Systematic Review and Meta-Analysis of Sciatic Nerve Injury in Acetabular Fractures
Background: Acetabular fracture is a challenging orthopaedic injury, usually associated with post-traumatic arthritis, deep vein thrombosis, and sciatic nerve injury (SNI). Therefore, we assess the incidence and outcome of SNI associated with acetabular fractures in this study. Methodology: We applied search keywords across PubMed, clinicaltrail.gov, Scopus, and Cochrane library database from 2002 to March 2022 with the studies reporting SNI associated with acetabular fracture. Patient's demographic details, acetabular fracture type, recoveries rate and time, number of patients with acetabular fracture reporting SNI, and follow-up. Methodological Index for Observational Non-Randomized Studies (MINORS) criteria assessed the quality appraisal of each identified study. Results: This study includes twenty-one studies with a total of 682 patients, 19 iatrogenic SNI, and 44 post-traumatic injuries. Overall incidence of post-traumatic and iatrogenic SNI associated with acetabular fractures was 9% [95% CI: 6%-11%] and 5% [95% CI: 3%-7%] respectively. The overall recoveries rate from iatrogenic SNI and post-traumatic SNI associated with acetabular fracture were 55% (95% CI: 22%-83%) and 68% (95% CI: 53% -81%), respectively. The overall quality score of all included studies was 64.28± 7.43% (R: 56.25 % -81.25%), with seven studies below 60%. In most cases, Recoveries of sciatic nerve injury occur within 2-24 months after any open reduction and internal fixation (ORIF). Conclusion: This review estimates SNI incidence with acetabular fracture and recoveries rates. However, this study fails to report the association of SNI with specific acetabular fracture types due to insufficient reported data across eligible studies.
Introduction
Acetabular fracture is a complex orthopedic injury managed using different surgical approaches such as ilioinguinal, Kocher-langenbeck, anterior intrapelvic, or combined surgical approach [1]. Acetabular fractures usually occur among young and elderly populations that result from trauma with significantly high kinetic energy, as in motor vehicle accidents, falls from heights, and extreme sporting events [2]. Most displaced acetabular fractures require open reduction and internal fixation (ORIF) surgery to restore the normal hip anatomy [3]. ORIF approaches for displaced acetabular fracture are intrapelvic approaches (i.e., Stoppa approach) and extra-pelvic approaches (i.e., ilioinguinal approach). In 1961, Letournel described the ilioinguinal approach, which usually manages columns and anterior fractures [4]. Stoppa approach treats intra- abdominal surgical diseases such as incisional hernia and complicated groin. But in 1989, Cole, et al. described the Stoppa approach in the management of displaced fracture related to the pelvic medial wall, quadrilateral surface and sacroiliac joint [5]. The complications of surgical approach intervention in managing acetabular fractures are chondrolysis, post-traumatic arthritis (PTA), femoral head osteonecrosis, and sciatic nerve injury [6]. Acetabular fractures damage articular cartilages, leading to post- traumatic arthritis [7]. A Finland national-wide study reported an increased incidence of acetabular fractures from 6.4/1000 to 8.1/1000 [8].
Potential causes of sciatic nerve palsy related to acetabular fracture include iatrogenic injury occurring during reconstructive surgery, direct trauma damage, late complication of surgery, improper traction, excessive leg stretching, and damage caused by suture and trochanteric wire [9, 10]. However, the potential cause of Iatrogenic SNI includes placements of implants, instruments, and retractors. Causes of post-traumatic SNI include dislocation or fracture of the hip joint. Post-surgical complications might cause SNI by implant migration, hematoma, heterotopic ossification, and muscle scarring. Additionally, SNI depends on the patient’s age and comorbidities, anatomical location of the injury, chronicity, and injury severity [10].
The prevalence of sciatic nerve palsy associated with acetabulum fracture ranges from 10% to 30% [10, 11]. However, the iatrogenic sciatic nerve palsy rate related to acetabulum fracture occurred between 5% to 15% [10]. This injury significantly affects the outcome of the acetabular fracture fixation [12].
A detailed history should be assessed to determine the temporal relationship between clinical presentation and reconstructive surgery of acetabular fracture or any pre- existing lumbosacral degenerative disease. Patients may present with several motor and sensory symptoms. Thus, specific imaging studies such as magnetic resonance imaging (MRI), computed tomography (CT), electromyographic studies, and plain radiographs helps in detecting the nerve injury and its grade [10, 13].
