Alteration of Early-Phase Piperaquine Disposition by Concurrent Administration of Clarithromycin in Healthy Volunteers
Malaria and Helicobacter pylori infections are some of the most prevalent infectious diseases causing thousands of deaths worldwide. Concurrent infections can exacerbate co-morbidities or make worse the management of malaria. Drug-drug interactions arising from activities of CYP450 during concurrent management of the co-infections could worsen management challenges and therapeutic outcomes. Fifteen healthy volunteers were administered single oral dose of P-Alaxin© consisting piperaquine (960 mg) and dihydroartemisinin (240 mg). Following a five-month wash out period, clarithromycin (500 mg) was administered twice daily for five days. A single dose of P-Alaxin© was administered on the 3rd day. Blood samples were collected within 48 hours and analyzed for plasma levels of the administered drugs using RP-HPLC methods. The Tmax was 5.2±2.11 h vs 5.47±2.56 h and did not vary significantly p>0.05. However, Cmax and AUC0-48, of piperaquine when concurrently administered with clarithromycin increased significantly (179.41±56.35 ng/ml vs 478.99 ± 148.86 ng/ml; 37,644.56 ± 16.716.95 vs 104,098.47 ± 53.311.57 ng/ml*h respectively (p
Ademisoye AA¹, Soyinka JO²*, Igbinoba SI³, Onyeji CO⁴, Aluko AT⁵, Ademisoye AI⁶ and Adodo KA⁷
Keywords: Metabolism; Drug Interactions; Clarithromycin; Piperaquine
Introduction
Malaria is constantly ranked as a prime cause of deaths around the world and the effect of the disease is majorly found in developing countries of the world with heaviest toll reported in Africa [1]. In 2019 alone, global estimate of 229
million cases of malaria and 409,000 deaths, with 67 per cent of the death occurring in under 5 years children was reported [2]. The severity of illness is determined by intrinsic immunity of the host, the timing and efficacy of treatment as well as the species of infecting organisms. Plasmodium falciparum and Plasmodium vivax are the major species responsible for most cases of severe malaria. Poor diagnosis, co-existence with other infections and mismanagement of uncomplicated malaria can rapidly lead to the severe form if appropriate treatment is not instituted as soon as possible [3]. In immune-compromised individuals, it is not unexpected to find co-existence of infections like HIV, tuberculosis, and fungal infections resulting in increased mortality [4].
Much as malaria is widespread in developing countries, Helicobacter pyloric infection is also prevalent in these countries [5]. H. pylori is a bacterium that can cause stomach and other gastrointestinal ulcers affecting over fifty percent of the population of the world [6]. The infection could begin from childhood and may remain asymptomatic till adulthood [7]. The mode of transmission is unclear, but it could be through fecal-oral, or oral-oral route. Factors such as socioeconomics, poor drinking water, overcrowding, personal and environmental hygiene have been known to control transmission of H. pylori [8]. Globally, H. pylori infection shows marked geographical variation in prevalence, ranging from 24·4% in Oceania to 70·1% in Africa, high values were in low-income and middle-income countries than in high-income countries [9]. For example, in sub Saharan Ethiopia, prevalence ranged between 69 and 81 percent depending on the sophistication of the diagnostic methods while in Nigeria and Ghana, researchers reported a high prevalence rates of 73.0 percent and 94.5 percent, respectively, among patients with dyspepsia [10, 11, 12]. Also in the city of Kano in Nigeria, H. pylori infections are common among low socioeconomic group characterized by unsafe drinking water, overcrowding, and cigarette smoking [13]. Common presenting symptoms of H. Pylori infection include: dyspepsia, vomiting, diarrhea, abdominal pain and subacute intestinal obstruction which incidentally are common complaints in malaria [14]. Concurrent infection of plasmodium and H. pylori is grossly underreported, yet malaria and stomach ulcers remain a major health problem in Africa [15]. There are reports of complaints of epigastric pain in ongoing malaria infection, necessitating self or prescribed medications for both malaria and gastritis [16]. Generally, there is paucity of data on association of malaria and H. pylori. One study however reported a prevalence of malaria and H. pylori co-infection amongst age groups, gender and educational level with significant prevalence of 26.55%, 21.9% and 9.9% respectively (p ˂0.05) [17]. Clarithromycin amongst other antibiotics is frequently prescribed in seven- day triple therapies with a proton pump inhibitor, and metronidazole for effective eradication of H. pylori [18].
