Case Report of Follow-up about a Yorkshire Dog with Multinodular Bone Tumor with Development of Pulmonary Metastasis
The multinodular bone tumor is a slow-growing, locally invasive malignant tumor capable of metastasizing. Its occurrence is greater in the flat bones of the skull and hard palate. The clinical signs depend on the location of tumor and are generally related to compression of adjacent structures. This report describes the follow-up of a case of multinodular bone tumor in a currently thirteen-year-old dog, Yorkshire Terrier breed, which was initially treated with neoformation in a region overlapping the topography of the left zygomatic arch and the caudal portion of the left mandibular branch. After performing a skull radiographic evaluation, computed tomography and laboratory investigation, surgical removal and histopathological examination were performed, which confirmed the suspicion of a multinodular bone tumor. Two years after surgery, pulmonary metastasis was found on the left side of the lung. At the time of this publication, the animal is in good general condition and without respiratory symptoms, despite progressive metastatic growth.
Introduction
Multilobular bone tumor is a slow-growing, locally invasive bone neoplasm with malignant potential and a high rate of recurrence and the ability to metastasize. It occurs more frequently in dogs of medium or large breeds and rarely in giant and small breeds, being more common in middle-aged to elderly animals [1]. This bone tumor recurs locally after surgical excision, in addition to having the ability to metastasize to distant tissues such as lungs [2, 3]. The diagnosis of this tumor is defined using imaging tests, including radiography, computed tomography and magnetic resonance imaging, which are also fundamental in surgical planning [4].
Histologically, the multilobular bone tumor presents a mass with well-defined lobes containing osteoid and cartilage separated by fibrovascular septa. These lobes have a trilaminar appearance formed by islands of bone or mineralized cartilage circumscribed by ovoid or elongated cells, delimited by peripheral areas of fibrosis [4, 5, 6].
A canine animal, female, Yorkshire Terrier breed, in 2019, aged nine years old, was seen at a private clinic located in São Paulo, SP, Brazil, with a history of increased volume superimposed on the topography of the left zygomatic arch and caudal portion. Of the left mandibular branch (Figure 1A). At the time of the first consultation, radiographic examination of the skull and chest, computed tomography of the skull and chest, electrocardiogram, echocardiography, blood count and serum biochemistry were requested with assessment of serum levels of alanine aminotransferase, alkaline phosphatase, urea, creatinine, albumin and total proteins.
The radiographic examination revealed marked bone proliferation of high radiopacity, with an irregular and amorphous appearance superimposed on the topography of the left zygomatic arch and the caudal portion of the left mandibular ramus (Figure 1B). On computed tomography, the presence of multilobulated amorphous bone proliferation was verified (Figure 1C & 1D). Before surgery, three-view chest radiographs were performed to assess whether metastatic disease was present, with results within normal limits.
![Figure 1: A) Macroscopic appearance of the volume increase on the topography of left zygomatic arch and caudal portion of left mandibular ramus. B) Ventrodorsal radiographic evaluation. Presence of irregular and amorphous bone proliferation superimposed on topography of left zygomatic arch and caudal portion of left mandibular ramus. C) Computed tomography. Presence of amorphous, multilobulated bone proliferation (regular margins and defined limits, affecting the left zygomatic arch measuring 4.7cm in the rostrocaudal axis, 2.8cm in the dorsoventral axis and 2.1cm in the lateral axis). D) Computed tomography. 3D reconstruction of images obtained from the neoformation. Font: [4].](/fulltextimages/11812/fig_1.png)
Figure 1: A) Macroscopic appearance of the volume increase on the topography of left zygomatic arch and caudal portion of left mandibular ramus. B) Ventrodorsal radiographic evaluation. Presence of irregular and amorphous bone proliferation superimposed on topography of left zygomatic arch and caudal portion of left mandibular ramus. C) Computed tomography. Presence of amorphous, multilobulated bone proliferation (regular margins and defined limits, affecting the left zygomatic arch measuring 4.7cm in the rostrocaudal axis, 2.8cm in the dorsoventral axis and 2.1cm in the lateral axis). D) Computed tomography. 3D reconstruction of images obtained from the neoformation. Font: [4].
The material obtained after surgery was sent for histopathology. The microscopic examination of sections revealed presence of mesenchymal proliferation with expansive growth, sections forming lobular outlines delineated by bundles of spindle cells. Inside the lobes, an atypical cartilaginous component, areas of ossification and few foci showing immature osteoid matrix were observed.
The tumor cells appeared fusiform or rounded in appearance, with round to oval nuclei (Figures 2A & 2B).
