Establishment of Disease Surveillance Systems in Rural Communities of Sierra Leone
Using the native intelligence of rural people to establish a surveillance system reduces morbidity, mortality, poverty, and zoonotic and neglected disease outbreaks among humans and animals. People in rural communities constantly interact with domestic and wildlife, placing them at high risk of exposure to diseases. Health personnel is unevenly distributed, with the majority in the capital cities, making rural communities lack professional health personnel and health care service providers. Poverty limited rural people’s access to health care facilities. Emerging disease outbreaks resulting from complicated environmental changes pose a fundamental challenge in low-income countries, impacting the foundation of human and animal health. People find it difficult to reach medical centers due to a lack of funds. The Animal Health Club engaged thirty (30) villages in a focus group discussion and in-depth interview. Animal Health Club used information obtained to develop a semistructured questionnaire (600) and observed the people during the talks. Community people identify nine sources of diseases, including humans, poultry, wildlife, pets, ruminants’ crops, water, toilets, and garbage dump. The people elected/selected an executive to organize and nominate people to surveillance the nine sources of diseases. Large villages were divided into zones, while smaller villages remain the same. The people identified ten domestic animals and twenty-four wildlife animals in their communities and some diseases associated with them. They also revealed a high level of interaction between domestic, wildlife, and humans in towns and bush in their respective communities. Rural people believed animals transfer diseases to humans in various ways. However, people contract diseases more from human-human interaction than human- animals interaction. The study’s main objective was to explore livestock and wildlife disease interface and transmission chains within the human population in the selected communities and establish community-level epidemiological surveillance systems to reduce disease incidence.
Introduction
With the high level of animal-human interaction, there was a strong justification for the establishment of Surveillance sentinels for monitoring zoonotic diseases and the Animal health club ( AHC) for raising awareness on disease prevention and control, good animal husbandry practices, and environmental sanitation as a means to reduce of contracting diseases from these sources. During setting up AHCs, the people interviewed in the study identified the following sources humans can contract diseases; water, garbage dump, toilets, crops, humans, poultry, ruminants, pets, and wildlife. With this information. The zonal heads of AHCs were mandated to appoint two persons per each source of disease identified to monitor and report to the zonal moderator. These monitors were referred to as sentinel site monitors.
The study recorded stories from the people who have been directly affected by the Ebola virus, a zoonotic disease whose spread could have been quickly curbed had surveillance and AHC been fully functional in Sierra Leone. As reported by the people, the impact of Ebola included the death of their relatives, loved ones, and breadwinners and the adverse effects quarantines had on group work, food production, livelihood, education, business, and social activities.
The information generated by the study was documented and kept at the MAFFS wildlife department and Njala University Zoonotic Laboratory for future reference.
- Humans
- Ruminants
- Poultry
- Pets
- Wildlife
- Crops
- Water
- Garbage dumps
- Toilet Emerging and endemic zoonotic diseases pose a more significant disease burden in the developing world, with a significant societal impact on resource-poor rural communities [1, 2]. Rural communities in low-income countries carry the most critical responsibility for zoonotic and neglected zoonotic diseases [3]. Over the past hundred years, multiple disease outbreaks have occurred worldwide. Countries with the best health facilities have managed to contain diseases such as SAR, Ebola, Salmonella Typhimurium, and Avian influenza, but persist in rural communities of low-income countries [3].
These outbreaks occur mainly due to complicated changes occurring in the natural world and its ecosystems threatening the foundation of human health and survival, such as food yield, water availability, the constraint on infectious disease outbreaks, and buffers against extreme weather environmental challenges [4]. These are likely to increase poverty, decrease food intake and compromise the rural poor’s immune system.
People living around forest edge communities, mountainous terrain, and islands constantly interact with domestic and wildlife animals. Many such communities are hard-to-reach areas with vehicles and bikes [5]. Moreover, the people also find it extremely difficult to travel to medical centers for treatment due to a lack of funds. Surveillance systems established in most countries hardly reach such communities [5]. The inability of surveillance systems to reach such communities results in exponential exposure to the pandemic and the death of both animals and humans.
In Sierra Leone, the majority of the population, 58% [6], lives in rural communities engaged in subsistence farming and constantly interacting with livestock and wildlife, thereby increasing the risk of contracting diseases such as rabies and Lassa fever. Wildlife from Ivory Coast, Guinea, Liberia, and Sierra Leone interact around Kailahun, Pujehun, Kono, and Koinadugu districts. The 2013 Ebola outbreak in Sierra Leone started around forest edge communities in the Kailahun district, sharing borders with Liberia, Guinea, and Sierra Leone. Surveillance systems in Sierra Leone do not cover most of the communities in this district. Surveillance systems are limited to towns with health posts and villages within five miles radius [7].
Rural communities in Sierra Leone are at high risk of exposure to zoonotic and neglected diseases. Rural communities in this context are geographical areas located outside towns and cities and face challenges relating to demographic changes, workforce development, capital access, infrastructure, health, land use, environment, and community development strategies. Establishing a surveillance system in these hard-reach communities will drastically reduce exposure morbidity and mortality and hence pandemic.