Notable among the medications approved for the management of plasmodiasis are artemisinin- based combination therapy (ACT) which involves a combination of artemisinin or its derivative (e.g. artesunate, arthemether, dihydroartemisinin) with a long-acting antimalarial drug such as amodiaquine, piperaquine and lumefantrine. Piperaquine is prominently used when co-formulated with dihydroarteisinin. It is therefore likely that both piperaquine and clarithromycin can be co-administered in the treatment of malaria patients with H. pylori co-infection. Piperaquine and clarithromycin are substrate and inhibitor of CYP3A4 isozyme, respectively [19]. CYP3A4 is mainly localized in the endoplasmic reticulum of cells and is responsible for the metabolism of almost half of the drugs currently in use today [20]. The gene is located on chromosome7q21.1 [21]. Some drugs that are CYP3A4 substrates are also substrates, inhibitors, or inducers of the ABC transport protein known as P-glycoprotein. Thus, many observed drug interactions involve additive effects of modulations through both CYP3A4 and P-glycoprotein. For instance, enhanced bioavailability of tamoxifen by curcumin was due to inhibition of the CYP3A4-mediated metabolism of tamoxifen as well as inhibition of the P-gp efflux transporter and reduction of the first-pass metabolism of tamoxifen [22]. Piperaquine pharmacokinetics is characterized by slow absorption and its bioavailability is difficult to measure discreetly due to the complicated absorption process. It exhibits multiple plasma concentration peaks [23].
Piperaquine has been reported to be metabolized by CYP3A4 into two major metabolites, N-oxide (M1) and N, N dioxide (M2) as depicted in Figure 1. Two additional metabolites of piperaquine, M3 an M4 were confirmed using liquid chromatography tandem high-resolution LTQ-Orbitrap mass spectrometry (HRMS) and two other metabolites M5 and M6 generated via N-dealkylation pathways in human and rat [24]. Piperaquine exhibit multiple peak concentration with extremely long elimination half-life (∼30 days) , and presumed to accumulates more in females to a degree of 30-50% more than in males [25]. This may be attributed to reports from N-oxidation and reduction retro-conversion of piperaquine and its main metabolite N-Oxide (M1) [26]. While CYP 3A4 is responsible for forward metabolism to MI metabolite, flavin containing monooxygenases was also reported to modulate the conversion of M1 to piperaquine which have also been reported to be induced by female’s hormones [27]. On the other hand Clarithromycin, an analogue of erythromycin that inhibits CYP3A4 was also reported to inhibit liver- specific organic anion–transporting polypeptides [28] and intestinal activity of CYP3A4 [29]. The aim of this study was to determine the effect of clarithromycin co-administration on the early-phase disposition of piperaquine in healthy volunteers’ optimization of concurrent infectious diseases therapy.
![Figure 1: Two additional metabolites of piperaquine, M3 an M4 were confirmed using liquid chromatography tandem high-resolution LTQ-Orbitrap mass spectrometry (HRMS) and two other metabolites M5 and M6 generated via N-dealkylation pathways in human and rat [24]. Piperaquine exhibit multiple peak concentration with extremely long elimination half-life (∼30 days) , and presumed to accumulates more in females to a degree of 30-50% more than in males [25]. This may be attributed to reports from N-oxidation and reduction retro-conversion of piperaquine and its main metabolite N-Oxide (M1) [26]. While CYP 3A4 is responsible for forward metabolism to MI metabolite, flavin containing monooxygenases was also reported to modulate the conversion of M1 to piperaquine which have also been reported to be induced by female’s hormones [27]. On the other hand Clarithromycin, an analogue of erythromycin that inhibits CYP3A4 was also reported to inhibit liver- specific organic anion–transporting polypeptides [28] and intestinal activity of CYP3A4 [29]. The aim of this study was to determine the effect of clarithromycin co-administration on the early-phase disposition of piperaquine in healthy volunteers’ optimization of concurrent infectious diseases therapy.](/fulltextimages/13489/fig_1.png)
Materials and Method
Materials
Pure samples of piperaquine and the internal standard hydroxylchloroquine were obtained from AK Scientific Inc., San Francisco, CA, USA. HPLC-grade methanol (Fisher Chemicals UK and acetonitrile (Honeywell Research Chemical Germany) were used in the preparation of HPLC mobile phase Hydrochloric acid (Sigma-Aldrich, UK), Analytical grade diethyl ether (Fisher Scientific. UK), heptane and trichloroacetic acid (Lobal Chemie, Mumbai, India) were also obtained. Clarithromycin tablets and piperaquine/ dihyroartemisinin (P-Alaxin) were purchased from a registered Pharmacy in Nigeria.