The surgeon intraoperatively confirmed most post- traumatic SNI occurred due to blunt contusion of nerves [10]. However, it is challenging to determine the severity of the nerve injury intraoperatively and predict the outcome [14]. Understanding the root cause of SNI can help the surgeon choose an appropriate therapeutic approach. Thus, we aim to determine iatrogenic and post-traumatic nerve injury incidence and outcome in an acetabular fracture setting.
Methodology
This study focuses on assessing the incidence and outcome of SNI associated with acetabular fracture following “Preferred Reporting Items for Systematic Review and Meta- analysis (PRISMA)” guidelines [15].
Literature Search and Selection Criteria
We performed an electronic search of Scopus, PubMed, cliniicaltrail.gov, and Cochrane Library database from 2002 to March 2022. We discovered the potential articles using keywords and MESH terms: sciatic nerve palsy, sciatic nerve injury, “Sciatic Neuropathy”[Mesh], acetabular, pelvic, and fractures. We use Boolean operators and relevant keywords to find their intersection. Also, search keywords were matched based on a different database. Manually, we checked the reference of eligible studies and relevant abstract and narrative reviews. Also, a literature search was restricted to the English language only.
We included only those articles that meet the following study criteria 1) longitudinal observation study 2) sciatic nerve palsy 3) recoveries of SNI 4) All gender 5) studies published in a peer-review journal 6) publicly full-text available studies. The following criteria are used to exclude if 1) review articles 2) no full text available 3) editorial letter/ commentaries 4) non-research letter 5) animal studies 6) case reports or case series 7) conference abstracts
Study Selection, Data Extraction and Quality Assessment
We create an endnote library for all literature searches. Three authors “(N.H.), (S.A.) and (F.A.) ” evaluated each identified article individually to screen records that did not meet the study criteria. An independent third-party reviewer “J.A.” resolved any discrepancies. We conducted a full-text review if the abstract of relevant articles could not demonstrate specific results. We performed data extraction after full-text analysis into data collection form using Microsoft word. Three authors “(N.H.), (S.A.) and (F.A.)” independently extracted article details like study design, age of the population, study period, country, the total number of participants, acetabular fracture type, fracture fixation approach, number of patients with SNI, SNI recoveries and time until recoveries.
We only included the case of complete SNI recovery. Also, we considered patients with partial or no recovery as one group since partial recovery did not provide any clinical meaning. Three authors “(N.H.), (S.A.) and (F.A.)” independently assessed the methodological quality of each identified study using a methodological index for observational non-randomized studies (MINORS) [16].
Statistical Methods
A fixed and random effect model evaluated sciatic nerve injury’s overall effect associated with acetabular fracture incidence and recoveries. The outcomes were assessed using dichotomous variables, i.e., event and total sample size. Higgins I2 statistic quantifies heterogeneity level, interpreted as minimal (1%-40%), moderate (30%-60%), substantial (50%-90%), and considerable (90%-100%). Fixed effects model was used in estimating overall effects for minimal heterogeneity while random effects for moderate and substantial heterogeneity. We performed subgroup analysis based on data collection method, Publication year, and quality appraisal. We used Comprehensive Meta-analysis (CMA) software version 3 to estimate the overall effect of primary outcomes and create a forest plot to present the outcomes. The pooled effect was considered statically significant at P-value< 0.05.
Results
This review includes 21 studies, including 682 patients at follow-up with an average of 38.6 years. Most studies were retrospective (N=17) and prospective cohort (N=4) studies. Patients usually underwent open reduction and internal fixation (ORIF) for acetabular fracture within 4 days to 21 days. An eligible study reported 44 post-traumatic SNI and 19 iatrogenic SNI in 682 patients.