Why should we establish a Surveillance System in Sierra Leone Rural Communities?
Multidimensional poverty index and multiple barriers limit rural communities’ access to medical care, leading to morbidity and mortality from zoonotic and non-zoonotic diseases [8, 9, 10]. In Sierra Leone, more than half of the population lives in rural communities, 58% [5], with a multidimensional poverty index of 64.8% [8]. Geographical location, self-paid medical bills, lack of skilled medical professionals, and poor-quality services make it difficult to access medical care [10, 11] uneven distribution of health and medical personnel in the country. The capital city Freetown has more health care and referral facilities and workers than the rest of the country [12].
The government introduced Free Health care for suckling mothers, but people in rural communities do not enjoy this facility due to charges requested by medical staff.
Those who make it will not be able to pay for all the medical bills and hence return home without completing treatment. Those who attempt to visit hospitals do so with gifts such as rice, palm oil, fish and chicken, or a piece of traditional bush meat (Roland Suluku Personal Observation, 2018). Older men and women who visit the hospitals do so by the household tasking every member to pay for the trip. In most cases, they share requests equally among all family members. As a result of poverty, some take loans or delay paying these contributions, resulting in the patient’s death.
Medical practitioners often visit Rural communities to provide free medical services. Most people miss these opportunities due to a lack of transportation. The people do not use ambulances provided by the government to service people in rural communities because they cannot afford the charges levied by the local councils. Sick people, in most cases, are taken back home or die. Mature people in these communities visit hospitals only after harvesting their crops. They sell their products and use the proceeds to pay for medical bills.
Sierra Leone is one of the hungriest countries in the world. Crop yields have drastically reduced due to decreased soil fertility caused by lumbering, deforestation, slash and burn method, and charcoal burning. These activities have reduced crop harvest leading to food insecurity in rural communities. Rural communities can no longer boast of a bumper harvest and cannot sell harvested crops to invest in other social amenities or medical services. Establishing surveillance systems in rural communities will assist rural people in knowing about all the animals in their communities, the diseases associated with them, the signs and symptoms related to each disease in their communities, and some medications for treatment and curing such disease conditions.
Methodology of Data Collection
Focus Group Discussion
Animal Health Club divided the focus group discussion into three groups. Youths aged between 15-35years comprise both girls and boys. The older women from 36 years and above and the older men aged range 36years and above were interviewed. The research team includes a prompt person who initiates the discussion, a recorder, and a person to issue out cards. Groups set rules and the process of how the debate should proceed. A card system was used to prevent one person from dominating the discussion. A participant will raise their hand, and the person issuing the card will give the card before the person talks. Each card is marked with a letter and number. Each participant will only speak three times during the discussion. However, if others do not participate in the discussion, a participant will be allowed to speak more than three times. Names of individuals are not recorded, but only the letter on the card and number. Aside from the focus group discussion, the research team will observe and record any side comments during the discussion. The discussion lasted for thirty minutes or a maximum of one hour. The voices were recorded and placed in tabular form.
Structured Questionnaire
The animal health Club designed six hundred structured questionnaires and distributed them to twenty people in each community. The team interviewed 30 communities. The purpose of the questionnaire was to identify the people living in the 30 communities, their source of income, types of animals, and management system, which will show the level of interaction. The questionnaires were designed to elicit data relating to diseases associated with domestic and wildlife in these communities, mode of treatment, control, and prevent such conditions. The questionnaire also explores some information on bats, bushmeat consumption, and Ebola.
People interviewed were randomly selected. The number of houses was counted and divided by the total number of questionnaires. Animal Health Club interviewed an equal number of older men and women household heads. The team scrutinized and amended the questionnaires to ensure that not more than twenty minutes were spent interviewing an individual. The questionnaires were administered, collected, and analyzed using census pro.
In-Depth Study
Animal Health Club interviewed vital informants such as animal rearers, hunters, traditional healers or herbalists, and older adults in the communities. Discussions relating to disease outbreaks in the past, how they responded, types of animals they have, live within their communities, diseases associated with these animals, and those potentially infectious to human beings. These discussions guide the establishment of the surveillance system.
Observation
The research team trained members to observe the people’s behavior in their respective environments and compare their thought with what emerged from the discussions. These observational guides are written and discussed in detail to identify topics and gaps for further studies. The information generated can solve a gap between their teachings and practices. Observations are vital in research as communities are sensitive about researchers and most often unwilling to disclose or divulge information, particularly after Ebola. Researchers were empowered to get sharp details which naturally is difficult to obtain from communities.
Method of Forming the Animal Health Club to establish a Surveillance System establishment of Disease Surveillance Systems in Rural Communities of Sierra Leone?
The First Step is to Engage the Villages in Focus Group Discussion
Establishing disease surveillance systems in rural communities is the right step to saving the lives of millions of people in such communities. In Sierra Leone, sheep, goats, chickens, and dogs are present in most communities. They have vast knowledge about the existence of wildlife and the diseases associated with these animals.