Drug Administration
Fifteen (15) healthy volunteers were recruited after fulfilling the inclusion criteria of nonsmoking, consent to participate in the study, not on any form of medication and of Nigerian descent and the exclusion criteria included pregnancy, breastfeeding, evidence of gastrointestinal, cardiovascular and neurological disorders as well as not complying with blood sampling protocols. Ethical approval for the study was obtained from Institute of Public Health, Obafemi Awolowo University (OAU), Ile-Ife, Nigeria. The healthy volunteers were administered single doses of three tablets of P-Alaxin each tablet consisting of piperaquine phosphate (320 mg) and dihydroartemisinin (80 mg) with meal. Blood samples were collected at pre-determined time intervals of 0, 1, 2, 4, 6, 8, 12, 24, 48, hours following the drug administration. The blood samples were centrifuged at 2000g for 15 min to obtain plasma which were stored at -20oC until drug analysis. After five months of wash out period, 500 mg clarithromycin was administered twice daily to each volunteer for five days. On the third day, a single dose of 3 tablets of P-Alaxineach tablet consisting piperaquine (320 mg) and dihydroartemisinin (80 mg) was administered with a meal and venous blood samples were collected at the same time points as was done in the case of administration of piperaquine alone. Plasma samples were stored at -200C until analysis.
Drug Analysis and Extraction Procedure
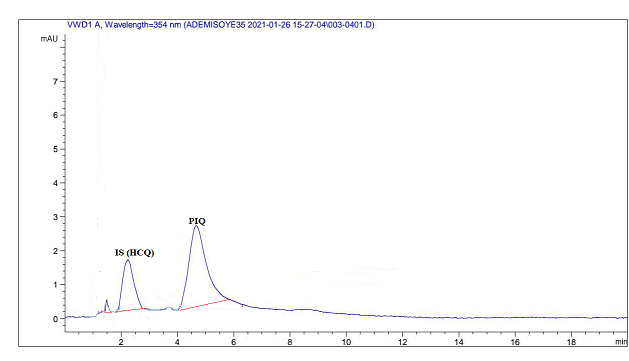
The HPLC-UV method reported by Choemang and Na-Bangchang [30] was adapted for the analysis of test compound. The method was validated for accuracy, precision, recovery and reproducibility. To 150µl of plasma in a 10 ml extraction tube, 35 ul of 1 mg/ml of internal standard hydroxychloroquine was added. After thorough vortex mixing for 5 mins, 500u1 of 0.2M hydrochloric acid (HCl) was added. The sample was mixed thoroughly and allowed to stay for 2 min at room temperature. 1 ml (1M NaOH) and 5ml of a mixture of hexane and diethyl ether (1:1) v/v were added and gently mixed for 30 min. The organic layer was separated through centrifugation at 3000 g for 5 min and transferred into a polypropylene tube and evaporated to dryness under a stream of warm air. The residue was reconstituted with 1ml of mobile phase and 200 ul injected into the column. The precision of the method was validated for intraday and inter studies for concentrations of 25 ng/ml, 100 ng/ml and 500 ng/ml while 100 ng/ml concentration was used for accuracy and recovery studies. The PIQ chromatographic peak test compound was ensured to be distinct from internal standard and other similar compounds.
Data and Statistical Analyses
The early phase was within 48 hours and the peak plasma concentrations (Cmax) and the time to reach peak concentration (Tmax) were noted directly from the concentration-time profiles. The total area under the plasma concentration-time curve (AUC0-48) was determined using the linear trapezoidal rule. The parameters calculated using the pharmacokinetic program Kinetica™ Version 4.1, 2002 InnaPhase Corporation (1700 Race Street Philadelphia, PA 19103 USA). The non-parametric Wilcoxon matched pairs signed-ranked test was used to evaluate the difference between pairs of data; a p-value below 0.05 was considered significant.