The characteristics of each eligible study are summarised in Table 1. The MINORS tool summarizes the quality appraisal of each eligible study as in Table 2. The overall quality score of all included studies was 64.28± 7.43% (R: 56.25 % -81.25%), with seven studies below 60%. In most cases, Recoveries of sciatic nerve injury occur within 2-24 months after any ORIF.
| Reference study | Study design | Age (years) | Study period | Country | Total patients at follow up | Fracture type | No. of patients with | Fracture fixation approach | No. of recoveries from | Recovery time (months) | Time until ORIF | Final follow up (months) |
| :--- | :--- | :--- | :--- | :--- | :--- | :--- | :--- | :--- | :--- | :--- | :--- | :--- |
| Al Adawy, 2020 [17] | RC | 41.8 ± 8.42 | 2015-2019 | Egypt | 38 | AC fracture: 15; ACPHT (both columns): 5; T type:10 | 0 | 3 | MS/I | 3 | 0 | 06-Dec | <4 weeks | 18 |
| Almeida AGI, 2011 [18] | PC | NR | 1999-2009 | Brazil | 76 | All types of fracture | 7 | 3 | KL, KL+I, I | 3 | 5 | NR | NR | 58.8 (48-72) |
| Anizar-Faizi A, 2014 [19] | RC | 39.9 (R: 14-81) | 2008-2011 | Malaysia | 30 | All types of fracture | 0 | 3 | KL, I, KL+I | 1 | | 10 | 16.1 (1-68) days | 12 |
| Ebraheim NA, 2007 [20] | RC | 41 (R:14-80) | July 1998 - Feb 2004 | USA | 32 | post wall fractures | 2 | 0 | KL | 0 | 2 | 24 | 4 (1-26) days | 43 (24-70) |
| Giordano V, 2009 [21] | PC | 39.9 (23.3-66.7) | NR | Brazil | 35 | post wall fractures | 3 | 0 | KL | 0 | 3 | NR | 7-21 days | 12 |
| Gultac E, 2019 [22] | RC | 34.9 (R: 19-67). | 2009-2013 | Turkey | 21 | Post wall fractures | 1 | 0 | KL | NA | 1 | 8 | NR | 24 (12-60) |
| Gupta RK, 2015 [23] | RC | 43.77 | Dec 2001-Jan 2013 | India | 64 | All types of fracture | 5 | 1 | KL, I | 1 | 2 | NR | < 3 weeks in 35 cases | 60.3 (26-130) |
