Epidermolysis Bullosa. A Rare Disturbance in Clinical Veterinary of Felines
Epidermolysis bullosa is an inherited group of rare genetic dermatosis characterized by mucocutaneous fragility and blister formation, inducible by often minimal trauma. Epidermolysis bullosa is described in humans and domestic animals, and this dermatosis in humans is classified in four categories based predominantly on the plane of skin cleavage in simplex epidermolysis bullosa, junctional epidermolysis bullosa, dystrophic epidermolysis bullosa and Kindler epidermolysis bullosa. In veterinary medicine the classification of epidermolysis bullosa is based in the human classification the according with the level of ultrastructural separation of skin. The epidermolysis bullosa in cats is a rare disease with a description of isolated cases involving the forms simplex, junctional and dystrophic. The laboratory diagnosis of cats under suspicion of epidermolysis bullosa should include dermo histopathology, transmission electron microscopy, immunofluorescence for antigen mapping and when possible, mutation analysis. There is no specific treatment for epidermolysis bullosa in cats, and care is palliative. The few case reports of epidermolysis bullosa in cats indicates a short time of survival with few months to years, being the cats sacrificed or dying during the first months of life. Due to these factors, it is essential the deep studies of disease in cats so that they can present an increase in expectancy and quality of life.
Introduction
Epidermolysis bullosa corresponds a group of genetic diseases characterized by mechanical fragility of tissues leading to formation of mucocutaneous blisters, erosion and ulceration secondary to trauma. The blisters can be localized or generalized, affecting different parts of the body, from limbs to the oral cavity [1]. In humans, epidermolysis bullosa have worldwide occurrence, affecting both sexes in equal proportion, and its incidence varies from 3.8 to 35/1 million live births [2]. In pets, the frequency of epidermolysis bullosa is not known or estimated, and in cats it is recognized as a rare disease with few isolated cases described.
Microscopic Structure of Skin
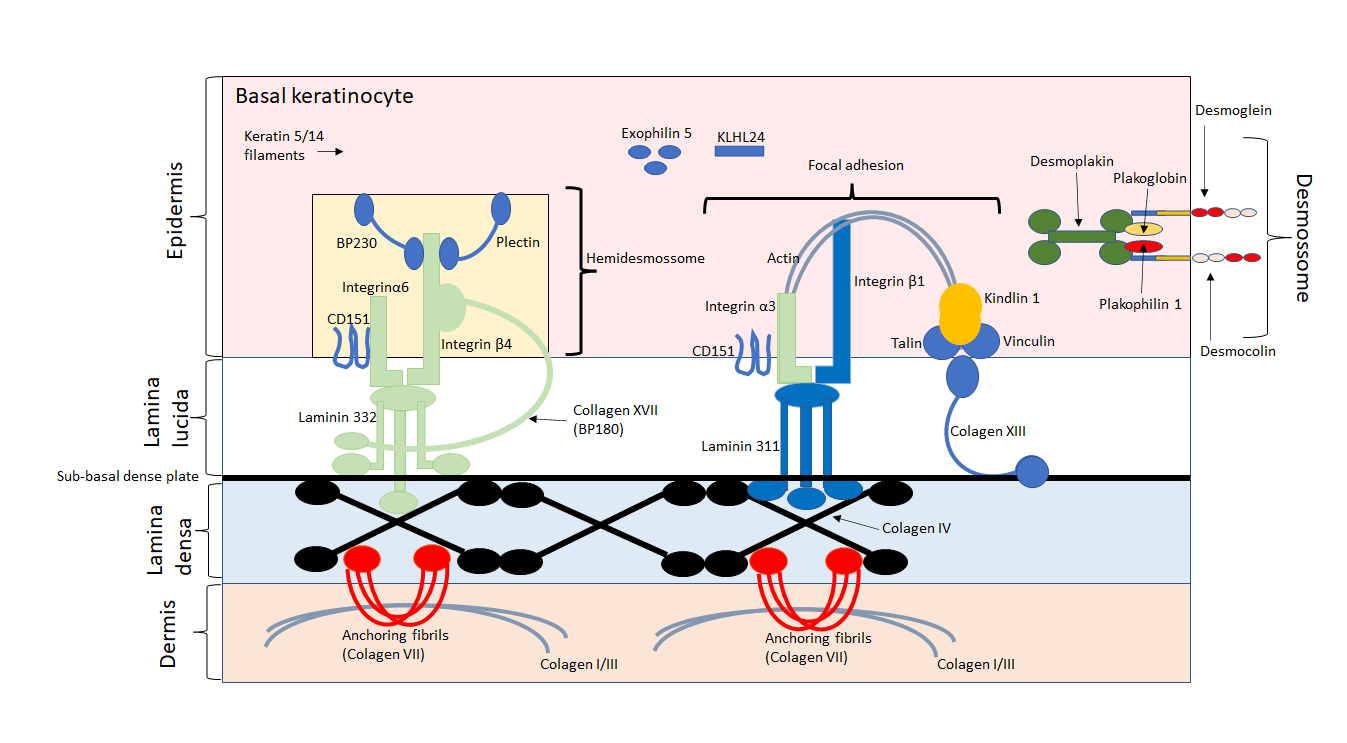
The skin is considered the large organ in the body of humans and animals, being formed by the epidermis and dermis layers. Between the epidermis and dermis is located the basement membrane, responsible for the adhesion of epidermis to dermis [3]. The basement membrane is formed by two structures, lamina lucida and lamina densa. Above the lamina lucida are present the intermediate filaments (composed by keratin 5 and 14), and an intracellular network that links the cytoskeleton of basal cells to the hemidesmosomes (formed by the inner plate and outer plate) in the keratinocyte basement plasma membrane [4].