The first action is to form Animal Health Clubs in each community. The animal health club is an organization established to cater to the health needs of both lower (Domestic and Wildlife) and higher (Human beings) animals. Every member in the community or town, including school- going children, becomes a club member. The following are steps involved in the formation of the animal health club.
The first step involves scoping the mission to the paramount chief and town chiefs of the town or village. The team leader visits the paramount chief and explains the purpose of the visit. In some cases, visitors give the chief ten thousand (Le 10,000.00) Leones as traditional demands. It is not compulsory. The town chief invites the town’s elders or household head to the meeting. The Animal Health Club team leader explains to the authorities that the animal health club educates people in rural communities and raises awareness on good animal husbandry practices, environmental health and sanitation, toilet, water and wildfire management, and disease control and prevention. Such as rabies, new castle disease, and Peste des petit ruminant.
The second step is to engage the whole village in focus group discussion. The focus group discussion aims to identify and name all the domestic animals (chicken, ducks, pigeon, sheep, goat, cattle, cats, dogs) and wildlife. They also called the various diseases associated with these animals, their signs and symptoms, how people contract diseases from animals, transfer from humans to animals, and some local or traditional herbs used to treat them. The diverse sources of diseases affect the people in their communities. Communities identified nine sources of infections affecting them in their communities. Surveillance systems collect information from these nine sources, which include:
- Humans
- Ruminants
- Poultry
- Pets
- Wildlife
- Crops
- Water
- Garbage dumps
- Toilet Zonal heads appointed people two’s each week or bi- weekly to monitor and surveillance these sources. The third step is to form the clubs’ executives, which comprise a chairperson, deputy chairperson, secretary, public relations officer, and zonal head. The process can be carried out by selection or election depending on the town or village and the people. Here the community selects or elects an engaged person who loves animals as the chairperson and deputy chairperson. A public relations officer is famous and interacts with everyone in the town or village. He has a following, and people can listen to him. The secretary is the village teacher or a school dropout who can often read and write, and the zonal head is a famous person in a section of the town.