| Gupta RK, 2009 [24] | RC | 38.4 (19-68) | 1997-2003 | India | 63 | All types of fracture | 0 | 2 | KL, I | 1 | | 3 | 12.33 (4-30) days | 52.94 (37-96) |
| Gupta S, 2017 [25] | RC | 33.28 (R: 17-63) | 2011-2013 | India | 25 | Post wall fractures:15; PC fracture:6; Transverse:4 | 2 | 1 | KL | 1 | 2 | 12 | 4.6 (1-26) days | Jun-15 |
| Gupta S, 2018 [26] | RC | 30.5 (R:18-49) | 2011-2013 | India | 6 | Post wall fractures | 1 | 0 | KL | NA | 1 | 24 | NR | 47.7 (43-57) |
| Harnroongroj T, 2013 [27] | RC | 38.14 | 2001-2011 | Thailand | 21 | post wall fracture | 0 | 3 | KL | 0 | | NR | NR | 36 |
| Iqbal F, 2016 [28] | PC | 44.20±11.65 | 2012- 2014 | Pakistan | 50 | Simple fracture:48, associated fracture pattern :8 | 6 | 0 | KL, I | 0 | 4 | 12 | 5 ± 3.59 days | 24 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Kim HT, 2011 [29] | RC | 47.9 | 2004- 2009 | Korea | 33 | post wall fractures | 4 | 0 | KL | 0 | 2 | NR | NR | 24 |
| Kim HY, 2015 [30] | RC | 45 (R:20- 70) | 2007- 2010 | Korea | 22 | Anterior column:6; | 3 | 0 | MS; MS+ KL | 0 | 2 | 7 | NR | 30 (24-36) |
| transverse and posterior wall:6 | ||||||||||||||
| T-shape:1; | ||||||||||||||
| AC +ACPHT:8 | ||||||||||||||
| Both column:1 | ||||||||||||||
| Liu X, 2010 [31] | RC | 44.05 | 1999- 2009 | China | 19 | All types of fracture | 2 | 0 | KL, I | 0 | 2 | 2 | 1-12 weeks | 58.5 |
| Magu NK, 2014 [32] | RC | 41.28 ± 7.16 | 1990- 2007 | India | 25 | Post wall fractures | 0 | 1 | KL | 1 | 15 | 4.2±1.7 days | 60 | |
| Malhotra R, 2019 [33] | PC | 46.4 (R: 21- 57) | 2012- 2015 | India | 18 | Acetabular fracture | 1 | 1 | KL | 1 | 1 | 4 | <3 weeks | 57.6 (48- 70) |
| Masse A,2013 [34] | RC | 35.25 | 2005- 2011 | Italy | 31 | T-fracture, transverse, post wall fractures | 2 | 0 | KL | 0 | 0 | NR | NR | 43 (24-87) |