The anchoring filaments connect the hemidesmosomes (formed by the proteins plakoglobin, placophyllin, desmoplakin; and the cadherins desmocolin and desmogelin) the lamina densa, and anchor the fibrils across the lamina lucida [5].
The inner plate of hemidesmosomes is composed by the proteins HD1/plectin and BP230, and is connected to the intermediate filaments inside the cytoplasm of basal keratinocytes. The outer plate of hemidesmosomes is composed of integrin α6β4 and BP180. The lamina lucida is formed by the plasmatic membrane, sub-basal plate and anchoring filaments (composed of collagen XVII and laminin 332), and the lamina densa is formed by type IV collagen [6]. The type VII collagen present in anchoring fibrils extends from the lamina densa towards the papillary dermis and combines with interstitial collagen fibrils in the dermis, promoting skin support [7] (Figure 1).
Classification of Epidermolysis Bullosa
Epidermolysis bullosa can be of genetic or autoimmune origin, being classified as hereditary epidermolysis bullosa or acquired epidermolysis bullosa [8]. The hereditary epidermolysis bullosa has different phenotypes because the different genetic mutations caused by inherance autosomal dominant or recessive that cause structural changes and fragility of the cytoskeleton of basal keratinocytes or basement membrane [9]. The acquired epidermolysis bullosa no has genetic transmission, being of an autoimmune nature, where the production of IgG autoantibodies against collagen VII that make the anchoring fibrils [10]. Current, the acquired epidermolysis bullosa is included in the group of autoimmune subepidermal bullous diseases [1].
In veterinary medicine the classification of epidermolysis bullosa is based on the human classification according to the level of ultrastructural separation of skin [11]. The according with the layer skin involved, epidermolysis bullosa is classified into simple epidermolysis bullosa, junctional epidermolysis bullosa, dystrophic epidermolysis bullosa, and Kindler’s epidermolysis bullosa [1, 8, 9].
Although skin fragility is greater in humans, it is less reported in pets, probably due to the presence of hairs that act as mechanical barrier and promote the anchoring of dermis to the epidermis because the invagination of hair follicles [11, 12].
Simplex Epidermolysis Bullosa
The simplex epidermolysis bullosa corresponds to 70% of all cases in humans and is usually as inherited in an autosomal dominant manner, with some rare autosomal recessive forms [1]. The mutations involved in simplex epidermolysis bullosa affect proteins that provide structural support and cohesion of stratified epithelium, in particular of epidermis [1, 2]. In domestic animals, this is apparently the most common form [11].
In humans, the most common mutations involve KRT5 gene (encodes keratin 5) and KRT14 gene (encodes keratin 14) involved in the formation of intermediate filaments and cytoskeleton of basal keratinocytes. Mutations of these genes lead to a reduction in the mechanical rigidity of the keratinocyte cytoplasm, increased sensitivity to mechanical stress and weakening of desmosome adhesion. Also, mutations in PLEC gene (encodes plectin) compromises the formation of intermediate filaments [1].
