Relationship of the Vitamin D Levels with Various Biochemical Parameters among the Adult Males of Chandigarh, India
Background: Vitamin D level in the body is impacted by various biochemical parameters. Age related changes mark a significant role in the regulation of these parameters. Aims and Objectives: The present study intends to assess the correlation of the vitamin D levels with various biochemical parameters among males of various age groups in Chandigarh. Materials and Methods: The sample included 332 males of the age ranging between 30 and 70 years. Vitamin D level of all the participants was estimated by employing chemiluminescence immunoassay method. For the other biochemical parameters, the standard laboratory procedures were deployed. All the subjects were divided into three categories of Vitamin D level, i.e., normal range (>30–100 ng/ml), insufficiency (21–29 ng/ml), and deficiency (0–20 ng/ml) as per the Endocrine Society Guidelines (2011). Results: The mean value of serum phosphorous was found to be higher for males in normal category as compared to the males in the vitamin D deficient and insufficient categories in all age groups. The mean value of parathyroid hormone was minimum among males in vitamin D normal category while the maximum mean value of this parameter was reported in vitamin D deficient males across all the age groups. The serum phosphorous was reported to have a positive association with the vitamin D level in normal (r=0.445**) and deficient (r=0.026) category. Serum calcium presented a positive and significant correlation with the normal vitamin D level (r=0.348**). Parathyroid hormone exhibited a negative and significant correlation with normal vitamin D level (r=-0.792**). Serum creatinine exhibited a negative and significant correlation (r= -0.447**) with the normal vitamin D level in males. The serum alkaline phosphatase displayed a negative and significant association with the vitamin D level in normal category (r=-0.616**) and a positively significant association with vitamin D deficient males (r = 0.285**). Conclusion: Serum phosphorous and serum calcium were found to be positively and significantly associated with the vitamin D level among males whereas parathyroid hormone and serum alkaline phosphatase were reported to be negatively and significantly associated with the vitamin D level overall.
Abbreviations
VDRs: Vitamin D receptors; CLIA: Chemiluminescence immunoassay; UV: Ultra Violet; DEA: Diethanolamine; DGKC: Deutsche Gesellschaft Fur Klinische Chemie; ANOVA: Analysis of Variance; VDD: Vitamin D deficient; VDI: Vitamin D insufficient.
Introduction
Vitamin D can be synthesized endogenously after the exposure of skin to the sunlight, a major proportion of the required Vitamin D is obtained through this process [1]. It is required for the maintenance of optimum blood levels of calcium and phosphate that are required for normal mineralization of bone, muscle contraction, nerve conduction, and general cellular function in all cells of the body. It is also reported to be significant for immune function, for inflammation, cell proliferation, and differentiation [1, 2]. Ergocalciferol (vitamin D2) and cholecalciferol (vitamin D3) are the two supplemental forms of vitamin D which are officially designated as equivalent and interchangeable by Pharmacopoeias [3].
The active form of Vitamin D initiates the absorption of calcium in the duodenum and enhances the calcium influx in distal tubules of kidney through nuclear Vitamin D receptor (VDR); latter is specifically regulated by parathormone level [4]. Vitamin D has a significant role in the maintenance of health , due to the presence of its highly specific receptors, VDRs (vitamin D receptors) in all tissues of the body. It also contributes a regulatory role in the encoding of more than 200 genes [5]. The serum level of vitamin D is regulated by several factors. Alkaline phosphatase consists of group of identical enzymes that are native to four homologous alkaline phosphatase genes [6]. Tissue specific enzymes are coded by three out of four genes while the remaining one is present in many body tissues like bone, kidneys and liver. In an adult who possesses normal hepatic function, liver and bone contribute equally to the total serum pool of alkaline phosphatases whereas in case of children and pubertal age groups, bone specific isoenzyme are reported in abundant form due to rapidly growing bones [7]. As raised level of serum alkaline phosphatase signifies the state of increased bone turnover hence it is used as a bone formation marker [8]. According to a study conducted on the adult population of Chandigarh, the overall vitamin D deficiency among the adult males of Chandigarh was found to be 28.5% [9].
