Treatment Strategies for Pancreatic Ductal Adenocarcinoma: Exploring Multimodal Therapeutic Approaches
Pancreatic ductal adenocarcinoma (PDAC) remains one of the most formidable malignancies. The gloomy prognosis of PDAC is attributed to its aggressive nature, which is characterized by expeditious metastasis, treatment resistance, and lack of early detection methods. PDAC is driven by genetic alterations, including mutations in the KRAS oncogene, TP53, CDKN2A, and SMAD4
Alam M¹*, Abbas K² and Mustafa M³
¹Indian Biological Sciences and Research Institute (IBRI), India ²Department of Zoology, Faculty of Life Sciences, Aligarh Muslim University, India ³Department of Biochemistry, J.N. Medical College, Aligarh Muslim University, India *Corresponding author: Mudassir Alam, Indian Biological Sciences and Research Institute (IBRI), Noida, Delhi, India, Email: syedalamalig@gmail.com Adenocarcinoma; PDAC; Tumor
Editorial
Pancreatic ductal adenocarcinoma (PDAC) remains one of the most formidable malignancies. The gloomy prognosis of PDAC is attributed to its aggressive nature, which is characterized by expeditious metastasis, treatment resistance, and lack of early detection methods. PDAC is driven by genetic alterations, including mutations in the KRAS oncogene, TP53, CDKN2A, and SMAD4 [1, 2]. Genetic alterations lead to anomalies in vital biological processes that regulate cell invasion, apoptosis [3], and proliferation. Furthermore, the development of PDAC depends on the tumor microenvironment (TME). Its distinctive features include dense desmoplastic stroma and immunosuppressive mechanisms that lead to treatment resistance [4]. The new PDAC paradigm has evolved into multimodal therapy, which combines many treatment techniques to battle the ailment. Multimodal approaches aim to overcome the limitations of single-agent therapy and address the heterogeneity of PDAC by focusing on many disease features. Understanding multimodal therapies, surgical interventions, chemotherapy, radiation therapy, targeted medicines, and immunotherapy is critical to providing PDAC patients with the best potential prognosis. The molecular complexity and TME of PDAC are responsible for its aggressive character and resistance to treatment. High levels of genetic heterogeneity, including the accumulation of many somatic mutations and chromosomal abnormalities, are characteristics of PDAC [5]. Over 80% of cases have to activate KRAS mutations, which are widely present and cause constitutive activation of the PI3K/AKT/ mTOR and RAS/RAF/MEK/ERK signaling pathways. This promotes cell survival, proliferation, and metastasis. Apart from KRAS, deactivating mutations in tumor suppressor genes, including TP53, CDKN2A, and SMAD4, are frequently detected, resulting in abnormalities related to cell cycle regulation, programmed cell death, and transforming growth factor-beta (TGF-β) communication, in that order [6, 7]. Furthermore, DNA methylation abnormalities and histone alterations indicate epigenetic modifications resulting in altered gene expression and silencing patterns [8, 9]. A study describes the TME in PDAC as a thick desmoplastic stroma composed of an extracellular matrix (ECM), activated pancreatic stellate cells, and immune cells [10]. Another study proposes that this desmoplastic reaction creates a nutrient- and oxygen-deprived environment that promotes treatment resistance and cancer stem cell morphologies. The immunosuppressive features of the TME, which are regulated by regulatory T cells, myeloid-derived suppressor cells, and cytokines like TGF-β, further impede anti-tumor immune responses [11]. The majority of PDAC cases are diagnosed at later stages, making surgical resection not feasible, which exacerbates the difficulties associated with late identification. This emphasizes the importance of implementing early detection techniques and individualized treatment plans based on the molecular heterogeneity and TME specific to each patient [12].