Result
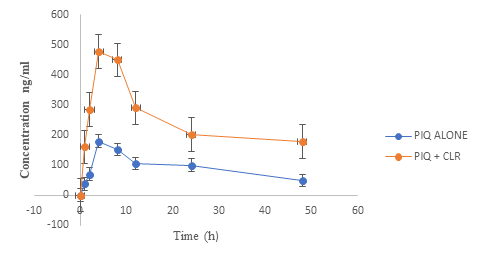
The fifteen healthy volunteers recruited comprising of twelve females and three males completed the study. Their mean age and mean weight were 26.4 ± 4.42 years and 66.65±9.96 kg respectively. The modified procedure for the analysis of the test compound was as reported by Choemag and Na-Banagchang [30], and was validated for the study. The reagents used in the extraction procedure produced a clear supernatant from the plasma. compound. The retention time of the internal standard hydroxychlroroquine was 2.5 minutes, and did not interfere with solvent front as well as the test compound which had retention time of 4.9 minutes. Figure 2 shows chromatogram of piperaquine as clearly separated from the internal standard hydroxychloroquine. The mean plasma piperaquine (PIQ) concentration with or without administration of clarithromycin (CLR) is displayed in Figure 3. The summarized PIQ pharmacokinetic parameters during administration of PIQ alone and when co- administered with CLR are displayed in Tables 1 and 2 while the statistical summary is displayed in Table 3.
| Subject | C (ng/ml) max | T (h) max | AUC( ) (ng/ml. h) 0-48h | MRT (h) |
|---|---|---|---|---|
| 1 | 354.7 | 4 | 96,810.00 | 510 |
| 2 | 174.2 | 2 | 29,929.00 | 253 |
| 3 | 204.35 | 8 | 41,714.00 | 295 |
| 4 | 166.55 | 4 | 32,949.00 | 361 |
| 5 | 159.08 | 4 | 31,245.00 | 382 |
| 6 | 167.82 | 4 | 34,177.00 | 492 |
| 7 | 153.42 | 4 | 33,396.00 | 429 |
| 8 | 253.63 | 8 | 36,113.00 | 461 |
| 9 | 153 | 8 | 32,951.00 | 225 |
| 10 | 156.93 | 8 | 26,435.00 | 288.2 |
| 11 | 147.42 | 4 | 33,679.00 | 296.63 |
| 12 | 155.6 | 4 | 33,203.00 | 268 |
| 13 | 161.03 | 4 | 37,103.00 | 291 |
| 14 | 131.69 | 4 | 33,823.45 | 425 |
| 15 | 151.68 | 8 | 31,141.00 | 357 |
| MEAN | 179.41 | 5.2 | 37,644.56 | 355.59 |
| STD | 56.35 | 2.11 | 16,716.95 | 90.87 |
Table 1: Derived pharmacokinetic parameters of piperaquine following oral administration of P-Alaxin (comprising of 960 mg pipera
| Cmax(ng/ml) | Tmax(h) | AUC(0-48h)(ng/ml. h) | MRT(h) | |
|---|---|---|---|---|
| 1 | 851.95 | 8 | 285,520.00 | 788 |
| 2 | 521.54 | 2 | 87,312.00 | 1,145.00 |
| 3 | 564.85 | 4 | 104,716 | 711 |
| 4 | 537.7 | 4 | 105,179.00 | 476 |
| 5 | 478 | 8 | 90,041 | 741 |
| 6 | 256 | 2 | 79,447.98 | 741 |
| 7 | 582 | 2 | 88,089.00 | 768 |
| 8 | 379.62 | 8 | 55,281.00 | 697 |
| 9 | 445 | 8 | 67,731.00 | 159.81 |
| 10 | 562.22 | 4 | 135,287.00 | 361 |
| 11 | 496.19 | 8 | 97,347.00 | 673 |
| 12 | 345.22 | 4 | 87,094.97 | 497.67 |
| 13 | 355.19 | 4 | 101,803.40 | 935.99 |
| 14 | 538.49 | 8 | 90,990.00 | 582 |
| 15 | 271.16 | 4 | 85,637.70 | 682.24 |
| MEAN | 478.99 | 5.47 | 104098.47 | 663.91 |
| STD | 148.86 | 2.56 | 53,311.57 | 233.42 |
| Parameters | PIQ alone | PIQ + CLR | Significance | |
| Cmax | 179.41±56.35 ng/ml | 478.99±148.86 ng/ml | P<0.05 | |
| Tmax | 5.2±2.11 h | 5.47±2.56 h | p>0.05 | |
| AUC(0-48) | 37,644.56±16,716.95 ng/ml.h | 104,098.47±53,311.57 ng/ml.h | P<0.05 |
Table 2: Derived pharmacokinetic parameters of piperaquine following oral administration of P-Alaxin (comprising of 9600 mg piper
The results of the calibration curve showed a linearity of response at concentration range of 10 ng/ml – 1000 ng/ ml for PIQ (r2 = 0.9941). The intra and inter assay precision for plasma concentration of PIQ was 8.14, 9.59 and 7.86 and 12.69, 15,65 and 8.11 at 25 ng/ml, 100 ng/ml and 500 ng/ ml respectively. Good precision was demonstrated by the coefficient of variation. The recovery of PIQ from plasma test sample was 85.17 % ±8.71. The mean Cmax for PIQ when administered alone and during concurrent dosing with CLR were 179.41 ± 56.35 ng/ml and 478.99 ± 148.86 ng/ml respectively (p<0.05). The Tmax ranged from 2 h to 8 h with mean values of 5.47 ± 2.56 h during PIQ administration alone as against 5.20 ± 2.11 h during concurrent administration with CLR. The AUC0-48 increased significantly from 37,644.56 ± 16.716.95 ng/m.h to 104,098.47 ± 53.311.57 ng/ml.h (p<0.05). The Mean Residence Time (MRT) also increased from 355.59 ± 90.87 h to 663.91 ± 233.42 h. Seven out of fifteen of the healthy volunteers recruited reported severe weakness of the body and four subjects vomited about eight hours post dose of concurrent administration of CLR and PIQ.