| Paksoy AE, 2019 [14] | RC | 38.3 (R: 17- 71) | 2011- 2014 | Turkey | 35 | AC: 9; ACPHT (both columns):16 | 2 | 0 | MS/I/KL / combined (MS+I+KL) | 1 full recoveries & 1 partial recoveries | NR | 6.3 (2- 17) days | 21.3 (12- 47) | |
| ; T type:5; AC +ACPHT: 2; ACPHT+ PC:5 | ||||||||||||||
| Wang SX, 2019 [35] | RC | 41.1 (R:21- 64) | Feb 2010- Sep 2014 | China | 21 | Post wall fractures | 3 | 0 | KL | NA | 3 | NA | NR | 49 (36-79) |
| Yang Y, 2022 [36] | RC | 47 | 2009- 2018 | China | 17 | Transverse and post wall fracture | 0 | 1 | KL | 1 | 0 | 5 | 7.1 days | 29.5 (12- 96) |
Table 1: Characteristics of each eligible study. I: Ilioinguinal; KL: Kocher-Langenbeck; AIF: Anterior Iliofemoral; MS: Modified
| Clearly stated aim | Inclusion of consecutive patients | prospective data collection | Appropriate endpoints to study aim | Unbiased assessment of study endpoint | Follow-up period relevant to study aim | <5% lost to follow-up | Prospective calculation of the study size | Overall score | Overall score % | |
|---|---|---|---|---|---|---|---|---|---|---|
| Al Adawy, 2020 [17] | 2 | 2 | 1 | 2 | 0 | 2 | 2 | 0 | 11 | 68.75 |
| Almeida AGI, 2011 [18] | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 0 | 12 | 75 |
| Anizar-Faizi A, 2014 [19] | 2 | 2 | 1 | 2 | 0 | 2 | 2 | 0 | 11 | 68.75 |
| Ebraheim NA, 2007 [20] | 2 | 2 | 1 | 2 | 1 | 2 | 2 | 0 | 12 | 75 |
| Giordano V, 2009 [21] | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 0 | 13 | 81.25 |
| Gultac E, 2019 [22] | 2 | 2 | 1 | 1 | 0 | 2 | 2 | 0 | 10 | 62.5 |
| Gupta RK, 2015 [23] | 2 | 2 | 1 | 1 | 0 | 2 | 1 | 0 | 9 | 56.25 |
| Gupta RK, 2009 [26] | 2 | 2 | 1 | 1 | 0 | 2 | 1 | 0 | 9 | 56.25 |
| Gupta S, 2017 [25] | 2 | 2 | 1 | 1 | 0 | 1 | 2 | 0 | 9 | 56.25 |
| Gupta S, 2018 [26] | 1 | 2 | 1 | 1 | 0 | 2 | 2 | 0 | 9 | 56.25 |