Material and Methods
The present study was conducted with the objective to assess the correlation of the Vitamin D levels with the other biochemical parameters among the adult males of Chandigarh, India, which is the capital of states named Punjab and Haryana. In the present cross‑sectional study, a random sampling procedure was adopted to select 332 males with age ranging between 30 and 70 years. Before initiating data collection, all the participants were informed about the nature as well as purpose of the study, and their verbal informed consent was also obtained. Union territory of Chandigarh comprised the city of Chandigarh and a number of adjoining villages, but the data were not collected from the rural areas. The data were collected from different sectors of Chandigarh city. Data collection was carried out from December 2017 to March 2019 from various parts of union territory of Chandigarh. Background information of all the participants regarding their age, education, occupation, and diet was collected using a detailed questionnaire. Informed consent was taken from each participant, and ethical clearance for conducting the study was obtained from the institutional ethical committee.
Exclusion criteria: Participants having any chronic liver disease, long illness, history of medication with corticosteroids, hormone replacement therapy, and any record/history of surgery were excluded from the study.
Laboratory Methods
The estimation of the serum levels of the vitamin D, phosphorous, calcium, parathyroid hormone, creatinine and alkaline phosphatase were done through standard laboratory procedures.
Estimation of Serum Vitamin D level: For the estimation of the serum levels of Vitamin D of the participants, chemiluminescence immunoassay (CLIA) method was adopted. Blood samples were collected by a phlebotomist. The samples were transported to the laboratory in cool packs and were stored at −20°C. Serum 25 (OH) Vitamin D level was estimated by CLIA technique (Beckman dxi 600) in the laboratory. Vitamin D level was stratified into three categories, i.e., normal range (>30–100 ng/ml), Vitamin D insufficiency (21–29 ng/ml), and Vitamin D deficiency (0–20 ng/ml) [10].
Estimation of Serum Phosphorous: Estimation of serum phosphorus is done by Serum phosphomolybdate analysis with spectrophotometry. Serum phosphorus level was determined by molybdate UV method with the help of Liquimax Phosphorus-SLR kit (Avecon Healthcare Pvt. Ltd.). The optical density of the test serum (10 µl) was read against the blank and standard samples at 340nm wavelength using UV Spectrophotometer in this method. Normal serum phosphorus values in this method ranged from 2.4 to 5.0 mg/dL.
Estimation of Serum Calcium: Modified O-cresolphthalein Complexone method was used for the estimation of the serum level of the calcium. Erba Mannheim calcium estimation kit was used. The normal values of calcium with this kit ranged from 8.4 to 10.4 mg/dL.
Estimation of Parathyroid Hormone: This was gauged as per specific chemiluminescence immunoassays with range value of 16-87 pg/ml.
Estimation of Serum Creatinine: Serum Creatinine was estimated by deploying the Jaffe’s method of which the normal value ranged from 0.7-1.2 mg/dL.
Estimation of serum alkaline phosphatase: This was done quantitatively by DEA buffer/DGKC method using Liquimax alkaline phosphatase from Avecon Healthcare Pvt. Ltd. Change in the optical density of 20µl of test serum was read against distilled water at 405nm. Normal value of alkaline phosphatase ranges from 80-315(U/L).
Statistical analysis
The collected data were analysed by employing Statistical Package for Social Sciences (SPSS) version 21.0 (SPSS Inc.). The one way analysis of variance(ANOVA) was deployed for calculating the difference among the categorical variables. Karl Pearson coefficient of correlation was used to assess the association of the vitamin D levels with the various biochemical parameters. The level of significance for all analysis was set at P < 0 ∙ 05 and a confidence interval of 95%.