Based on these results, the diagnosis of multilobular bone tumor was established, and the tutor was recommended to periodically reevaluate the dog for possible local recurrence of the tumor or emergence of metastases.
![Figure 2: Histopathology. A. Mesenchymal proliferation with expansive growth, with stretches forming lobular outlines delineated by bundles of fusiform cells. Inside the lobes, presence of atypical cartilaginous component, areas of ossification and foci with immature osteoid matrix (Hematoxylin/Eosin stain, 4x magnification). B. Presence of tumor cells with a fusiform or rounded appearance, with rounded to oval nuclei (Hematoxylin/Eosin stain, 40x magnification). Font: [4].](/fulltextimages/11812/fig_2.png)
Figure 2: Histopathology. A. Mesenchymal proliferation with expansive growth, with stretches forming lobular outlines delineated by bundles of fusiform cells. Inside the lobes, presence of atypical cartilaginous component, areas of ossification and foci with immature osteoid matrix (Hematoxylin/Eosin stain, 4x magnification). B. Presence of tumor cells with a fusiform or rounded appearance, with rounded to oval nuclei (Hematoxylin/Eosin stain, 40x magnification). Font: [4].
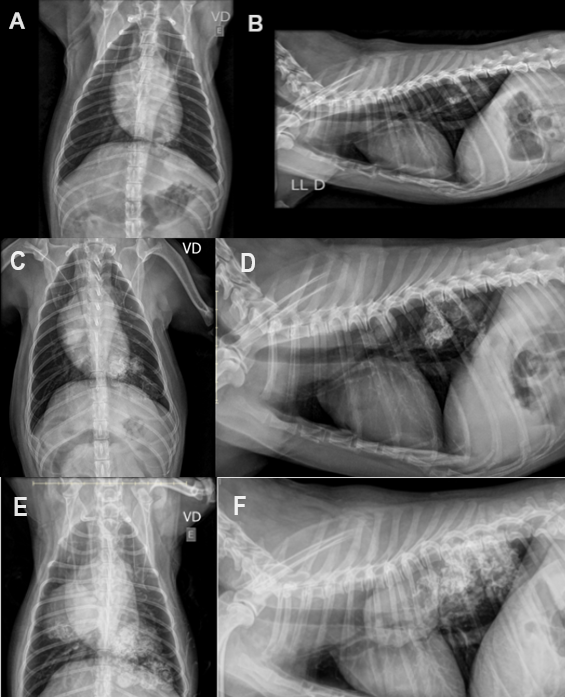
Figure 3: Chest X-ray. A, B. Chest X-ray performed in 2021: Presence of amorphous image with partially defined limits, irregular contours and water radiopacity, with a discrete heterogeneous area of increased radiopacity interspersed, superimposed on the dorsocaudal region of left hemithorax, measuring approximately 3,6cm x 2,5cm. C, D. Chest X-ray performed in 2022: Presence of amorphous image with partially defined limits, irregular contours, water radiopacity, with a heterogeneous area of increased radiopacity interspersed, superimposed on the dorsocaudal region of left hemithorax, measuring 4,47cm x 2,87cm. Another homogeneous radiopacity image measuring approximately 1,87cm x 1,57cm superimposed on the 6th pair of ribs, dorsal to the cardiac silhouette by the laterolateral projection and in the 6th intercostal space on the right by ventrodorsal projection. E, F. Chest X-ray performed in 2023: Presence of nodular image, soft tissue radiopacity with defined limits, overlapping the dorsal region of middle third of right hemithorax, measuring 4.73cm x 4.4cm x 4.2cm. Presence of areas with heterogeneous opacification, high radiopacity, poorly defined limits and irregular contours, overlapping the dorsocaudal region of left hemithorax and dorsal/middle region of the right hemithorax. The image on the left hemithorax measures at least 6,1 cm in the longest axis.
In 2021, after performing a chest x-ray, the presence of amorphous image with partially defined limits, irregular contours and water radiopacity was observed, with a discrete heterogeneous area of increased radiopacity interspersed, superimposed on the dorsocaudal region of left hemithorax. Due to the tumor’s refractoriness to chemotherapy, it was decided by the owner to only monitor the dog. In 2022, this amorphous image with partially defined limits increased in size. In 2023, the image presented a nodular appearance, with soft tissue radiopacity and with defined limits in left hemithorax, being larger in dorsal region of middle third of right hemithorax. Despite the growth of tumor in the lung, at the time of this publication the dog is in good general condition and does not present respiratory symptoms (Figure 3).