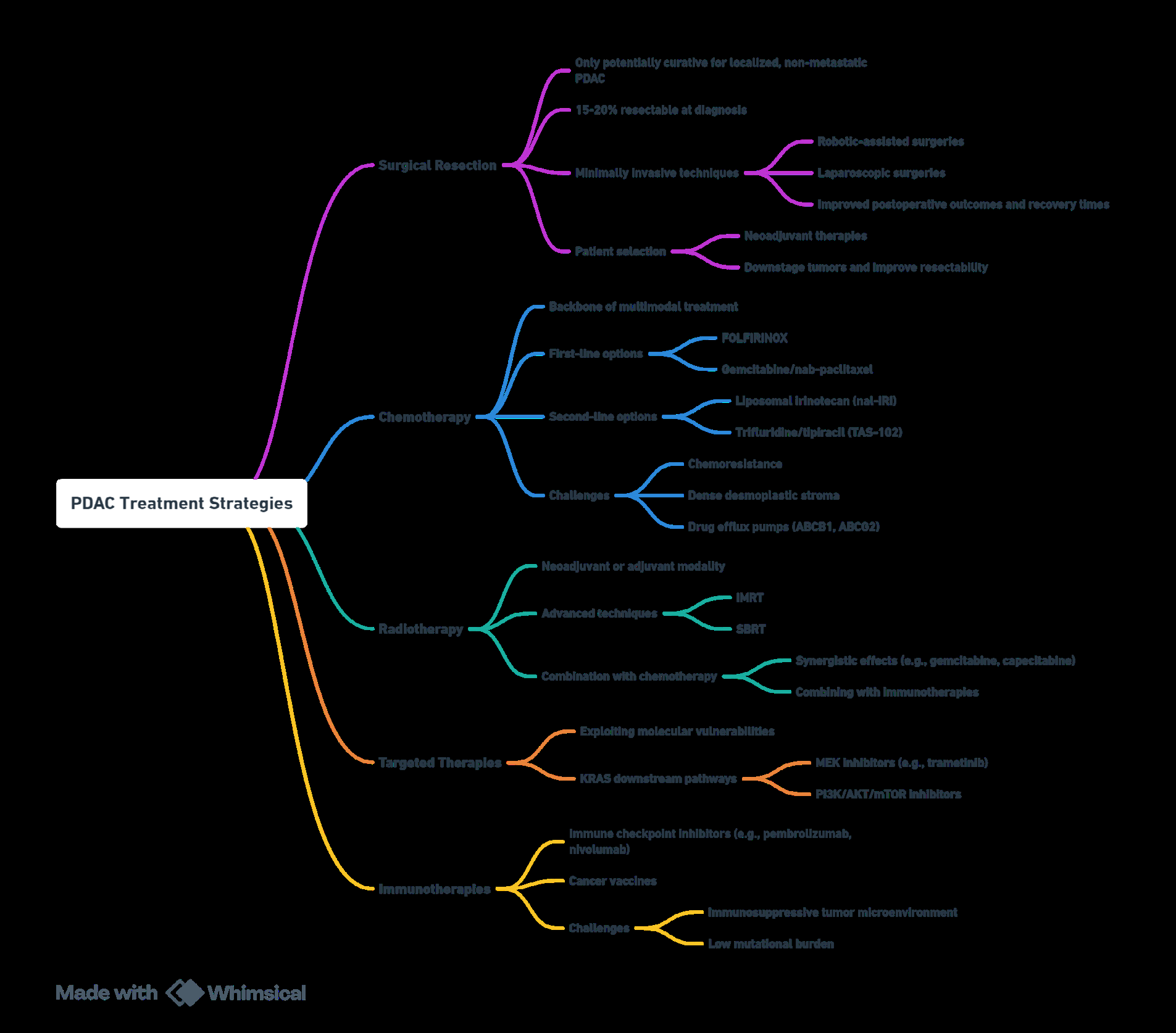
The only potentially curative treatment option available for PDAC patients with localized, non-metastatic disease is still surgical excision. However, as per study, only 15- 20% of cases are considered treatable at diagnosis [13]. Robotic-assisted and laparoscopic operations are minimally invasive methods that have improved postoperative outcomes and shortened recovery times. Careful patient selection is crucial for surgical resection, which frequently incorporates neoadjuvant therapy to reduce tumor size and increase respectability. Chemotherapy is the mainstay of the multimodal PDAC treatment plan [14]. The standard first- line chemotherapy regimens for metastatic PDAC include gemcitabine/nab-paclitaxel and the FOLFIRINOX regimen, which consists of 5-fluorouracil, leucovorin, irinotecan, and oxaliplatin as a combination. In second-line treatment settings, innovative chemotherapeutic medicines including trifluridine/tipiracil (TAS-102) and liposomal irinotecan (nal-IRI) have shown promising results [15]. Resolving chemoresistance remains a significant challenge, which is typically connected to thick desmoplastic stroma and enhanced expression of drug efflux pumps such as ABCG2 (BCRP) and ABCB1 (MDR1) [16]. Radiotherapy, whether utilized as an adjuvant or neoadjuvant therapeutic modality, is a critical component of multimodal PDAC treatment.
Modern radiation therapy delivery technologies, such as stereotactic body radiation therapy (SBRT) and intensity- modulated radiation therapy (IMRT), have decreased toxicity to surrounding healthy tissues while increasing targeting precision [17]. Targeted therapies exploit PDAC by focusing on specific oncogenic pathways and the TME. For example, PI3K/AKT/mTOR inhibitors and MEK inhibitors (e.g., trametinib) are KRAS downstream effector pathway inhibitors being explored in combination with chemotherapy [18]. Certain PDAC patients, particularly those with a high mutational burden and microsatellite instability, have reacted well to immunotherapies such as immune checkpoint inhibitors (e.g., pembrolizumab, nivolumab) and cancer vaccines. However, the low mutational burden in PDAC and the immunosuppressive TME remain significant obstacles to immunotherapy [19] (Figure 1).
References
-
Stefanoudakis D, Frountzas M, Schizas D, Michalopoulos NV, Drakaki A, et al. (2024) Significance of TP53, CDKN2A, SMAD4 and KRAS in Pancreatic Cancer. Curr Issues Mol Biol 46(4): 2827-2844.