Genes encoding hemidesmosome proteins that anchor keratin filaments to the plasma membrane, such as DSP (desmoplakin), JUP (plakoglobin junction), PKP1 (plakophilin 1), PLEC (plectin) and DST (dystonin) are also associated with cases of simplex epidermolysis bullosa, as well the EXPH5 gene (exophilin 5) leading to disruption of intracellular vesicle trafficking along actin and tubulin networks and loss of basal keratinocyte adhesion. The mutations of KLHL24 gene cause increase of keratin degradation leading to cytoskeleton collapse, tissue cohesion and cellular resilience under stress conditions [9].
In domestic animals, clinical signs appear early after birth, with detachment of the epidermal layers under pressure, and development of deformity of hooves or claws. When occur basal separation with cytolysis of basal cells, ulcers may form on the gingiva, palate, oral mucosa and dorsum of the tongue [11].
Classically the histology of simplex epidermolysis bullosa is characterized by intraepidermal cleavage without cytolysis of basal cells. Microscopic changes are seen below epidermis with intraepidermal blister formation and vacuolar changes in the layer of epidermal basal cell [9].
Recently Dettwiler et al. described the first case report of simplex epidermolysis bullosa in a domestic cat with a history of desquamation of the paw pads and ulcerations in the oral cavity and inner surface of the ear. Clinical and histopathological findings indicated a congenital disease with the formation of blisters inside layer of basal cell of epidermis and epithelium of oral mucosa. Genetic sequencing revealed a homozygous nonsense variant in the KRT14 gene (c.979C>T, p.Gln327*) and the mapping of antigens by immunohistochemistry indicated the absence of keratin 14 staining of biopsied tissues [13].
Junctional Epidermolysis Bullosa
In humans the junctional epidermolysis bullosa has both an autosomal dominant and recessive pattern of inheritance, microscopically characterized by cleavage of lamina lucida from the basement membrane [9]. In humans the junctional epidermolysis bullosa is molecularly heterogeneous resulting from biallelic mutations of genes that encode proteins involved in anchoring of basal keratinocytes to the basement membrane, such as COL17A1 gene (encode type XVII collagen that constitutes desmosomes), LAMA3, LAMB3 and LAMC2 gene (encodes laminin 332 that forms the anchoring filaments of lamina lucida), ITGA6 and ITGB4 genes (encodes α6β4 integrin of desmosomes) and IGTA3 gene (encodes the subunit α3 of β1 integrin responsible by focal adhesion of basal keratinocytes) [1].
In cats the clinical manifestations of junctional epidermolysis bullosa includes the formation of ulcers in the skin and oral cavity (Figures 2A-C).
![Figure 2: Clinical manifestation of junctional epidermolysis bullosa in Brazilian short hair kitten with 5 months of age. A. Palate ulceration. B. Skin ulcer secondary to physical friction trauma in the dorsal thoracic region. C. Skin suture in the left thoracic region after self-inflicted trauma. Font: Errante, et al. [14].](/fulltextimages/8776/fig_2.png)
In the histopathological evaluation of the skin, cleavage occurs inside the lamina lucida of basement membrane, which is joined to the floor of cleft (Figures 3A&B), and ultrastructural changes can be seen in desmosomes and anchoring filaments (Figure 3C) [14].
![Figure 3: Histopathological examination of skin. A. Dermal-epidermal separation area. The epidermis is detached from the dermis, forming subepidermal fissures. Presence of neutrophils dispersed in the superficial and deep dermis. H/E staining, 10X objective. B. Dermo-epidermal separation forming a vesicle with cleavage in the basement membrane region. The basement membrane remains at the base of the vesicle attached to the dermis. PAS staining, 40X objective. C. Transmission electron micrograph of the skin. Cleavage of anchor filaments (arrow) attached to not well defined hemidesmosomes. Font: Errante, et al. [14].](/fulltextimages/8776/fig_3.png)
Figure 3: Histopathological examination of skin. A. Dermal-epidermal separation area. The epidermis is detached from the dermis, forming subepidermal fissures. Presence of neutrophils dispersed in the superficial and deep dermis. H/E staining, 10X objective. B. Dermo-epidermal separation forming a vesicle with cleavage in the basement membrane region. The basement membrane remains at the base of the vesicle attached to the dermis. PAS staining, 40X objective. C. Transmission electron micrograph of the skin. Cleavage of anchor filaments (arrow) attached to not well defined hemidesmosomes. Font: Errante, et al. [14].
Alhaidari, et al. described a case report involving two kittens who had ear lesions, oral ulceration and onychomadesis (nail detachment from the proximal extremity). Histopathology showed the presence of subepidermal separation with union of the lamina densa to the floor of vesicles and antigen immunomapping indicated alteration in the g2 subunit of laminin in one case, and alteration of β3 subunit of laminin in the other case [12].