Results
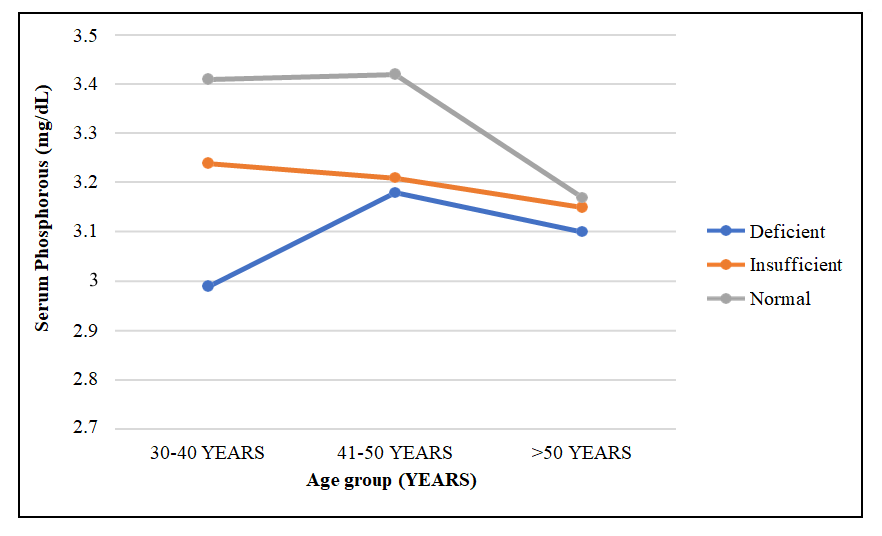
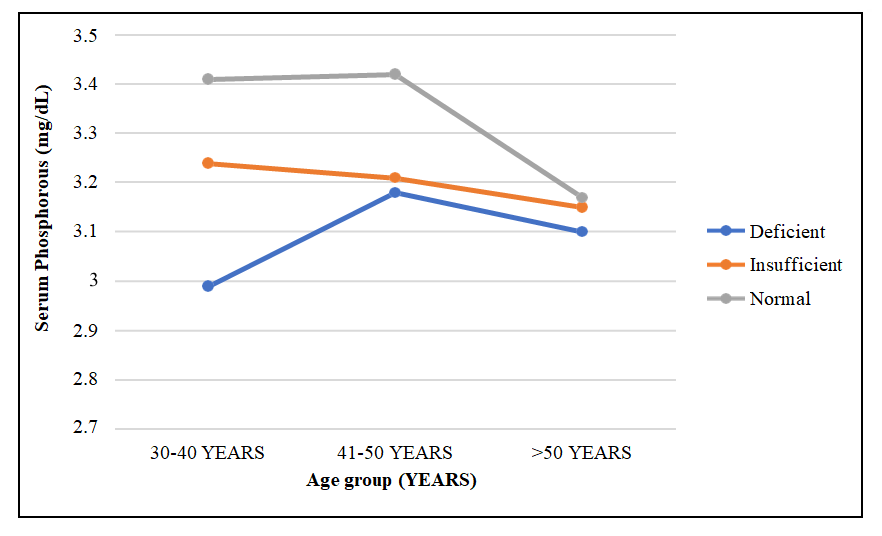
Age group wise descriptive statistics of biochemical parameters of males in three different categories of Vitamin D level have been summarized in the Table 1. The mean value of Serum Phosphorous was found to be higher for males in normal category as compared to the males in the vitamin D deficient and insufficient categories in all age groups under consideration (Table 1). In vitamin D deficient (VDD) category the mean value was found to be highest in the age group 41-50 (3.18 mg/dL), where after the mean value of the serum phosphorous exhibited a slightly decrement in the age group >50(3.1 mg/dL). In the insufficient category (VDI) the mean value of serum phosphorous was found to be highest in the age group 30-40(3.24 mg/dL) followed by an age related decline in the mean value. In the normal category of the vitamin D the highest mean value was observed in the age group of 41-50(3.42 mg/dL), thereafter a decline in the mean value was noticed in the age group>50(3.17mg/dL). F values displayed statistically significant difference in all the categories of Vitamin D in age groups 30-40 (F=16.93) and 41-50 (F=5.812) only, while in >50 years (0.506) non- significant value was noted (Figure 1).
The serum calcium levels across three different categories of Vitamin D showed a different pattern. The overall mean value of the serum calcium level was found to be higher in the normal category of vitamin D as compared to the males in the vitamin D insufficient category across all the age groups (Figure 2). In vitamin D deficient category of males, the lowest mean value was found in the age group 41- 50(8.51 mg/dL), while the highest mean value was observed for the age group 30-40 (9.54 mg/dL). Among males in the insufficient category (VDI), the highest mean value was recorded for the age group 41-50 (9.0 mg/dL), while the lowest was recorded in the oldest age group (8.74 mg/dL). In the normal category, the highest mean value was recorded for the age group 41-50 (9.25 mg/dL) and the lowest was recorded for the age group >50. The results of one-way analysis of variance in different categories of Vitamin D level depicted significant difference in age groups 30-40 (F=21.27) and 41-50 (F=92.65) only.