| Harnroongroj T, 2013 [27] | 2 | 2 | 1 | 2 | 0 | 2 | 2 | 0 | 11 | 65 |
| Iqbal F, 2016 [28] | 2 | 1 | 2 | 2 | 0 | 2 | 1 | 0 | 10 | 62.5 |
| Kim HT, 2011 [29] | 1 | 2 | 2 | 1 | 0 | 2 | 1 | 0 | 9 | 56.25 |
| Kim HY, 2015 [30] | 2 | 1 | 1 | 2 | 0 | 2 | 1 | 0 | 9 | 56.25 |
| Liu X, 2010 [31] | 2 | 2 | 1 | 1 | 0 | 2 | 2 | 0 | 10 | 62.5 |
| Magu NK, 2014 [32] | 2 | 2 | 1 | 2 | 0 | 2 | 2 | 0 | 11 | 68.75 |
| Malhotra R, 2019 [33] | 2 | 2 | 2 | 1 | 0 | 2 | 2 | 0 | 11 | 68.75 |
| Masse A, 2013 [34] | 2 | 2 | 1 | 1 | 0 | 2 | 2 | 0 | 10 | 62.5 |
| Paksoy AE, 2019 [14] | 2 | 2 | 1 | 1 | 0 | 2 | 1 | 0 | 9 | 56.25 |
| Wang SX, 2019 [35] | 2 | 2 | 1 | 2 | 0 | 2 | 2 | 0 | 11 | 68.75 |
| Yang Y, 2022 [36] | 1 | 2 | 2 | 2 | 0 | 2 | 1 | 0 | 10 | 62.5 |
Table 2: MINORS criteria assessing quality appraisal of each eligible study. Each item scored 2 points. The maximum overall score
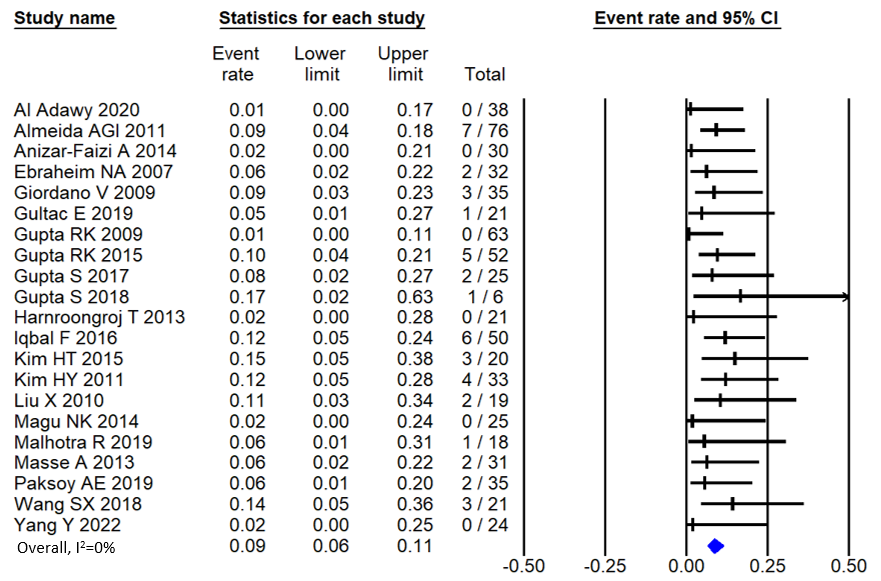
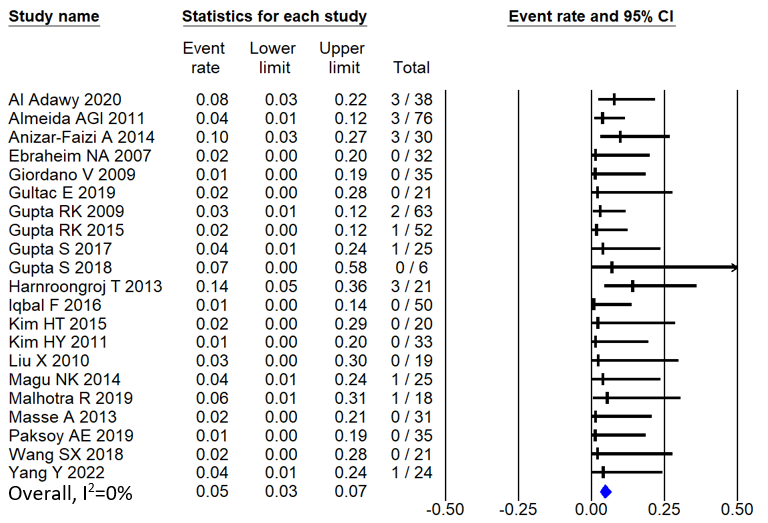
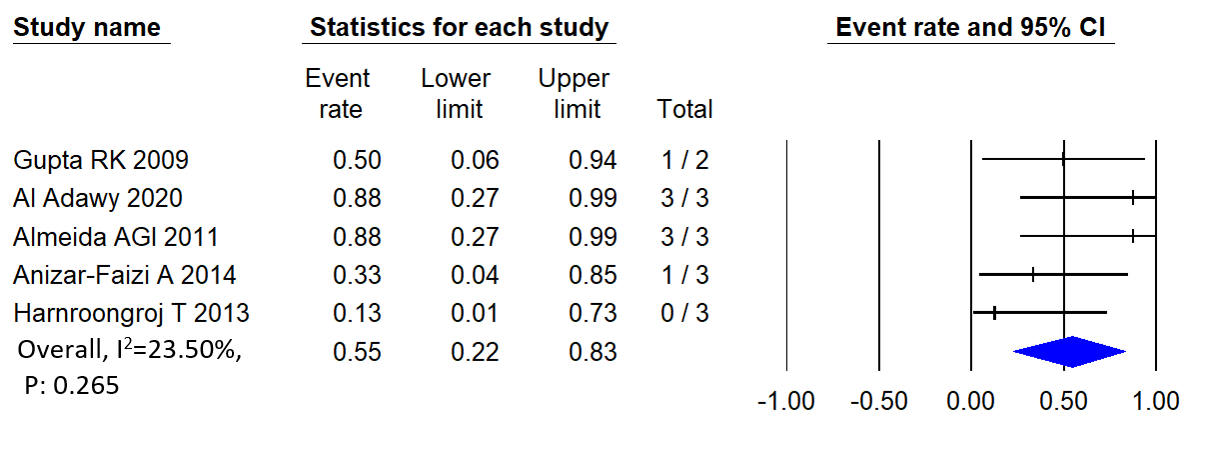
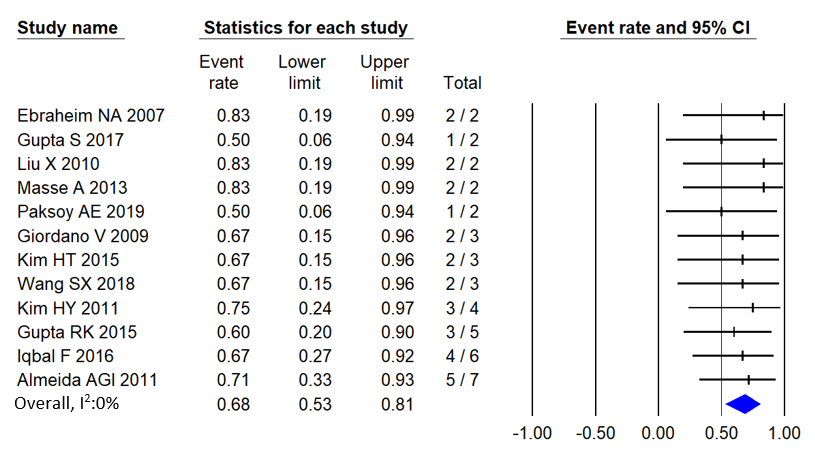
The overall incidence of post-traumatic SNI associated with acetabular fracture was 9% [95% CI: 6%-11%], as in Figure 1. Similarly, the overall incidence of Iatrogenic SNI associated with acetabular fracture was 5% [95% CI: 3%- 7%], as presented in Figure 2. The heterogeneity between the studies was minimal for post-traumatic SNI and Iatrogenic SNI. Figures 3 and 4 demonstrated the recoveries from iatrogenic SNI and Post-traumatic SNI. The overall recoveries rate from iatrogenic SNI and post-traumatic SNI associated with acetabular fracture were 55% (95% CI: 22%-83%) and 68% (95% CI: 53% -81%), respectively. Since meta-analysis could not be performed for 1 sample, we rejected the studies reporting SCI for only one patient for recoveries outcome [23, 25, 32, 33, 36].