The fourth step is to divide the town or village into sections or zones. If the town or village is small, no division takes place. The executive divided the towns and villages into zones and appointed people to monitor the animals and sources of diseases listed during focus group discussions. These sources include ruminants (Cattle, Sheep, and goats) and non-ruminants (chicken, duck, pigs, pigeon), pets (dogs and cats), wildlife, humans, water, and toilets. Each zonal head appoints people to monitor these nine areas for two weeks, and other team members are set aside to take up from them.
The fifth step is to train the appointed or selected Monitors on passive and active surveillance, syndromic surveillance, and event-based surveillance—collecting, collating, and reporting data. The data collected should go through the Zonal head to the chairman. He will take the correct information to the town chief for approval before sending the information to the relevant authorities. The Animal Health Club will visit the communities for six months to ensure the people adequately understand the system.
Reporting Procedure
The reporting procedure for disease surveillance from community level to national levels is in Figure 1 below.
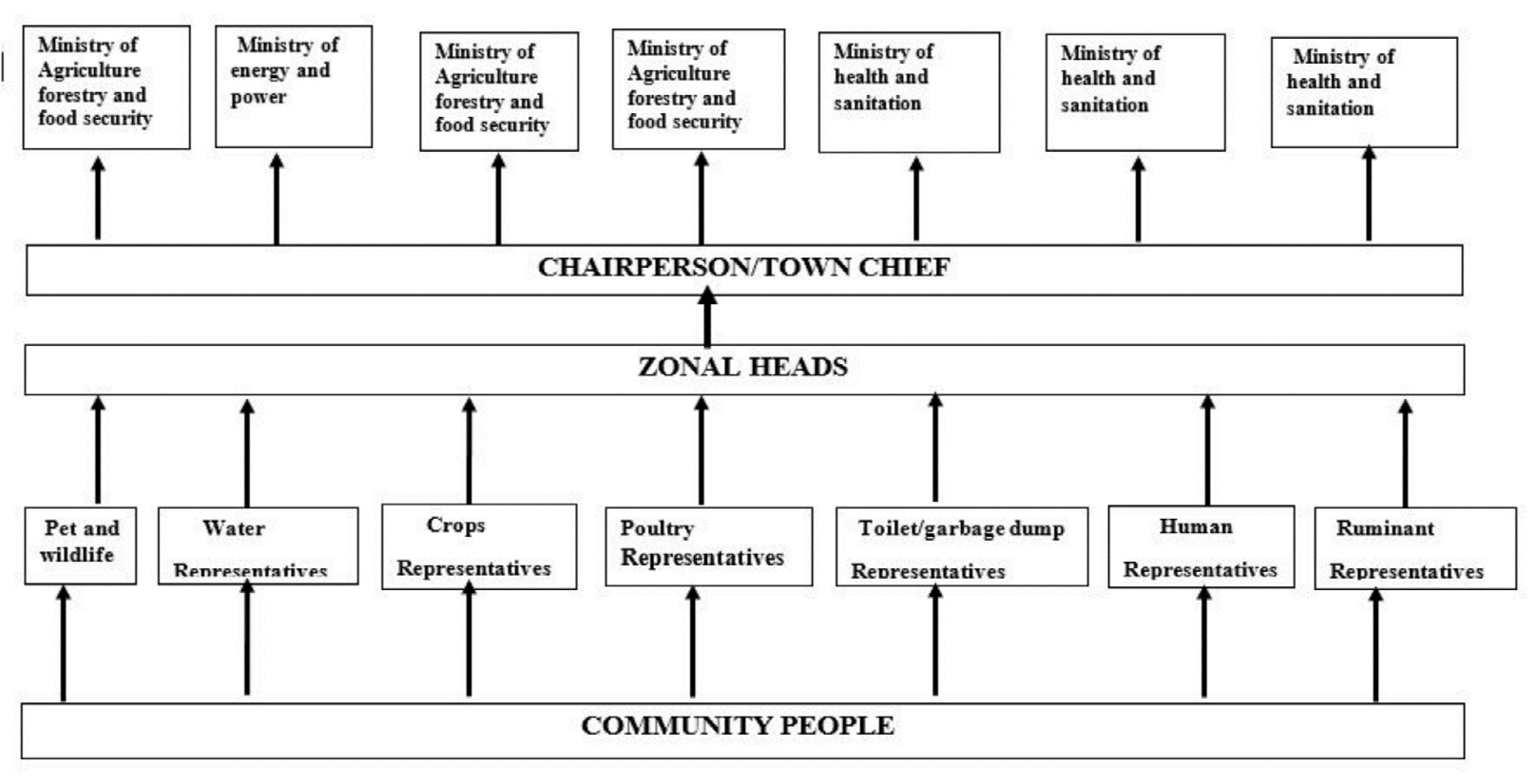
Figure1: Proposed reporting structure for disease monitoring and surveillance.
Results
| No | Animals Regions | Domesticated | Wildlife |
|---|---|---|---|
| 1 | Eastern | Dog, Cat, Sheep, Goat, Chicken, Duck, Pig, Cow, Pigeon, Guinea Fowl. | Elephant, Bush dog, Bush hog, Buffalo Squirrel, Baboon, Bush cat, Ground Squirrel, Rat, Bush cat, Rabbit, Bats, Monkey, Fox, Grasscutter, Tuttle, Porcupine, Chimpanzee, Giant rat, Deer, Antelope, tiger, Pumpkin pine Snake, Leopard, Muscat |
| 2 | Southern | Goat, Sheep, Duck, Chicken, Cat, Dog, Guinea fowl, Pigeon, Pig | Grasscutter, Buffalo, Antelope, Squirrel, Deer, Monkey, Rat, Tiger, Bush goat, Royal antelope, Tree squirrel, Dicker Rabbit, Mongoose, Giant, rat, Chimpanzee, Porcupine, Bush cat, Bush hog, Bamboo, Kapolei, Mongoose, pewee, Red fox, Snail, Tuttle |
| 3 | Northern | Goat, Sheep, Chicken, Cat, Cow v | Squirrel, Bush dog, monkey, Deer, Lion, Buffalo Bush hog, Antelope, Water deer, Grasscutter, leopard, Giant rat, Rat, Monkey, Chimpanzee, Bamboo, Elephant, Bush goat, Rabbit Hyena, Pumpkin pine, Leopard, Dicker, Red monkey, White monkey, wolf, Hippopotamus, Gorilla, Bush cat, Stone goat, Black squirrel, Muscat, Red fox, Ndadaqui (Longtail squire) |
Table 1: List of Domestic and Wildlife animals in the south, east, and Northern Province of Sierra Leone.