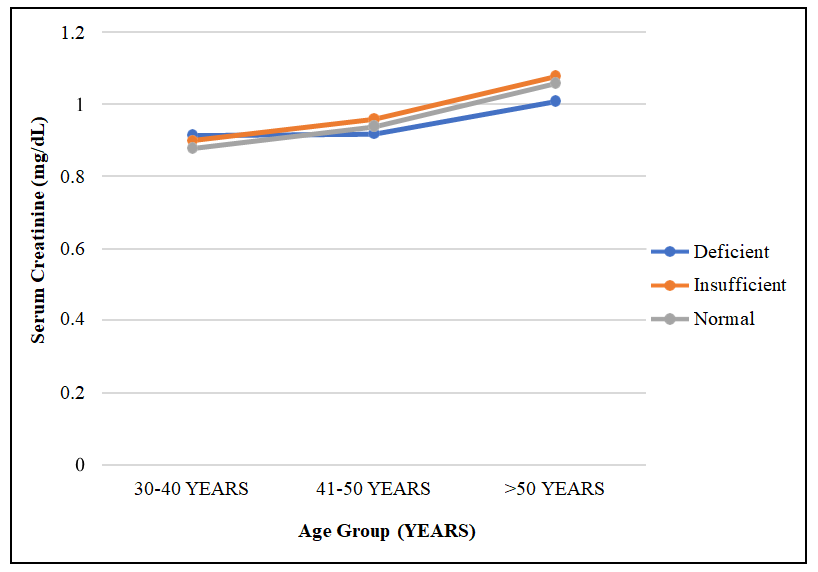
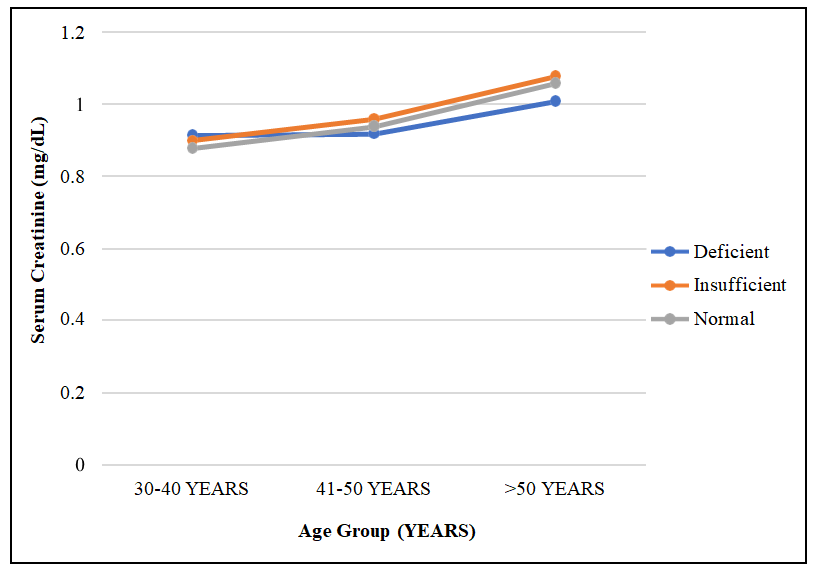
The mean value of parathyroid hormone was minimum among males in vitamin D normal category while the maximum mean value of this parameter was reported in VDD males across all the age groups (Figure 3). In the vitamin D deficient group highest mean value was noted in the age group >50 (77.56 pg/ml), while in vitamin D insufficient category highest mean value was observed in 30-40 years (48.49 pg/ml). The results of one-way analysis of variance (ANOVA) in different categories of Vitamin D level displayed significant difference across all age groups as depicted from the F-values of various age groups 30-40 (466.16), 41-50 (30.517) and >50 (219.479**). The mean value of serum creatinine was highest for the males in the age group >50 for all the categories of vitamin D levels as shown in Table 1. The participants in all the three categories of Vitamin D level revealed an age associated increment in their mean values of this variable (Figure 4). In VDD males the mean value of serum creatinine was found to be highest in the age group of >50 (1.01 mg/dL) whereas the lowest was noted in the age group 30-40 (0.91 mg/dL). In the insufficient (1.08mg/dL) and normal (1.06mg/dL) category the mean value of serum creatinine was highest in the age group >50. The results of one-way analysis of variance in three different categories of Vitamin D level displayed significant difference only in age level >50 ( F-value=4.284*), while for 30-40 years (F value =1.690) and 41-50 years (F value =1.760) differences were statistically non-significant.