| Number of studies | Overall effect, % | L CI, % | U CI, % | I² | P value | References | |
|---|---|---|---|---|---|---|---|
| 1 | 7 | 30.5 | 22 | 40.6 | 70.29 | 0.003 | [14,19-19,23,24,28] |
| KL | 18 | 88 | 78.3 | 93.7 | 81.33 | <0.001 | [18-32,34,35] |
| AIF | 1 | 2.6 | 0.7 | 9.9 | 0 | <0.005 | [18] |
| MS | 2 | 39 | 17 | 66 | 81.24 | 0.021 | [14,17] |
| I + MS | 1 | 31 | 18 | 48 | 0 | 1 | [14] |
| I + KL | 4 | 39.3 | 16.3 | 68.3 | 83.45 | <0.005 | [14,23,30,33] |
Table 3: Meta-analysis of different surgical approach. I: Ilioinguinal; KL: Kocher-Lange beck; AIF: Anterior Iliofemoral; MS: Mod
Table 3: Meta-analysis of different surgical approach. I: Ilioinguinal; KL: Kocher-Lange beck; AIF: Anterior Iliofemoral; MS: Modified Stopp Table 3 demonstrates the overall rate of various surgical approaches to fixing the acetabular fracture. The various surgical processes were ilioinguinal, Kocher langebeck, modified Stoppa, and anterior iliofemoral. The most frequently used surgical approach was Kocher-Langenbeck, while the least was an anterior iliofemoral approach. The overall rate of Kocher langerbeck and anterior iliofemoral surgical methods was 88% [95% CI: 78.3%-93.7] and 2.6% [95 CI: 0.7%-9.9%], respectively.
| Post-traumatic SNI incidence (%) | Iatrogenic SNI incidence (%) | Post-traumatic SNI recovery (%) | Iatrogenic SNI recovery (%) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Subgroup analysis | N | overall effects | 95% L CI | 95 % UCI | N | overall effects | 95% L CI | 95 % UCI | N | overall effects | 95% L CI | 95 % UCI | N | overall effects | 95% L CI | 95 % UCI | I2 |
| All studies | 21 | 8.6 | 6.5 | 11.3 | 21 | 4.6 | 3.1 | 6.7 | 1.2 | 68.5 | 53 | 80.7 | 5 | 53.9 | 22.3 | 80.2 | 23.05 |
| MINORS rating | |||||||||||||||||
| <10 | 12 | 9.93 | 6.6 | 13.1 | 12 | 2.6 | 1.4 | 4.9 | 1 | 50 | 6 | 94 | 1 | 50 | 6 | 94 | 0 |
| >10 | 9 | 7.5 | 4.8 | 11.6 | 9 | 6.4 | 3.9 | 10.4 | 4 | 56.3 | 16.8 | 89.1 | 4 | 56.3 | 16.8 | 89.1 | 42.58 |
| Data collection | |||||||||||||||||
| prospective | 4 | 9.7 | 6.1 | 15 | 4 | 3.3 | 1.4 | 7.7 | 3 | 68.7 | 43.2 | 86.3 | 1 | 87.5 | 26.6 | 99.3 | 0 |
| retrospective | 17 | 8 | 5.6 | 11.3 | 17 | 5 | 3.2 | 7.7 | 9 | 68.3 | 48.4 | 83.2 | 4 | 44.4 | 15.3 | 75.9 | 15 |
| Years of Publication | |||||||||||||||||
| 2002-2012 | 6 | 8.8 | 5.6 | 13.4 | 6 | 2.9 | 1.4 | 6 | 5 | 74.5 | 51.2 | 89 | 2 | 71.3 | 24.7 | 94.9 | |
| 2013-2022 | 15 | 8.5 | 5.9 | 12 | 15 | 5.5 | 3.5 | 8.7 | 7 | 63.9 | 43 | 80.6 | 3 | 43.3 | 8.5 | 86.5 | 42.78 |
Table 4: Outcome of sub-group analysis determining the variation of reported incidence based on quality appraisal, data collectio
Similarly, Table 4 represents the subgroup analysis of potential incidence variation of Sciatic nerve injury in association with MINORS quality appraisal, publication years, and data collection method. The sub-group analysis represents the reduced incidence of post-traumatic sciatic nerve injury (SNI) associated with an acetabular fracture in recent ten years. Also, a higher incidence rate of post- traumatic SNI was observed in retrospective or low-quality studies (MINORS rating <10). However, the incidence of iatrogenic SNI increased in recent years, with high-quality studies and retrospective studies.
Interestingly, we observed a higher incidence of post- traumatic SNI than in Iatrogenic SNI concerning quality of studies, methodological data collection process, and years of articles published.