Dystrophic Epidermolysis Bullosa
In humans the dystrophic epidermolysis bullosa can be inherited in an autosomal dominant or recessive form, and the severity of lesions depends if the lesions are localized or generalized [1]. In dystrophic epidermolysis bullosa, mutations in the COL7A1 gene (encodes collagen VII) causes qualitative/quantitative alteration of type VII collagen, with formation of rudimentary fibrils and alteration in the number of anchoring fibrils in the dermo-epidermal junction. Microscopically, dermo-epidermal separation is observed below the sublamina densa due to cleavage occurring below the basal lamina [9].
Dystrophic epidermolysis bullosa was diagnosed in an 8-month-old male domestic shorthaired cat with skin ulceration, mucous membranes and onychomadesis. The histology of lesions indicated a dermal-epidermal separation, the immunohistochemistry showed the presence of collagen IV located at the roof of the cleft at both the dermal- epidermal and follicular-dermal interfaces, and electron microscopy showed presence of cleft in the sublamina densa of dermal-epidermal junction [15]. In other case report, dystrophic epidermolysis bullosa was diagnosed in a kitten with epithelial sloughing of oral mucosa, footpads and skin. Histopathology of skin demonstrated a dermo epidermal separation, and ultrastructural microscopy the presence of anchoring fibrils exhibited filaments with alteration in morphology and number [16].
Kindler Epidermolysis Bullosa
In humans Kindler epidermolysis bullosa is an autosomal recessive disease caused by a mutation in the FERMT1 gene that encodes the kindlin-1 protein. This kind of epidermolysis bullosa is characterized by the development of acral blisters in infancy, photosensitization, poikiloderma, and progressive skin atrophy [1]. Microscopic ultrastructural changes reveal a reduplication of the basement membrane and many types of cleavage in the dermal-epidermal junction (inside basement membrane, along the lamina lucida or below the lamina densa) consequence of alterations in the keratinocyte cytoskeleton network, and loss adhesion of keratinocyte integrins to basement membrane [1, 8]. No case report associated with Kindler epidermolysis bullosa has been reported in cats until the moment.
Diagnosis
Skin diseases are uncommon in cats and their diagnosis can be a challenge for the small animal veterinarian, since felines have a limited number of patterns of skin response to different pathologies. A suspicion of epidermolysis bullosa should be taken into account when newborn or young animals have blisters and/or erosions on the skin and mucous membranes secondary insignificant mechanical trauma [11, 14].
Laboratory diagnosis of histological lesions under light microscopy, routine practice for skin analysis with detachment of the epidermis from the dermis requires confirmation by transmission electron microscopy, immunofluorescence for antigen mapping and mutation analysis [11, 12, 13, 14, 15, 16]. Electron microscopy and immunofluorescence for antigen mapping allow the determination of the level of skin cleavage, which can be intraepidermal, intralamina lucida or sublamina densa [11, 15, 16]. The electron microscopy allows visualization of specific structures such as keratin filaments, desmosomes, hemidesmosomes, dense sub-basal plates, anchoring filaments and anchoring fibrils [11, 14]. The immunofluorescence provides information about the type of epidermolysis bullosa and which structural proteins are altered [16]. The search for mutations through DNA sequencing is important to determine the mode of inheritance and the mutation, playing a fundamental role in the identification of the mode of inheritance and of animals carrying these genes [11, 13].
Unfortunately, few veterinary laboratories have the capacity and experience to diagnose epidermolysis bullosa in pets. Consequently, skin examination of animals with epidermolysis bullosa can lead to misdiagnosis. The transmission electron microscopy, immunofluorescence antigen mapping and mutation analysis are usually performed at reference centers in public universities in developing countries such as Brazil.
Treatment
There is no specific treatment for epidermolysis bullosa in pets, especially in cats. Care is palliative and includes the prevention of trauma and blisters through nail clipping to protect the skin from friction, prevent infections and fluid loss. Control of ectoparasites such as fleas is essential to avoid self-trauma [14].
In the presence of small lesions, the use of antimicrobial ointments is recommended, but they do not present encouraging results [12]. In cases of extensive wounds, the application of sutures and the use of systemic antibiotics are necessary [14, 15]. In animals affected by stomatitis, antibiotic therapy has a partial effect [12].