Discussion
Piperaquine is an officially endorsed partner drug with dihydroartemisinin in combination therapy by the World Health Organization which has become one of the most widely used antimalarial. Malaria co-infection with H. pylori is known to be common in many underdeveloped countries. [31] Clarithromycin is one of the anti-infective agents used in combination therapy of H. pylori, hence, there is a high possibility of concurrent administration of this drug with piperaquine in the treatment of patients with malaria and H. pylori co-infection. Clarithromycin is an inhibitor of CYP3A4 while piperaquine is a substrate of the same isozyme but little information is however known about the impact of clarithromycin on CYP3A4 mediated metabolism on piperaquine. The modification of the extraction procedure was easily achieved because the reagents were readily available; tert-butylmethyl ether was substituted with diethylether and the evaporation of the organic solvents was achieved with stream of warm air which makes for simplicity, cost effectiveness and robustness of the method.
The results from the study indicated that absorption of PIQ ranged between 2 to 8 h and the pharmacokinetic data derived for Cmax and AUC0-48 when PIQ was administered generally agreed with those of other workers [32, 33, 34]. The blood sampling period was restricted to 48 h because the objective of the study was to focus on the early phase disposition of piperaquine that coincided with when clarithromycin attains steady state plasma concentration. Nonetheless the data obtained provided sufficient needed information for the study because plasmodium clearance from infected individuals are usually achieved within 48 hours of therapeutic dosing. However, there was significant increase in the values of piperaquine Cmax, AUC0-48 during co-administration with clarithromycin. PIQ metabolism is majorly mediated by CYP3A4 and clarithromycin (CLR) is a potent inhibitor of the isozyme [35, 36]. The Cmax and AUC0-48 increased by about 3 folds. In addition, the MRT increased 100 percent during co-administration with CLR which can impact duration of therapeutic effect and possibly lead to prolonged side effect. It may also play a vital role in interpreting the risk of drug accumulation. Overall, there was large inter-individual variation in the data as observed in the standard deviation of PIQ with or without co-administration with CLR. The absorption was probably influenced by meals that was provided for the volunteers [37]. Piperaquine is also known to exhibit gender-based discrimination in the values of pharmacokinetic parameters. A statistically significant effect on QT interval prolongation that is linearly related to the Cmax and AUC of PIQ has been reported among females volunteers [38]. This was consistent with observation of 80 % of the population which were female in the study.
Metabolism of PIQ is known to be catalysed selectively by CYP3A4 and CYP2C8. Inhibition can result to loss of activity of CYP3A4 and elevated concentration of PIQ. Clarithromycin, like its analogue erythromycin are potent inhibitors of CYP3A4 [39] it is noteworthy that inhibition of CYP3A4, more frequently cause pharmacokinetic-pharmacodynamic drug-drug interactions. The pronounced systemic plasma concentration of PIQ could not have been unconnected with the inhibition of CYP3A4 metabolism of piperaquine during co-administration with CLR . However clinical significance of CYP3A4 inhibition of PIQ may be inherent in its safety and efficacy which warrants closer understanding of the mechanisms of inhibition and inactivation which may also be exploited for therapeutic gain in certain circumstances [40]. Parasitemia resolution in falciparum malaria is usually achieved within 48 hours of standard dosage of dihydoartemisinin-piperaquine with peak plasma concentration of about 68 ng/ml using capillary sampling of blood in children [41]. The adult therapeutic three day treatment with 960 mg of PIQ have been reported to attain about 500 ng/ml which can raise a clear safety concern like similar members of the 4-aminoquinoline drug class with potential to cause QTc prolongation with irregularities in heart rhythm that may be fatal at the therapeutic doses despite 99% protein binding [42]. This may have consequences when PIQ is co-administered with enzyme inhibitor like CLR that caused a maximum plasma concentration that ranged between 256 ng/ml to 876 ng/ml (Cmax 478.99±148.86 ng/ ml) as reported in this study with a single dose of 960 mg PIQ [43]. It is worthy of consideration because PIQ evince unique pharmacokinetic profiles for instance it exhibit several peak concentrations due to its high protein binding, extensive distribution and high compartelisation [44].
