemeni Patients Taking Statins for Primary and Secondary Prevention of Cardiovascular Diseases. Curr Med Res Opin 38(6): 889-899.
-
Dighrir I, Hammadi A, Zaeri H, Aldajany R, Alotaibi R, et al. (2021) Identify and Assess Drug Interactions with Atorvastatin in Inpatient Care.
-
Samardzic I (2017) Incidence of Statin-Drug Interactions in Croatian Community Pharmacy. Pharmazie 72(3): 187-191.
-
Lau WC, Waskell LA, Watkins PB, Neer CJ, Horowitz K, et al. (2003) Atorvastatin Reduces the Ability of Clopidogrel to Inhibit Platelet Aggregation: A New Drug- Drug Interaction. Circulation 107(1): 32-37.
-
Cowley E, Omar MA (2021) Suspected Drug-Induced Rhabdomyolysis from the Combination of Atorvastatin, Amiodarone, and Ciprofloxacin. Ann pharmacother 55(3): 415-416.
-
Wiggins BS, Saseen JJ, Page RL 2nd, Reed BN, Sneed K, et al. (2016) American Heart Association Clinical Pharmacology Committee of the Council on Clinical Cardiology; Council on Hypertension; Council on Quality of Care and Outcomes Research; and Council on Functional Genomics and Translational Biology. Recommendations for Management of Clinically Significant Drug-Drug Interactions with Statins and Select Agents Used in Patients with Cardiovascular Disease: A Scientific Statement from the American Heart Association. Circulation 134(21): e468-e495.
-
Hermann M, Asberg A, Christensen H, Holdaas H, Hartmann A, et al. (2004) Substantially Elevated Levels of Atorvastatin and Metabolites in Cyclosporine-Treated Renal Transplant Recipients. Clin Pharmacol Ther 76(4): 388-391.
-
Maltz HC, Balog DL, Cheigh JS (1999) Rhabdomyolysis Associated with Concomitant Use of Atorvastatin and Cyclosporine. Ann Pharmacother 33(11): 1176-1179.
- Gallic and Citric Acid Present in the Peels of Tropical Fruits as an Alternative in the Fight against Cancer
- Treating the Forehead Lines with Combination of Forehead and Glabellar Botulinum Toxin Among Japanese Patients
- Clinical Evaluation of Patients Suffering from Breast Cancer & Determination of Treatment Therapies and Better Strategies Related to Breast Cancer
- Medieval Recipes by Al-Zahrāwī for Heart Palpitations Treatment
- Etiology and Prescription Errors of Myocardial Infarction in Different Health Care Systems of Azad Kashmir
- Early Diagnosis and Multidisciplinary Management of Turner Syndrome: A Paediatric Case Study