Discussion
The multilobular bone tumor is an uncommon bone neoplasm, most frequently described in medium or large breed dogs, with few cases described in small breeds [4]. Clinical manifestations and behavioral changes may arise due to compression of adjacent structures [5], a phenomenon not mentioned by the animal’s owner [4].
An increase in serum alkaline phosphatase levels may occur due to the release of the bone isoenzyme released in cases of reactive lesions or bone neoplasms [7], a finding not verified in the present report, since alkaline phosphatase values were within of the reference limit for the species (44 U/L) [4].
Using imaging tests such as radiography and magnetic resonance imaging, the bone tumor was found to be located in the region of the left zygomatic arch without compromising adjacent structures or the presence of tumor metastases, facts already reported in other investigations [1, 8]. Imaging exams were essential for establishing diagnosis, surgical planning and metastasis research, leading to guidance from the owner on the indication of the surgical procedure with a wide margin of safety [4, 8]. Surgical removal is often difficult due to the location of the neoplasm and local recurrence occurs in approximately 50% of cases [1]. Aggressive surgical excision with wide margins is considered the treatment of choice and can result in long-term remission of the neoplasm [4, 9], once chemotherapy and radiotherapy present a clinical response variable and short-lived [10, 11, 12].
Histologically, a mesenchymal proliferation was observed with sections forming lobular outlines delineated by bundles of spindle cells. Inside the lobules, an atypical cartilaginous component, areas of ossification and foci with immature osteoid matrix were visualized, containing tumor cells with a fusiform or rounded appearance, with rounded to oval nuclei [4, 5, 6].
The lung is a richly vascularized organ and is often the target of metastases [13, 14, 15, 16]. The incidence of primary lung tumors and metastatic is not well established in dogs [17, 18].
The clinical signs presented by dogs vary and are often nonspecific, and exercise intolerance, tachypnea and dyspnea, pleural effusion and hemothorax may be observed. The treatment of choice consists in the surgical excision of tumor, in combination with radiotherapy and chemotherapy [19, 20, 21]. To the multilobular bone tumors, the best therapeutic option is removal of the primary tumor with a wide surgical margin, whereas chemotherapy and radiotherapy for the treatment of lung metastases are not effective [3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22]. Because this discouraging situation, many tutors opt to euthanize the dog due to the dismal prognosis for shortening the suffering [23].
After confirming the diagnosis of a multilobular bone tumor, the owner was advised about the patient’s prognosis and periodic monitoring by the veterinarian in search of local recurrence and the emergence of metastases [1, 4] fact that was verified two years after surgery.
At the time of this publication, the animal was in good general condition and showed no signs of respiratory compromise.
Conclusion
The multinodular bone tumor is an uncommon neoplasm, with a high rate of recurrence and the ability to metastasize. Therefore, it is essential to provide guidance to tutors regarding the need for periodic reevaluation of dogs for the emergence of local recurrence or metastases.
References
-
Cook S, Civello A, Lam R, Fenn J, Neilson D, et al. (2017) Rapid postoperative recurrence of a cranial multilobular tumor of bone in a young dog. Clin Case Rep 5(12): 1995- 1999.
-
Mclain DL, Hill JR, Pulley LT (1983) Multilobular osteoma and chondroma (chondroma rodens) with pulmonary metastasis in a dog. J Am Anim Hosp Assoc 19(3): 359- 362.
-
Losco PE, Diters RW, Walsh KM (1984) Canine multilobular osteosarcoma of the skull with metastasis. J Comp Pathol 94(4): 621-624.
-
Vasconcelos IC, Errante PR (2022) Multilobular bone tumor in Yorkshire terrier breed dog: case report. Rev MV&Z 20(1): e38288.
-
Marangon WF, Mello JB, Rodrigues NS, Merlini NB, Assis MMQ (2020) Multilobular osseum tumor in dog-case report. Braz J Develop 6(10): 83069-83076.
-
Avallone G, Rasotto R, Chambers JK, Miller AD, Behling Kelly E, et al. (2021) Review of histological grading systems in Veterinary Medicine. Vet Pathol 58(5): 809- 828.
-
Berger A, Graca R, Bailey K, Messick J, de Lorimier LP, et al. (2005) Use of alkaline phosphatase staining to differentiate canine osteosarcoma from others vimentin- positive tumors. Vet Pathol 42(2): 161-165.