| No. | Domestic animals | Diseases with which they are associated |
|---|---|---|
| 1 | Cattle | Ringworm (dermatophytosis), Cryptosporidiosis, Cysticercosis Anaplasmosis, Heartwater, Ascariasis (roundworm), trans Crimean- Congo Hemorrhagic fever, Trichinosis, Poxvirus, Rabies, Q – fever, Salmonellosis (Gastroenteritis), Leptospirosis, Escherichia coli, Brucellosis, Anthrax. |
| 2 | Goat and sheep | Ringworm (dermatophytosis), Anaplasmosis, Heartwater, Ascariasis (roundworm), Tuberculosis, Crimean- Congo Hemorrhagic fever, Chlamydiosis (Enzootic abortion), Caseous Lymphadenitis, Johne’s disease (Para-tuberculosis), Ringworm, Rift Valley Fever, Sore-mouth (Orf), Rabies, Toxoplasmosis, Listeriosis, Q – fever, Escherichia coli, Brucellosis, Anthrax |
| 3 | Goat | Cryptosporidiosis |
| 4 | Sheep | Tularemia |
| 5 | Swine | Ebola, Cysticercosis, Ringworm (dermatophytosis), Ascariasis (roundworm), Balantidiasis, Giardiasis, Tuberculosis, Influenza, Crimean- Congo Hemorrhagic fever, Trichinosis, Poxvirus, Brachyspira pi Losi Coli, Rabies, Brucellosis, Anthrax |
| 6 | Cat | Ringworm (dermatophytosis), Ascariasis (roundworm), Giardiasis, Mange, Histoplasmosis, Lyme disease, Fleas, Tularemia, Encephalopathy, Bovine spongiform/Creutzfeldt-Jakob disease- transmissible spongiform encephalopathy, Strongyloidiasis, Visceral Larval Migrans (VLM), Rabies, Toxoplasmosis, Yersiniosis (Yersinia enterocolitis), Listeriosis, Salmonellosis (Gastroenteritis), Escherichia coli, Salmonellosis |
| 7 | Dog | Salmonellosis, Ebola, Ringworm (dermatophytosis), Giardiasis, Histoplasmosis, Mange, Lyme disease, Tularemia, Strongyloidiasis, Visceral Larval Migrans (VLM), Brachyspira pilosicoli, Yersiniosis (Yersinia enterocolitica), Rabies, Listeriosis, Brucellosis, Fleas. |
| 8 | Domestic bird | Ascariasis (roundworm), Balantidiasis, Tuberculosis, Influenza, Poxvirus, Brachyspira pilosicoli, Salmonellosis (Gastroenteritis), New Castle |
| 9 | Rabbit | Cryptosporidiosis, E. cuniculi, Fleas, Cheyletiella, Dermatomycosis, Rabies. |
Table 2: Zoonotic diseases of domestic animals.
| No. | Wildlife | Zoonotic diseases |
|---|---|---|
| 1 | Antelope | Rift valley fever, Rinderpest, Foot and mouth disease, Blue Tongue, Rabies, Lumpy skin diseases, Crimean-Congo Hemorrhagic fever, Bovine virus, diarrhea, Babesiosis, Theileriosis, Trypanosomiasis, Heartwater, Anaplasmosis, Brucellosis, Anthrax, Tuberculosis |
| 2 | Deer | Brucellosis, Encephalopathy, Anthrax, Tularemia |
| 3 | Rodent | Ringworm (dermatophytosis), Plague, Lyme disease, Tularemia, Tuberculosis, Salmonellosis |
| 4 | Monkey | Salmonellosis, Tuberculosis, Ornithosis, Hepatitis A, Balantidiasis, Rabies |
| 5 | porcupine | Salmonellosis, Tuberculosis, Lyme disease, Tularemia, Leptospirosis, porcupine, Rabies, Plague |
| 6 | Wild birds | Ringworm (dermatophytosis), Histoplasmosis, Influenza, Tuberculosis |
| 7 | Rats | Rat-bite fever, Bubonic plague |
| 8 | Fish | Salmonellosis |
| 9 | Hog | Salmonellosis |
| 10 | Frog | Tularemia, Salmonellosis |
| 11 | Rabbits | Plague, Ringworm (dermatophytosis), Lyme disease, Tularemia |
| 12 | Squirrel | Leptospirosis, Lyme disease, Tularemia, Rabies |
| 13 | Hares | |
| 14 | Bat | Lyme disease, Rabies, Histoplasmosis, Ebola |
| 15 | Fox | Brucellosis, Rabies |
| 16 | Ground squirrel | Bubonic plague |
| 17 | Pigeon | Ornithosis |
| 18 | Chimpanzee | Ebola, Marburg |
| 19 | None-human primate | Tuberculosis |
| 20 | Mastomys spp | Lassa fever |
| 21 | Snake | Salmonellosis |
| 22 | Turtle | Salmonellosis |
| 23 | Lizard | Salmonellosis |
Table 3: Zoonotic diseases of wildlife.