PIQ is generally known to cause tolerable and temporary adverse effects such as dizziness, headache, cough, nausea, vomiting, anorexia, asthenia, abdominal pain, diarrhea, fever, as well as changes in biochemical and blood indices [45]. However, a rare case of choreoathetosisan an involuntary muscle disorder which was not a documented side effect of PIQ has also been reported [46]. The reported adverse effect experienced by the volunteers could be attributable to the enhanced exposure of PIQ during co-administration with CLR [47]. In conclusion it was established that there was drug-drug interaction between PIQ and CLR. Frequent situation that warrants management of peptic ulcer disease is prevalent in many countries with avalanche of reported adverse drug reactions during therapeutic management of uncomplicated malaria with PIQ, a call for caution is inevitable when the drugs are to be co-administered with drug such as clarithromycin A reduction of dosage or substitution of other antimalarial may suffice to prevent potentials leading to toxicity.
Conflict of Interest
The authors declare no conflict of interest
References
-
WHO (2014) Severe Malaria. Tropical Medicine and International Health 19(S1): 7-131.
-
UNICEF (2019) Malaria in children.
-
Nicholas WJ (2022) Severe malaria. Malaria journal 21(1): 284.
-
Tebit EK (2018) Malaria and HIV coinfection in sub- Saharan Africa: prevalence, impact, and treatment strategies. Res Rep Trop Med 27(9): 123-136.
-
Vinay G, Perez G, Dorsey G, Rosenthal PJ, Blaser MJ (2012) The seroprevalence of Helicobacter pylori and its relationship to malaria in Ugandan children. Trans R Soc Trop Med Hyg 106(1): 35-42.
-
Olga S, Pavlova J, Niv Y, Leja N (2018) Epidemiology of Helicobacter pylori infection. Helicobacter 23(1): e12514.
-
Aitila P, Mutyaba M, Okeny S, Kasule MN, Kasule R, et al. (2019) Prevalence and risk factors of Helicobacter pylori infection among children aged 1 to 15 years at holy innocents children’s hospital, Mbarara, South Western Uganda. Journal of Tropical Medicine 7: 9303072.
-
Tsongo L, Nakavuma J, Mugasa, Edwin K (2015) Helicobacter pylori among patients with symptoms of gastroduodenal ulcer disease in rural Uganda. Infection Ecology and Epidemiology 5(1): 26785.
-
Li Y, Choi H, Leung K, Jiang, Fang J, et al. (2023) Global prevalence of Helicobacter pylori infection between 1980 and 2022: a systematic review and meta-analysis Lancet Gastroenterol Hepatol 8(6): 553-564.
-
Asrat D, Nilsson I, Mengistu Y, Soud W, Wadström T, et al. (2004) Prevalence of Helicobacter pylori infection among adult dyspeptic patients in Ethiopia. Ann Trop Med Parasitol 98(2): 181-189.
-
Archampong TN, Asmah RH, Aidoo EK, Wiredu E, Gyasi RK, et al. (2017) Helicobacter pylori cagA and vacA genes in dyspeptic Ghanaian patients. BMC Research Notes 10: 1-5.
-
Olokoba AB, Gashau W, Bwala W, Adamu A, Slawu FK, et al. (2013) Helicobacter pylori Infection in Nigerians with Dyspepsia. Ghana Medical Journal 47(2): 79-81.
-
Bello AK, Umar AB, Borodo MM (2018) Prevalence and risk factors for Helicobacter pylori infection in gastroduodenal diseases in Kano, Nigeria. African Journal of Medical and Health Sciences 17(1): 41-46.
-
Odeghe EA, Adeniyi OF, Oyeleke GK, Keshinor SO (2019) Use of alarm features in predicting significant endoscopic findings in Nigerian patients with dyspepsia. The Pan African Medical Journal 2(34): 36.
-
Gupta V, Perez-Perez GI, Dorsey G, Rosenthal PJ, Blaser MJ (2012) The seroprevalence of Helicobacter pylori and its relationship to malaria in Ugandan children. Trans R Soc Trop Med Hyg 106(1): 35-42.