Cats with epidermolysis bullosa have a short survival rate of a few months to years, being euthanized or dying during the first few months of life [11, 12, 14].
Conclusion
Since skin diseases are uncommon in cats and their clinical manifestations are restricted to a limited number of patterns, the diagnosis of epidermolysis bullosa is a challenge for the small animal veterinarian. In cats, three types of epidermolysis bullosa have been described, simplex, junctional and dystrophic. Unfortunately, few veterinary laboratories have the capacity and experience to perform the diagnosis of epidermolysis bullosa. Transmission electron microscopy, immunofluorescence antigen mapping and mutation analysis are usually performed at reference centers in public universities in developing countries, limiting their access. Currently, there is no specific treatment for cats affected by this disease, whose clinical management consists of protecting the skin from friction and preventing infections.
References
-
Bardhan A, Bruckner Tuderman L, Chapple ILC, Fine JD, Harper N, et al. (2020) Epidermolysis bullosa. Nat Rev Dis Primers 6: 78.
-
Fine JD (2016) Epidemiology of inherited epidermolysis bullosa based on incidence and prevalence estimates from the National Epidermolysis Bullosa Registry. JAMA Dermatol 152: 1231-1238.
-
Souci L, Denesvre C (2021) 3D skin models in domestic animals. Vet Res 52: 21.
-
Moreci RS, Lechler T (2020) Epidermal structure and differentiation. Curr Biol 30: R144-R149.
-
Pora A, Yoon S, Windoffer R, Leube RE (2019) Hemidesmosomes and focal adhesions treadmill as separate but linked entities during keratinocyte migration. J Invest Dermatol 139: 1876-1888.e4.
-
Bruckner-Tuderman L, Has C (2014) Disorders of the cutaneous basement membrane zone-The paradigma of Epidermolysis bullosa. Matrix Biol 33: 29-34.
-
Tsutsui K, Machida H, Nakagawa A, Ahn K, Morita R, et al. (2021) Mapping the molecular and structural specialization of the skin basement membrane for inter- tissue interactions. Nat Commun 12: 2577.
-
Mariath LM, Santin JT, Schuler Faccini L, Kiszewski AE (2020) Inherited epidermolysis bullosa: update on the clinical and genetic aspects. An Bras Dermatol 95: 551- 569.
-
Has C, Fischer J (2019) Inhereited Epidermolysis bullosa: new diagnostics and new clinical phenotypes. Exp Dermatol 28: 1146-1152.
-
Kridin K, Kneiber D, Kowalski EH, Valdebran M, Amber KT (2019) Epidermolysis bullosa acquisita: A comprehensive review. Autoimmun Rev 18: 786-795.
-
Medeiros GX, Riet Correa F (2015) Epidermolysis bullosa in animals: a review. Vet Dermatol 26: 3-13.
-
Alhaidari Z, Olivry T, Spadafora A, Thomas RC, Perrin C, et al. (2005) Junctional epidermolysis bullosa in two domestic shorthair kittens. Vet Dermatol 16: 69-73.
-
Dettwiler M, Leuthard F, Bauer A, Jagannathan V, Lourenço AM, et al. (2020) A nonsense variant in the KTR14 gene in a domestic shorthair cat with epidermolysis bullosa simplex. Anim Genet 51: 829-832.
-
Errante PR, Silva PTD (2015) Epidermolysis bullosa in a Brazilian shorthair kitten. Revista CFMV 65: 67-72.
-
White SD, Dusntan RW, Olivry T, Naydan DK, Richter K (1993) Dystrophic (dermolytic) epidermolysis bullosa in a cat. Vet Dermatol 4: 91-95.
-
Olivry T, Dunson SM, Marinkovich MP (1999) Reduced anchoring fibril formation and collagen VII immunoreactivity in feline dystrophic epidermolysis bullosa. Vet Pathol 36: 616-686.
- California Red-Legged Frog and Non-Listed Amphibians Response to Non-Native Fish Removal
- Industrial Standardization of the Bio-OS: Algorithmic Codification of Resilience Engineering Guidelines and Version V8 Architecture
- Climate Variability and the Sustainability of Snail Farming in Nigeria: Past Trends, Present Challenges and Potential Outlook
- The Evaluation of the Surveillance System of Anthrax in Gilgit-Baltistan, Pakistan, 2018
- Natural Decline to Extinction of A New Zealand Rabbit Population
- Mitochondrial Bio-Logistics: Steering Co-Enzyme Q10 and Lycopene Synergies within the Science 4.0 Bio-OS Framework