| Wildlife- domestic animal interaction | Wildlife –Human interaction | |||
|---|---|---|---|---|
| Type of Wildlife animal | Place of interaction | Purpose of interaction | Place of interaction | Purpose of Interaction |
| Bush dog | ||||
| Bamboo | Bush | Bush and farm | Searching for food, hunting, pets, research, and trap | |
| Kapolei | ||||
| Peewee | ||||
| Red Fox | ||||
| Snail | Bush, farm, and town | Searching for food, prey for other animals | Town, bush, farm, and water | Search for food consumed by humans, medicine, and income |
| Tuttle | Bush and water | Searching for food, preyed upon by other animals | Water and bush | Searching for food caught during fishing collected for consumption, pets, sold, medicine |
| Bush Hog | Bush, water, and farms | Search for food, water, bathing, wallowing in mud | Bush farm and water | Search for food and water, hunting and trapping, slaughtering. |
| Bush cat | Bush, town, and farms | Search for prey, food, and water | Farms, bush, water points, and cooking places where fish and other animals are dried. | Search for food, trap, hunting walking in the bush. |
| Pumpkin Pine | . Bush farms, grassland, the forest along rivers and streams | Search for food, farms, and holes along river banks | Farm, bush, the forest along rivers and holes. | A search for food, traps, hunting, slaughtering |
| Chimpanzee | ||||
| Giant Rat | Bush, farms | Searching for food | Bush, town, farm huts | Searching for food, trapped, hunted, pets, consumed, processing |
| Mongoose | Bush, farms | Search for food, | Bush, farms, town, and homes | Searching for food, pets, trapping, and hunting |
| Rabbit | Bush | Search for food | Bush, farms, homes | Pets, trap, hunting, and butchering |
| Tiger | Bush | Search for prey, drinking water | Bush | Trap, hunting, and pets |
| Bush goat | ||||
| Royal Antelope | Bush | Search for food and water | Bush | Trap, walking along the same track in bush, hunting, trapping, and pets. |
| Tree Squirrel | Bush | A search for food and as prey for other animals | Bush | Crossing the road, trap, and pets, hunting. |
| Diaka | Bush water points and farms | A search for food and water | Bush | Search for food, trap and hunting and pets |
| Muscat | Bush, farms water points | Search for prey and water | Bush, town, farm huts | Searching for food, hunting, trapping, processing |
| Elephant | Bush | Search for food | Bush and town | Pets, trapping, hunting, and slaughtering. |
| Buffalo | Bush and watering pointing | Search for food, | Bush | Trapping and hunting |
| Squirrel | Bush, road, farms | Searching for food and prey for other animals | Bush, farm on the road | Searching for food, trapping, hunting, and slaughtering |
| Rat | Bush, farms, and town | Food and shelter | Bush town and farm | Search for food |
| Folding animal | ||||
| Snake | Bush, town, and farms | Searching for food and accommodation | House, village, farm, and bush | Foraging for food, accommodation |
| Bats | Bush, towns, and farms | Food | Town, caves, trees, fruits, farms, and bush | Food, guano, eating bats, eating leftovers, hunting, trapping, and playing with bats. |
| Grasscutter | Bush and Town | Searching for food | Bush, town, and farm | Pets, food, trapping and hunting, sales for income, and slaughtering. |
| Monkey | Bush Town and farm | Search for food | Bush, town farms, and homes | Search for food; humans hunt monkeys for food and pets, trap and hunt, sell to make income, and eat. |
| Leopard | Bush | Hunt domestic animals as prey | Bush | I worked in the bush and looked for domesticated animals in the bush and town. |
| Ndandakui | Bush, farm, and town | Hunt domestic chicken as prey | Farm and town | I am looking for poultry birds through trapping and hunting. |
| Stone goat | ||||
| Gorilla | Bush and town | Search for food, walking on the same path with other animals eating the same food. | Bush | Man-eating their leftovers are working in the bush through hunting and trapping. |
| White wolf | Bush | Search for domesticated animals as prey | Bush, farms, and town | We are looking for domestic animals as prey, feeding in a garbage dump, trapping, and hunting. |
| Hyena | Bush, town, and farms | Search for domesticated animals as prey | Bush, town, and farm | Looking for target, hunting, and trapping |
| Lion | Bush and town | Search for domesticated animals as prey | Bush and farm | Trapping and hunting, slaughtering and eating |
| Deer | Bush, town, and farms | Searching for food and wild animals looking for prey. | Bush and town | They search for food, trapping, hunting, pets, butchering, selling, and eating. |
| Hippopotamus | Bush | Bush and water | bush | Searching for food, trapping, hunting, butchering, and eating |
Table 4: Wildlife-domestic animal and human interaction that may lead to disease transfer and spread.
Discussion
Animal Health Clubs complement the efforts of Human health, environment, and veterinary services in Sierra Leone, particularly in hard-to-reach communities. Animal Health club brings and unites people to restore peace and security, leading to improved health, livelihood, food, and human safety. People formulate bye-laws that bind them to achieve the common good for their villages and town. Community Conflict is reduced as they work for the common good or mutual benefits.