-
Mcanulty JF, Budgeon C, Waller KR (2019) Catheter occlusion of the dorsal sagittal sinus-confluens sinnum to enable resection of lateral occipital multilobular osteochondrosarcoma in two dogs. J Am Vet Med Assoc 254(7): 843-851.
-
Fontes GS, Cook MR, Johnson LS, Hostnik ET, Lapsley JM, et al. (2023) Multilobular tumor of bone arising from the palatomaxillary suture line in the skull of a dog. Can Vet J 64(6): 545-548.
-
Holmes ME, Keyerleber MA, Faissler D (2019) Prolonged survival after craniectomy with skull reconstruction and adjuvant definitive radiation therapy in three dogs with multilobular osteochondrosarcoma. Vet Radiol Ultrasound 60(4): 447-455.
-
Sweet KA, Nolan MW, Yoshikawa H, Gieger TL (2020) Stereotactic radiation therapy for canine multilobular osteochondrosarcoma. Eight cases. Vet Comp Oncol 18(1): 76-83.
-
Sritrakoon N, Wibulchan W, Karntip W, Sirinarumitr T, Thayananuphat A (2023) Radiotherapy in combination with exenteration and partial orbitectomy for orbital multilobular tumor of bone in a Cocker Spaniel. Open Vet J 13(11): 1485-1490.
-
Rissi DR, Okubo DJA (2020) Metastatic renal interstitial cell tumor in a dog. J Vet Diag Invest 32(6): 957-960.
-
Nemoto Y, Nakaichi M, Sakurai M, Itamoto K, Morimoto M, et al. (2023) Histiocytic sarcoma with spinal necrosis in a dog with progressing non-ambulatory tetraparesis. Open Vet J 13(3): 394-399.
-
Umeda N, Yamazoe H, Wada A, Nagata K (2023) A dog with extraskeletal osteosarcoma of the salivary glands survived long-term, following surgical resection and adjuvant therapy. J Vet Med Sci 85(3): 358-362.
-
Renzi A, Sabatinni S, Annunzio DG, Zaccone R, Perfetti S, et al. (2023) Multiorgan metastases with massive bone involvement of a medullary thyroid carcinoma in a dog. Vet Clin Pathol 52(2): 341-345.
-
McPhetridge JB, Scharf VF, Regier PJ, Toth D, Lorange M, et al. (2021) Distribution of histopathologic types of primary pulmonary neoplasia in dogs and outcome of affected dogs: 340 cases (2010-2019). J Am Vet Med Assoc 260(2): 234-243.
-
Chalfon C, Finotello R, Sabatinni S, Gramer I, Morris JS, et al. (2023) Patters of nodal metastases, biological behaviour, and prognosis of canine mast cell tumors of the pinna: A multi-institutional retrospective study. Vet Comp Oncol 21(2): 332-338.
-
Lee BI, LaRue SM, Seguin B, Griffin L, Prebble A, et al. (2020) Safety and efficacy of stereotactic body radiation therapy (SBRT) for the treatment of canine thyroid carcinoma. Vet Comp Oncol 18(4): 843-853.
-
Rose RJ, Worley DR (2020) A contemporary retrospective study of survival in dogs with primary lung tumors: 40 cases (2005-2017). Front Vet Sci 7: 519703.
-
Ichimata M, Kagawa Y, Namiki K, Toshima A, Nakano Y, et al. (2023) Prognosis of primary pulmonary adenocarcinoma after surgical resection in small-breed dogs: 52 cases (2005-2021). J Vet Intern Med 37(4): 1466-1474.
-
Dernell WS, Straw RC, Cooper MF, Powers BE, LaRue SM, et al. (1988) Multilobular osteochondrosarcoma in 39 dogs: 1979-1993. J Am Anim Hosp Assoc 34(1): 11-18.
-
Stoll MR, Roussh JK, Moisan PG (2001) Multilobular tumor of bone with no abnormalities on plain radiography in a dog. J Small Anim Pract 42(9): 453-455.
- California Red-Legged Frog and Non-Listed Amphibians Response to Non-Native Fish Removal
- Industrial Standardization of the Bio-OS: Algorithmic Codification of Resilience Engineering Guidelines and Version V8 Architecture
- Climate Variability and the Sustainability of Snail Farming in Nigeria: Past Trends, Present Challenges and Potential Outlook
- The Evaluation of the Surveillance System of Anthrax in Gilgit-Baltistan, Pakistan, 2018
- Natural Decline to Extinction of A New Zealand Rabbit Population
- Mitochondrial Bio-Logistics: Steering Co-Enzyme Q10 and Lycopene Synergies within the Science 4.0 Bio-OS Framework