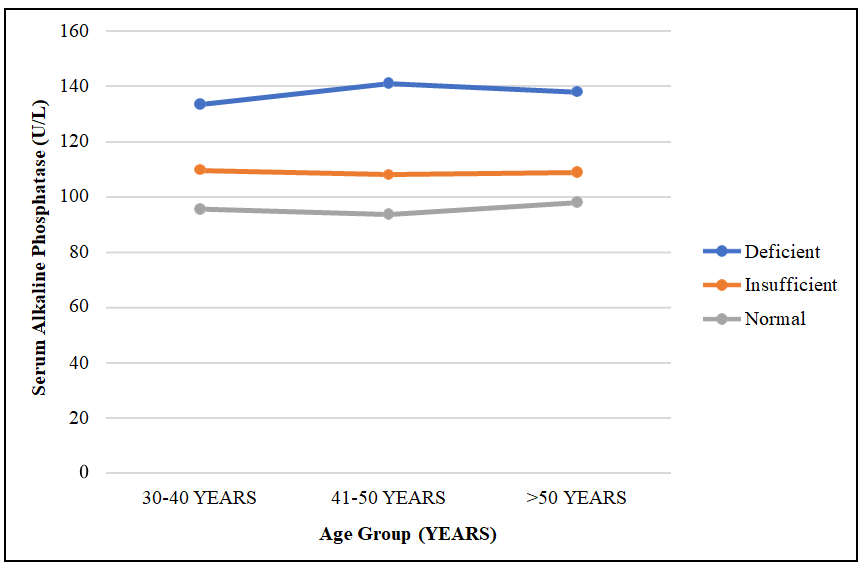
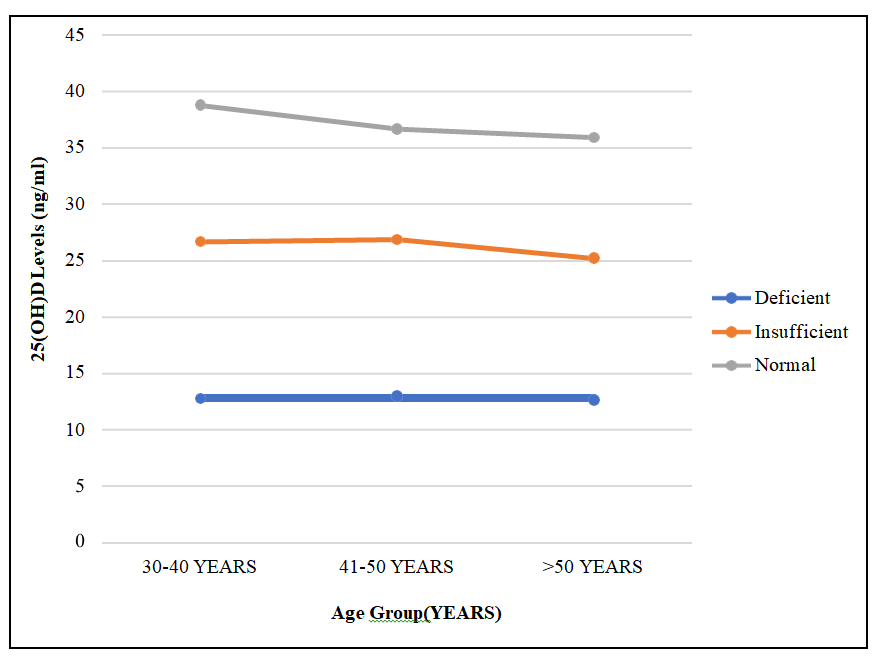
In male serum alkaline phosphatase demonstrated highest mean values in vitamin D deficient category as compared to their counterparts in vitamin D insufficient and normal category (Figure 5). In vitamin D deficient group, the mean value of this variable at 30-40 years was 133.54 U/L which increased to 141.24 U/L at 41-50 years followed by a decline in the mean value at >50 years (Table 1). Whereas in males with normal vitamin D level, lowest mean value was noted in the age group 41-50 (93.67U/L), thereafter an increment in the mean value was observed. In VDI participants, it was observed that age group 30-40 had the highest mean value of serum alkaline phosphatase. The outcome of one- way analysis of variance in different categories of Vitamin D level demonstrated significant difference in all age groups as portrayed from the F values 30-40 years (167.935) , 41-50 years (276.463) and >50 years (118.556). In males, the mean value of 25(OH) Vitamin D was found to be highest in the normal category of Vitamin D level in all age groups as compared to their counterparts in VDI as well as VDD category as shown in Figure 6. In both the VDD and VDI category, participants of age group 41- 50 had the highest mean value of 25(OH) vitamin D, while the lowest value of this parameter was noted at >50 years. Males with normal category of vitamin D exhibited highest mean value at 30- 40 years (38.82 ng/ml) followed by a decline in the mean values at successive age levels (Table 1). The results of one-way analysis of variance in different categories of Vitamin D level displayed significant difference across all age groups as depicted from the F-values of various age groups 30-40 (234.84), 41-50 years (293.486) and >50 years (190.403).