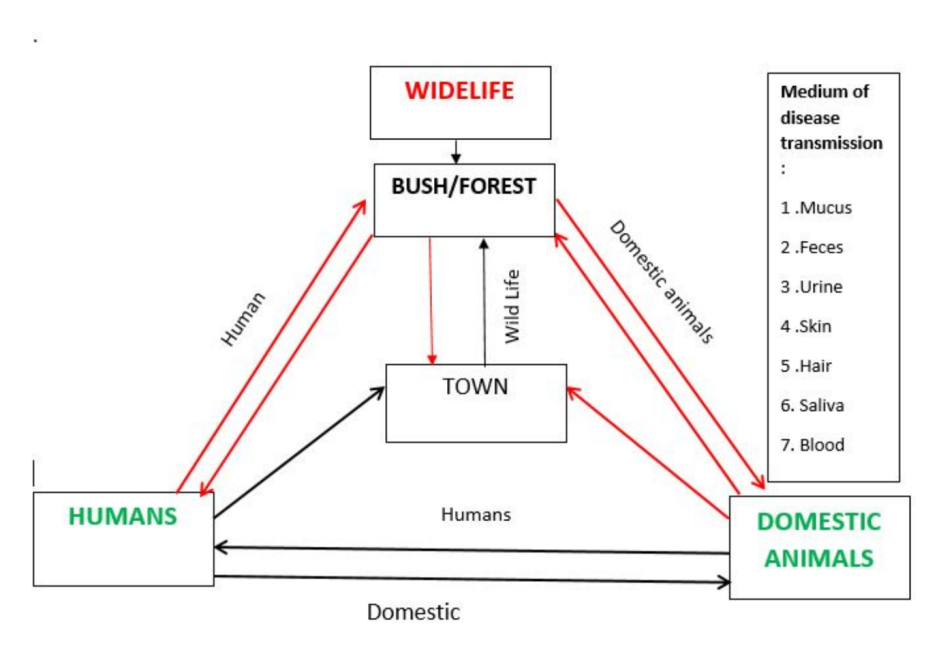
The Animal Health club team first identified sentinel sites with diversified wildlife and a high level of animal- human interaction [5, 13]. The club engaged communities in focus group discussions to identify domestic and wildlife (Table 1), diseases associated with these animals (Tables 2 & 3), and the point of interaction between domestic, wildlife, and humans, as seen in Figure 2 & Table 4. Sources of infection identified include toilets, Garbage dumps, water, crops, humans, pets and wildlife, Ruminants, and poultry [14]. The AHC team and community people list these animals and the likely zoonotic diseases (Tables 2 & 3). Indigenous people, hunters, and farmers provided this vital information. Zoonotic diseases which pose a threat to the communities were selected. The team developed a manual containing all these diseases with signs and symptoms to train people on disease surveillance in their communities [15].
Executive members were selected and appointed to establish the surveillance system. The executive committee divides the towns or villages into zones depending on the size. The people or committee nominate or select the zonal heads, who appoint people in each zone. Animal Health Club trains them on passive and active surveillance, including syndromic, evident-based management, integrated, and categorical surveillance. In this case, every community becomes a sentinel site. Nine trained people in each zone are appointed for two weeks to watch the nine sources of diseases in their zones and report to the zonal head daily. The zonal head collates and sends information generated to the chairman, who sends it to the town chief. They scrutinize the information received before submitting it to the relevant authorities in Ministries of Agriculture and health or nongovernmental organizations working with animals and humans in their areas, as in Figure 1.
Community people affirmed that multiple factors drive the point of interaction between domestic animals, wildlife, and humans. Thirgood, et al. [16] stated that various social factors allow humans and wildlife to interact across different landscapes. One such factor is their social hierarchy of needs, including food or prey, shelter, health, and recreation. Man and animals (domestic and wild) search for what they can eat daily, herbs to cure themselves when sick, and look for places to sleep and exercise when fed. Another indirect contact is when they ran into traps, hunted by hunters, and chased by wild animals.
Domestic animals search for food and come into contact with wildlife or, by walking in the same path, touch their saliva, feces, mucus, urine, or hair and blood. They contract diseases from the wild animals in the bush and come to town through this interaction. In some instances, they fight with wildlife and contract diseases. Domestic animals interact directly with humans by catching and putting them into pens or houses, feeding and playing with them. Indirectly, domestic animals lie in places where the humans sit, drink the same water, and lick their utensils. In this way, domestic animals transfer diseases to men and other animals in the community.
Wildlife animal interacts with domestic animals as above. Wildlife animals come to towns to catch domestic animals as prey. They fight with domestic animals, rub their saliva, mucus, hair, or blood on the animals or spill their shed blood on the ground. They may also defecate or urinate in towns. Humans and domestic animals step on the feces and urine, thereby contracting diseases. Humans, in turn, go to the bush to farm, find food, set a trap, hunt, and walk. Contact the urine, feces, and mucus hair of wildlife and walk in their path. Sometimes, they catch wildlife in their traps, touching them directly. Man, in turn, returns and connects with humans and domestic animals, thereby transferring diseases contracted from the wild.
Man contracts diseases from these sources and transfers them to the wild, domestic, and human beings. Community people have been able to name some of these animals and the likely zoonotic diseases associated with them, as seen in Tables 2 & 3 for a list of animals and conditions related to these animals. There is, therefore, a high level of interaction between humans and humans than between domestic and wildlife. During the focus group discussions, the community people confirmed this statement by reiterating that the human-to-human transfer of diseases is more than that of human-to-animals. This statement was evident during the Ebola crisis in 2013.
Animal Health Club is needed to fight disease outbreaks and use it as a surveillance tool to control and prevent diseases in rural communities. People will not conceal important information as they are an integral part of every activity and stage of disease surveillance in the community. Villages or towns should be motivated, as work is voluntary. Such motivating incentives include vegetable seeds and livestock that the community can raise and use proceeds to develop their communities—the clubs work with the communities to establish surveillance systems. The club’s constant attention and vigilance reduce disease incidence, morbidity, and mortality.