-
Neelapu RR, Nageswara CPK, Peddinti STR. Paspulati AMC (2013) New Strategies and Paradigm for Drug Target Discovery: A Special Focus on Infectious Diseases Tuberculosis, Malaria, Leishmaniasis, Trypanosomiasis and Gastritis. Infectious Disorders - Drug Targets 13(5): 352-364.
-
Lum PC, Guria NC, Nji N, Yunga B (2018) The Influence of Helicobacter pylori Infection on Malaria Parasitaemia among Symptomatic Patients in Buea, Cameroon International Journal of Tropical Disease and Health 31(4): 1-7.
-
Huang JQ, Hunt RH (1999) The importance of clarithromycin dose in the management of Helicobacter pylori infection: a meta‐analysis of triple therapies with a proton pump inhibitor, clarithromycin and amoxycillin or metronidazole. Aliment Pharmacol Ther13(6): 719- 729.
-
Olusola O (2019) Physiologically based pharmacokinetic modelling of antimalarial agents. PHD thesis, Aston University, UK.
-
Segen CYP3A4 (2012) Segen’s Medical Dictionary. Farlex Inc.
-
Sata F, Sapone A, Elizondo G, Miller VP, Zheng W, et al. (2000) CYP3A4 allelic variants with amino acid substitutions in exons 7 and 12: evidence for an allelic variant with altered catalytic activity. Clinical Pharmacology & Therapeutics 67(1): 48-56.
-
Choi YH, Lee U, Lee BK, Lee MG (2010) Pharmacokinetic interaction between itraconazole and metformin in rats: competitive inhibition of metabolism of each drug by each other via hepatic and intestinal CYP3A1/2. British Journal of Pharmacology 161(4): 815-829.
-
Tarning J, Bergqvist Y, Day P, Bergquist J, Arvidsson B, et al. (2006) Characterization of Human Urinary Metabolites of the Antimalarial Piperaquine Drug Metabolism and Disposition 34(12): 2011-2019.
-
Yang A, Zang M, Liu H, Fan P, Xing J (2016) Metabolite identification of the antimalarial piperaquine in vivo using liquid chromatography–high‐resolution mass spectrometry in combination with multiple data‐mining tools in tandem. Biomedical Chromatography 30(8): 1324-1330.
-
National Center for Biotechnology Information (2023) PubChem Compound Summary for CID 122262.
-
Xie Y, Zhang Y, Liu Y, Jie H (2012) Metabolic Retroversion of Piperaquine (PQ) via Hepatic Cytochrome P450– Mediated N-Oxidation and Reduction: Not an Important Contributor to the Prolonged Elimination of PQ. Drug Metabolism and Disposition 49(5): 379-388.
-
Lemoine A, Williams DE, Cresteil T, Leroux JP (1991) Hormonal regulation of microsomal flavin-containing monooxygenase: tissue-dependent expression and substrate specificity. Molecular pharmacology 40(2): 211-217.
-
Daniel Q, Li DQ, Kim R, McArthur E, Fleet JL, et al. (2015) Risk of adverse events among older adults following co-prescription of clarithromycin and statins not metabolized by cytochrome P450 3A4. Canadian Medical Association Journal 187(3): 174-180.
-
Amar G, Pinto, Ying-Hong W, Naga C, Skaar T, et al. (2005) Inhibition of Human Intestinal Wall Metabolism by Macrolide Antibiotics: Effect of Clarithromycin on Cytochrome P450 3A4/5 Activity and Expression. Clin Pharmacol Ther 77(3): 178-188.
-
Choemang A, Na-Bangchang K (2019) An Alternative HPLC with Ultraviolet Detection for Determination of Piperaquine in Plasma. Journal of Chromatographic Science 57(1): 27-32.
-
Naing C, Mak JW, Aung K, jodon R (2013) Efficacy and safety of dihydroartemisinin-piperaquine for treatment of uncomplicated Plasmodium falciparum malaria in endemic countries: meta-analysis of randomised controlled studies. Trans R Soc Trop Med Hyg 107(2): 65-73.
-
Changui, Zhang R, Hong X, Huang T, Mi S, et al. (2007) Pharmacokinetics of piperaquine after single and multiple oral administrations in healthy volunteers. Yakugaku Zasshi 127(10): 1709-1714.
-
Hai TN, Hietala SF, Van Huong N, Ashton M (2008) The influence of food on the pharmacokinetics of piperaquine in healthy Vietnamese volunteers. Acta Trop 107(2): 145-149.