The Karl Pearson correlation coefficient (r) of the vitamin D levels with different biochemical parameters in males is presented in Table 2. The serum phosphorous was reported to have a positive association with the vitamin D level in normal (r=0.445) and deficient (r=0.026) category, but the association was found to be significant only in normal vitamin D level. Serum calcium presented a positive and significant correlation with the normal vitamin D level (r=0.348), but in the deficient category of vitamin D association was negative (r=-0.130) and non-significant. Parathyroid hormone exhibited a negative and significant correlation with normal vitamin D level (r=-0.792) and VDD category (r=-0.460), Serum creatinine exhibited a negative and significant correlation (r= -0.447) with the normal vitamin D level in males, while a positive and significant correlation was observed in vitamin D deficient males (r=0.322). The serum alkaline phosphatase also showed similar trend, where a negative and significant association was seen with the vitamin D level in normal category (r=-0.616) and a positive as well as significant association with VDD males (r = 0.285).
| Biochemical Variables | Age Group (30-40) (n =101) 1 | Age Group (41-50) (n =113) 2 | Age Group (>50) (n =118) 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean±S.D | F-value | p- value | Mean±S.D | F-value | p- value | Mean±S.D | F-value | p- value | ||
| Serum Phosphorous (mg/dL) | Deficient | 2.99±0.35 | 16.93 | 0.000 | 3.18±0.23 | 5.812 | 0.004 | 3.1±0.343 | 0.506 | 0.604 |
| Insufficient | 3.24±0.291 | 3.21±0.366 | 3.15±0.225 | |||||||
| Normal | 3.41±0.306 | 3.42±0.399 | 3.17±0.314 | |||||||
| Serum Calcium (mg/ dL) | Deficient | 9.54±0.55 | 21.27 | 0.000 | 8.51±0.27 | 92.65 | 0.000 | 8.63±0.442 | 2.176 | 0.118 |
| Insufficient | 8.96±0.296 | 9±0.29 | 8.74±0.174 | |||||||
| Normal | 9.1±0.17 | 9.25±0.139 | 8.77±0.254 | |||||||
| Parathyroid Hormone (pg/ml) | Deficient | 67.98±6.66 | 466.16 | 0.000 | 66.86±33.47 | 30.517 | 0.000 | 77.56±14.1 | 219.479 | 0.000 |
| Insufficient | 48.49±3.21 | 43.15±2.77 | 47.04±2.02 | |||||||
| Normal | 33.69±4.14 | 35.5±2.32 | 37.45±1.83 | |||||||
| Serum Creatinine (mg/dL) | Deficient | 0.916±0.09 | 1.690 | 0.19 | 0.92±0.118 | 1.760 | 0.177 | 1.01±0.16 | 4.284 | 0.016 |
| Insufficient | 0.9±0.08 | 0.96±0.102 | 1.08±0.08 | |||||||
| Normal | 0.88±0.08 | 0.94±0.065 | 1.06±0.06 | |||||||
| Serum Alkaline Phosphatase (U/L) | Deficient | 133.54±13.36 | 167.935 | 0.000 | 141.24±11.67 | 276.463 | 0.000 | 138.1±4.83 | 118.556 | 0.000 |
| Insufficient | 109.84±7.07 | 108.09±8.02 | 109.02±12.31 | |||||||
| Normal | 95.68±5.87 | 93.67±6.97 | 98.05±4.9 | |||||||
| 25(OH) Vitamin D (ng/mL) | Deficient | 12.78±3.7 | 234.484 | 0.000 | 12.99±4.68 | 293.486 | 0.000 | 12.67±5.09 | 190.403 | 0.000 |
| Insufficient | 26.68±2.88 | 26.89±2.79 | 25.26±2.79 | |||||||
| Normal | 38.82±6.63 | 36.68±4.75 | 35.92±6.2 |
Table 1: Age group wise descriptive statistics of biochemical parameters of males in three different categories of Vitamin D leve
Level of significance p<.05*, p<.01 , p<.001 Table 1: Age group wise descriptive statistics of biochemical parameters of males in three different categories of Vitamin D level.
| Biochemical Parameters | Vitamin D Normal | Vitamin D Deficient | TOTAL | |||
|---|---|---|---|---|---|---|
| r | p-value | r | p-value | r | p-value | |
| Serum Phosphorous (mg/dL) | 0.445** | 0.000 | 0.026 | 0.805 | 0.411** | 0.0001 |
| Serum Calcium (mg/dL) | 0.348** | 0.000 | -0.13 | 0.21 | 0.155** | 0.005 |
| Parathyroid Hormone (pg/ml) | -0.792** | 0.000 | -0.460** | 0.0001 | -0.771** | 0.0001 |
| Serum Creatinine (mg/dL) | -0.447** | 0.000 | 0.322** | 0.001 | -0.091 | 0.096 |
| Serum Alkaline Phosphatase (U/L) | -0.616** | 0.000 | 0.285** | 0.005 | -0.836** | 0.000 |
Table 2: Karl Pearson correlation coefficient (r) of the Vitamin D levels with the different Biochemical parameters of the males.