Conclusion
Animal Health Club brings people together in a town or village to achieve a common goal and objective. Such unity increases peace and security in the community and improves health, livelihood, food, and human safety, in a cheap, long- lasting, and self-sustainable manner. Establishing sentinel sites in hard-to-reach communities utilizes the rich indigenous knowledge and native intelligence of rural people to identify domestic and wild animals, diseases associated with these animals, and how infection transfers from humans, animals, and wildlife. Training rural communities on the wealth of knowledge obtained to establish surveillance systems will increase their understanding of disease control and prevention in their environment, thus protecting their animals, wildlife, environment, and themselves from high morbidity and mortality.
Contributors
All authors contributed to writing subsequent drafts, editing, and approving the final manuscript.
Declaration of Interests
We declare no competing interests
Acknowledgement
Thanks to the country representative of the United Nations Food and Agricultural Organization of Sierra Leone, Dr. Gabriel Ragalema, and program manager David Mwesigwa who provided the fund to identify how people contract Disease. Special thanks to all the staff in the Freetown office who, in diverse ways, supported the work. The team also acknowledges the valuable contributions of the rural people of Sierra Leone who provide the information contained in this manuscript. The researchers are grateful to all Njala University One Health Serology and Molecular Diagnostic Laboratory staff, who assisted in the pretesting of the questionnaire.
References
-
Cleveland S, Sharp J, Abela-Ridder B, Allan KJ, Buza J, et al. (2016) One Health contribution towards more effective and equitable approaches to health in low and middle-income countries. Philos Trans R Soc Lond BBiol Sci 372(1725): 20160168.
-
Welburn SC, Beange I, Ducrotoy MJ, Okello AL (2015) The neglected zoonotic-the case for integrated control and advocacy. Clin Microbiol infect 21: 433-443.
-
Maudlin I, Eisler MC, Welburn SC (2009) Neglected and endemic zoonoses. Philos Trans R Soc Lond B Biol Sci 364: 2777-2287.
-
Anthony J McMichael (2015) Extreme weather events and infectious disease outbreaks Virulence. 6(6): 543- 547.
-
Ogunkola IO, Adebisi YA, Imo UF, Odey GO, Esu E, et al. (2020) Rural communities in Africa should not be forgotten in responses to COVID-19. Int J Health Plann Manage 35: 1302-1305.
-
World Bank (2020) Sierra Leone-Rural Population Trading Economics.com.
-
Katherine EL, Tonks W, Bender JB, Deem SL, Ferguson AW, et al. (2022) Strengthening global health security by improving disease surveillance in remote rural areas of low-income and middle-income countries. Global health 10(4): 579-584.
-
Sierra Leone Multidimensional Poverty Index 2019. pp: 1-44.
-
Ouma PO, Maina J, Thuranira PN, Macharia PM, Alegana VA, et al. (2015) Access to emergency hospital care provided by the public sector in sub-Saharan Africa in 2015: A geocoded inventory and spatial analysis. Lancet Glob Health 6: e342-e350.
-
Strasser R, Kam SM, Regalado SM (2016) Rural Health Care Access and Policy in Developing Countries. Ann. Rev. Public Health 37: 395-412.
-
Rutherford ME, Mulholland K, Hill PC (2010) How to access to health care relates to under-five mortality in sub-Saharan Africa: Systematic review. Trop Med Int. Health 15(5): 508-519.
-
(2020) Human Development Reports. Sierra Leone.
-
(2017) Ministry of Health and Sanitation, Republic of Sierra Leone. National Health Sector Strategic Plan 2017-2021.
-
Morse SS, Mazet JAK, Woolhouse M (2012) Prediction and prevention of the next pandemic zoonosis. Lancet 380: 1956-1965.
-
Suluku R (2016) Procedures in implementing Animal Health Clubs in Rural Sierra Leone. Published by Animal Health Club.
-
Thirgood S, Woodroffe R, Rabinowitz A (2009) The Impact of Human-Wildlife Conflict on Human Lives and Livelihoods. In: Woodroffe R., Thirgood S, Rabinowitz A, et al. (Eds.), People and Wildlife: Conflict or Coexistence? Cambridge University Press, Cambridge, UK, pp: 13-26.
- California Red-Legged Frog and Non-Listed Amphibians Response to Non-Native Fish Removal
- Industrial Standardization of the Bio-OS: Algorithmic Codification of Resilience Engineering Guidelines and Version V8 Architecture
- Climate Variability and the Sustainability of Snail Farming in Nigeria: Past Trends, Present Challenges and Potential Outlook
- The Evaluation of the Surveillance System of Anthrax in Gilgit-Baltistan, Pakistan, 2018
- Natural Decline to Extinction of A New Zealand Rabbit Population
- Mitochondrial Bio-Logistics: Steering Co-Enzyme Q10 and Lycopene Synergies within the Science 4.0 Bio-OS Framework