-
Banda CG, Dzinjalamala F, Mukaka M, Mallewa J, Maiden V, et al. (2018) Pharmacokinetics of piperaquine and safety profile of dihydroartemisinin-piperaquine co- administered with antiretroviral therapy in malaria- uninfected HIV-positive Malawian adults. Antimicrob Agents Chemother 62(8): e00634-18.
-
Niemi M, Backman JT, Neuvonen M, Neuvonen PJ (2003) Effects of gemfibrozil, itraconazole, and their combination on the pharmacokinetics and pharmacodynamics of repaglinide: potentially hazardous interaction between gemfibrozil and repaglinide. Diabetologia 46(3): 347-351.
-
Gandhi S, Fleet JL, Bailey DG, Arthur E, Wald R, et al. (2013) Calcium-channel blocker–clarithromycin drug interactions and acute kidney injury. Jama 310(23): 2544-2553.
-
Annerberg A, Lwin KM, Lindegardh N, Khrutsawadchai S, Ashley E, et al. (2011) A small amount of fat does not affect piperaquine exposure in patients with malaria. Antimicrobial Agents and Chemotherapy 55(9): 3971-3976.
-
Funck-Brentano C, Bacchieri A, Valentini G, Pace S, Tommasini, et al. (2019) Effects of dihydroartemisinin- piperaquine phosphate and artemether-lumefantrine on QTc interval prolongation. Scientific Reports 9(1): 1-8.
-
Akiyoshi T, Ito M, Murase S, Miyazaki M, uengerich FP, et al. (2013) Mechanism-based inhibition profiles of erythromycin and clarithromycin with cytochrome P450 3A4 genetic variants. Drug Metabolism and Pharmacokinetics 28(5): 411-415.
-
Zhou Q, Yu X, Shu C, Cai Y, Gong W, et al. (2011) Analysis of CYP3A4 genetic polymorphisms in Han Chinese. Journal of human genetics 56(6): 415-422.
-
Zongo, Issaka, Fabrice A, Some, Somda AM, et al. (2014) Efficacy and day 7 plasma piperaquine concentrations in African children treated for uncomplicated malaria with dihydroartemisinin-piperaquine. PLoS One 9(8): e103200.
-
Chan XHS, Haeusler IL, Win YN, Pike J, Hanboonkunupakarn B, et al. (2021) The cardiovascular effects of amodiaquine and structurally related antimalarials: An individual patient data meta-analysis. PLoS Medicine 18(9): e1003766.
-
Darpo B, Ferber G, Siegl P, Laurijssens B, Macintyre F, et al. (2015) Evaluation of the QT effect of a combination of piperaquine and a novel anti‐malarial drug candidate OZ439, for the treatment of uncomplicated malaria. Br J Clin Pharmacol 80(4): 706-715.
-
Tausif A, Sharma P, Gautam A, Brijesh V, Monica K, et al. (2008) Safety, tolerability, and single‐and multiple‐dose pharmacokinetics of piperaquine phosphate in healthy subjects. The Journal of Clinical Pharmacology. 48(2): 166-175.
-
Liu H, Zhou H, Cai T, Zang M, Xing J, et al. (2018) Metabolism of piperaquine to its antiplasmodial metabolites and their pharmacokinetic profiles in healthy volunteers. Antimicrobial Agents and Chemotherapy 62(8): e00260-18.
-
Adam I, Tarning J, Lindegardh N, Mahgoub H, Gready R, et al. (2012) Pharmacokinetics of Piperaquine in Pregnant Women in Sudan with Uncomplicated Plasmodium falciparum Malaria. American. Journal of Tropical Medicine and Hygiene 87(1): 35-40.
-
Kadia BM, Morfaw C, Simo AG (2017) Choreoathetosis– an unusual adverse effect of dihydroartemisinin- piperaquine: a case report. J Med Case Rep 11(1): 1-5.
- Gallic and Citric Acid Present in the Peels of Tropical Fruits as an Alternative in the Fight against Cancer
- Treating the Forehead Lines with Combination of Forehead and Glabellar Botulinum Toxin Among Japanese Patients
- Clinical Evaluation of Patients Suffering from Breast Cancer & Determination of Treatment Therapies and Better Strategies Related to Breast Cancer
- Medieval Recipes by Al-Zahrāwī for Heart Palpitations Treatment
- Etiology and Prescription Errors of Myocardial Infarction in Different Health Care Systems of Azad Kashmir
- Early Diagnosis and Multidisciplinary Management of Turner Syndrome: A Paediatric Case Study