Level of significance p<.05*, p<.01 , p<.001 Table 2: Karl Pearson correlation coefficient (r) of the Vitamin D levels with the different Biochemical parameters of the males.
Serum phosphorous and serum calcium were found to be positively and significantly associated with the vitamin D level among males whereas parathyroid hormone and serum alkaline phosphatase were reported to be negatively and significantly associated with the vitamin D level overall.
Discussion
In the present study, the mean value of the serum phosphorous was found to be higher in the normal category of the vitamin D than the deficient category across all age groups in the males. The serum phosphorous was found to be positively and significantly correlated with the vitamin D level (p<0.01). A study carried out on the population of Istanbul by Caykara et al. reported that there was a positive association between serum phosphorous level and vitamin D [11]. In divergence to the present findings, Al-Daghri et al. reported an inverse and significant correlation between the vitamin D and serum phosphorus on the adult population (males=373) of Saudi Arabia [12]. Kanani, et al. illustrated that the serum phosphorous exhibited a negative correlation with the vitamin D level in the males [13].
In the present study serum calcium revealed higher mean values in the normal category than the Vitamin D deficient category (VDD) in the males across all the age groups except for 30-40 years in males. This variable demonstrated a positive and significant correlation with the vitamin D levels among males. Similarly the findings of Kanani et al. on the subjects from Karachi revealed a positive association with the vitamin D level in the males [13]. A study of Caykara et al. on the population (males=298) of Istanbul also reported that there was a significant positive association between serum calcium level and vitamin D level [11].
In the present study, the mean value of the parathyroid hormone was found to be lower in the males with normal vitamin D level as compared to the VDD males across all the age groups. Likewise in the Brazilian population Martins et al. reported a negative and significant correlation vitamin D level with parathyroid hormone [14]. A negative and significant association of the parathyroid hormone was reported with the vitamin D level in several prior studies [12, 15, 16]. A recent study performed in Karachi also reported that parathyroid hormone was negatively correlated with the vitamin D level [13].
In the current cross-sectional study, mean value of the serum alkaline phosphatase was found to be higher in the vitamin D deficient category as compared to the normal category across all the age groups. Serum alkaline phosphatase level was negatively and significantly correlated with Vitamin D status in males. The observations of present study were not in coherence with the study conducted in Karachi. They reported non-significant and positive correlation of serum alkaline phosphatase with vitamin D level [17]. It was illustrated by Holick, that Vitamin D increases 30%- 40% efficiency of intestinal uptake of calcium and about 80% of phosphorus absorption [5]. Vitamin D deficiency results in secondary hyperparathyroidism which leads to loss of phosphorus in the urine and decreases intestinal uptake of phosphorus thereby causing diminished phosphorus concentration. Lower calcium and phosphorus levels may be responsible for defective mineralization which leads to rickets in children and osteomalacia in adults [1, 18, 19].
Conclusion
The result of the study showed that there was a gradual decrease in the level of the serum phosphorous with the advancement in the age among the males who were suffering from the vitamin D insufficiency. The mean value of serum calcium was found to be highest for the age group of 41–50 years for the vitamin D insufficient and vitamin D normal categories of males in comparison to the other age groups. The mean value of the parathyroid hormone was found to be highest for the vitamin D deficient males across all the age groups. The mean value of the serum creatinine was observed to be highest for the oldest age group for all the three categories of the vitamin D levels. The vitamin D normal males were found to have lowest level of the serum alkaline phosphatase across all the age groups. Serum phosphorous and serum calcium were found to be positively and significantly associated with the vitamin D level among males whereas parathyroid hormone and serum alkaline phosphatase were reported to be negatively and significantly associated with the vitamin D level.
Acknowledgment
I thank the UGC-CAS II Department of Anthropology, Panjab University, and New Delhi, for funding.