-
Mustafa M, Abbas K, Alam M, Habib S, Zulfareen, et al. (2024) Investigating underlying molecular mechanisms, signaling pathways, emerging therapeutic approaches in pancreatic cancer. Front Oncol 14: 1427802.
-
Mustafa M, Ahmad R, Tantry IQ, Ahmad W, Siddiqui S, et al. (2024) Apoptosis: A Comprehensive Overview of Signaling Pathways, Morphological Changes, and Physiological Significance and Therapeutic Implications. Cells 13(22): 1838.
-
Thomas D, Radhakrishnan P (2019) Tumor-stromal crosstalk in pancreatic cancer and tissue fibrosis. Mol Cancer 18(1): 14.
-
Heinrich MA, Mostafa AMRH, Morton JP, Hawinkels LJAC, Prakash J (2021) Translating complexity and heterogeneity of pancreatic tumor: 3D in vitro to in vivo models. Adv Drug Deliv Rev 174: 265-293.
-
McCubrey JA, Steelman LS, Chappell WH, Abrams SL, Montalto G, et al. (2012) Mutations and deregulation of Ras/Raf/MEK/ERK and PI3K/PTEN/Akt/mTOR cascades which alter therapy response. Oncotarget 3(9): 954-987.
-
Mustafa M, Abbas K, Alam M, Ahmad W, Moinuddin, et al. (2024) Molecular pathways and therapeutic targets linked to triple-negative breast cancer (TNBC). Mol Cell Biochem 479(4): 895-913.
-
Handy DE, Castro R, Loscalzo J (2011) Epigenetic modifications: basic mechanisms and role in cardiovascular disease. Circulation 123(19): 2145-2156.
-
Mudassir A, Abbas K, Chaudary B, Asif S, Balti A (2024) Computational Analysis of Selected Phytochemicals for their PARP Inhibitory Potential in Cancer. Acta Biochem Iran 2(1): 11-21.
-
Ferrara B, Pignatelli C, Cossutta M, Citro A, Courty J, et al. (2021) The Extracellular Matrix in Pancreatic Cancer: Description of a Complex Network and Promising Therapeutic Options. Cancers (Basel) 13(17): 4442.
-
Wu P, Gao W, Su M, Nice EC, Zhang W, et al. (2021) Adaptive Mechanisms of Tumor Therapy Resistance Driven by Tumor Microenvironment. Front Cell Dev Biol 9: 641469.
-
Schepis T, De Lucia SS, Pellegrino A, Del Gaudio A, Maresca R, et al. (2023) State-of-the-Art and Upcoming Innovations in Pancreatic Cancer Care: A Step Forward to Precision Medicine. Cancers (Basel) 15(13): 3423.
-
Wei K, Hackert T (2021) Surgical Treatment of Pancreatic Ductal Adenocarcinoma. Cancers (Basel) 13(8): 1971.
-
Muaddi H, Kearse L, Warner S (2024) Multimodal Approaches to Patient Selection for Pancreas Cancer Surgery. Curr Oncol 31(4): 2260-2273.
-
Hatashima A, Arango MJ, Reardon J, Freeman T, Williams T, et al. (2022) First-line gemcitabine plus nab-paclitaxel versus FOLFIRINOX for metastatic pancreatic cancer in a real-world population. Future Oncol 18(20): 2521-2532.
-
Robey RW, Pluchino KM, Hall MD, Fojo AT, Bates SE, et al. (2018) Revisiting the role of ABC transporters in multidrug-resistant cancer. Nat Rev Cancer 18(7): 452- 464.
-
Shouman MA, Fuchs F, Walter F, Corradini S, Westphalen CB, et al. (2024) Stereotactic body radiotherapy for pancreatic cancer - A systematic review of prospective data. Clin Transl Radiat Oncol 45: 100738.
-
Zhang J, Darman L, Hassan MS, Von Holzen U, Awasthi N (2023) Targeting KRAS for the potential treatment of pancreatic ductal adenocarcinoma: Recent advancements provide hope (Review). Oncol Rep 50(5): 206.
-
Melzer MK, Arnold F, Stifter K, Zengerling F, Azoitei N, et al. (2020) An Immunological Glance on Pancreatic Ductal Adenocarcinoma. Int J Mol Sci 21(9): 3345.
- An Efficient and Affordable Method for Isolating Bone Marrow- Derived Mesenchymal Stem Cells from Swiss Albino Mice
- Superposition of Cryo-EM and AlphaFold Predictions of Dengue Antigen-Antibody Complexes
- Jugular-Applied Coherent Low-Level Laser Therapy Enhances Systemic Mitochondrial Metabolic Function and Antioxidant Response
- Role of OMC32 Polypeptide in Acrosin-Mediated Exocytosis during the Bovine Sperm Acrosome Reaction
- Association of Galectin-3 but not Laminin in Tamoxifen-Induced Growth Suppression in Breast Cancer MCF-7 Cells
- Effect of Different Wavelengths of Light on the Rate of Photosynthesis