Financial Support and Sponsorship
The study was supported by the University Grants Commission, New Delhi, India, (research vide letter no. 854 /[NET DEC.2014]).
Conflicts of Interest
There are no conflicts of interest.
References
-
Holick MF (2003) Vitamin D: A millenium perspective. Journal of cellular biochemistry 88(2): 296-307.
-
Kumar V, Abbas AK, Aster JC (2013) Robbins basic pathology. 9th (Edn.), Elsevier Health Sciences, Amsterdam, Netherlands, pp: 922.
-
Houghton LA, Vieth R (2006) The case against ergocalciferol (vitamin D2) as a vitamin supplement. The American journal of clinical nutrition 84(4): 694- 697.
-
Holick MF (2005) The vitamin D epidemic and its health consequences. The Journal of nutrition 135(11): 2739S-2748S.
-
Hоlick МF (2007) Vitamin D deficiency. N Еngl J Med 357(3): 266-281.
-
Henthorn P, Millan JL, Leboy P (1999) Principles of Bone Biology. Academic press, San Diego, US, pp: 127-136.
-
Magnusson P, Larsson L, Magnusson M, Davie MW, Sharp CA (1999) Isoforms of bone alkaline phosphatase: characterization and origin in human trabecular and cortical bone. Journal of Bone and Mineral Research 14(11): 1926-1933.
-
Van Straalen JP, Sanders E, Prummel MF, Sanders GT (1991) Bone-alkaline phosphatase as indicator of bone formation. Clinica chimica acta 201(1-2): 27-33.
-
Dik D, Kaur M (2020) Prevalence of vitamin D deficiency and associated risk factors among adults in Chandigarh. International Journal of Advanced Medical and Health Research 7(2): 67-73.
-
Bischoff-Ferrari HA, Giovannucci E, Willett WC, Dietrich T, Dawson-Hughes B (2006) Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple health outcomes. The American journal of clinical nutrition 84(1): 18-28.
-
Caykara B, Ozturk G, Mutlu HH, Arslan E (2020) Relationship Between Vitamin D, Calcium, and Phosphorus Levels. Journal of Academic Research in Medicine 10(3): 252-257.
-
Al-Daghri NM, Yakout S, Aljohani N, Al-Saleh Y, Al-Attas OS, et al. (2020) Vitamin D Status and its correlation with Parathyroid Hormone level among population in Riyadh, Saudi Arabia. Journal of King Saud University- Science 32(3): 2016-2019.
-
Kanani FH, Zubairy M, Taimoor M (2020) Frequency and trend of vitamin D deficiency in correlation with demographic and selected biochemical parameters in Karachi, Pakistan. JPMA 70 (11): 1913-1917.
-
Martins JS, Palhares MD, Teixeira OC, Gontijo Ramos M (2017) Vitamin D status and its association with parathyroid hormone concentration in Brazilians. Journal of nutrition and metabolism: 9056470.
-
Sayed-Hassan R, Abazid N, Koudsi A, Alourfi Z (2016) Vitamin D status and parathyroid hormone levels in relation to bone mineral density in apparently healthy Syrian adults. Archives of osteoporosis 11: 18.
-
Tsugawa N, Uenishi K, Ishida H, Ozaki R, Takase T, et al. (2016) Association between vitamin D status and serum parathyroid hormone concentration and calcaneal stiffness in Japanese adolescents: sex differences in susceptibility to vitamin D deficiency. Journal of bone and mineral metabolism 34: 464-474.
-
Shaheen S, Noor SS, Barakzai Q (2012) Serum alkaline phosphatase screening for vitamin D deficiency states. J Coll Physicians Surg Pak 22(7): 424-427.
-
Holick MF (2002) Sunlight and vitamin D: both good for cardiovascular health. Journal of General Internal Medicine 17(9): 733-735.
-
Holick MF (2004) Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. The American journal of clinical nutrition 80(6): 1678S-1688S.
- Gallic and Citric Acid Present in the Peels of Tropical Fruits as an Alternative in the Fight against Cancer
- Treating the Forehead Lines with Combination of Forehead and Glabellar Botulinum Toxin Among Japanese Patients
- Clinical Evaluation of Patients Suffering from Breast Cancer & Determination of Treatment Therapies and Better Strategies Related to Breast Cancer
- Medieval Recipes by Al-Zahrāwī for Heart Palpitations Treatment
- Etiology and Prescription Errors of Myocardial Infarction in Different Health Care Systems of Azad Kashmir
- Early Diagnosis and Multidisciplinary Management of Turner Syndrome: A Paediatric Case Study