Discussion
Sciatic nerve injury associated with acetabular fracture occurs due to a direct traumatic injury, intra-operative caused by retractor placement, implant position, and traction or post-operative by hematoma or heterotopic ossification [10]. The tibial division of the sciatic nerve is less susceptible to injury and more likely to recover faster than the peroneal division. The susceptibility of the peroneal division occurs due to nerve tethering with a lower excursion at the greater sciatic notch and fibula neck, and a thinner nerve bundle with a smaller diameter of the peroneal branch than the tibial branch of the sciatic nerve [10, 37, 38]. This review has considerable heterogeneity about the incidence of iatrogenic and post-traumatic sciatic nerve injury. The incidence of post-traumatic sciatic nerve injury associated with posterior acetabular wall fracture can be as high as 30%. In addition, the incidence of iatrogenic sciatic nerve injury during the management of acetabular fracture with posterior surgical approach is 15% [39]. However, an inadvertently long screw used for osteosynthesis or an anterior surgical approach for acetabular fracture may cause SNI [40]. Our analysis demonstrates a higher incidence of post- traumatic SNI and lower iatrogenic SNI associated with acetabular fracture of 8.6% and 4.6%, irrespective of fracture type than the outcome of recent literatures [10, 41, 42]. This might be due to pooled consideration of different surgical approach in a single study.
None of studies described the occurrence of SNI based on used surgical approach.
Several precautions are proposed to avoid iatrogenic SNI during the surgical fixation of acetabular fracture. Knee flexion and hip extension maintained during surgical fixation of acetabular fracture reduces sciatic nerve tension and prevents iatrogenic SNI [40, 42]. Special Hohman retractors protect the sciatic nerve at sciatic notch region during operative fixation of acetabular fracture. These retractors are positioned between bone and hip external rotator muscles to avoid nerve injury during posterior surgical management of acetabular fracture [10].
The role of intraoperative somatosensory evoked potentials (SSEP) remains controversial. Helfet, et al. reported only a 2% incidence of Iatrogenic SNI using SSEP during the fixation of acute acetabular fractures [43]. The coupling of electromyography (EMG) and SSEP provides more rapid response for any irritation of sciatic nerve than SSEP alone. SSEP are significantly affected by epidural anaesthesia and anaesthetics [44]. Interestingly, in accordance with finding of previous literature, our analysis observed 70% spontaneous recovery of SNI [45]. Fassler, et al. reported that severe damage to the peroneal branch of the sciatic nerve cause worsened outcomes. Electromyography analysis demonstrated that iatrogenic or traumatic sciatic nerve injuries resulted from axonotmesis rather than neuropraxia [11]. Thirteen studies in this review reported the approximate time required for SNI spontaneous recovery. The recovery period of sciatic nerve injury varies from 2 months to 2 years [17, 19, 20, 24, 25, 26, 28, 30, 33, 36]. Thus, it becomes real challenge to decide the exact recovery time of intervention. Thus, a surgical approach in the form of tendon transplant can be considered if SNI spontaneous recovery fails after two years of post-injury. The surgeon’s ability to predict the outcome of SNI from an intraoperative macroscopic observation of an injured nerve rather than anatomically continuous sciatic nerve during the fixation of acetabular fracture would be beneficial. Unfortunately, this question remains yet to answer. However, intraoperative ultrasound can aid in viewing avulsed nerve directly and detect the proportion of intact fascicles [46].
Intraoperative ultrasounds scan the avulsed nerve directly and assess the fraction of intact fascicles, are one example of an effort in this direction [47, 48]. The outcome of ultrasound is significantly beneficial. However, safe use in clinical practices requires robust research. The nerve regeneration velocity of the axon is 1-2mm/ day. Regeneration of the sciatic nerve starts at the acetabulum level and requires reaching the whole leg length. Therefore, any surgical approach for nerve reformation should begin within 90-120 days post-injury. The nerve reform is doubtful to occur after 120 days [49, 50].
Limitation
This systematic review has several limitations 1) most of the studies were retrospective which might cause reporting bias 2) insufficient information on the severity of SNI 3) insufficient information on damage branching of sciatic nerve 4) only a few studies reported exact recovery time of SNI 5)
It remain unclear whether partial recovery was significant or not 6) insufficient data could not assess the association of acetabular fracture type and surgical approach 7)
Conclusion
Our meta-analysis reports approximately 5% and 9% incidence of iatrogenic and post-traumatic SNI. However, this study could not assess the association between acetabular fracture type and various surgical methods. Recoveries of SNI usually occur within two months to 2 years. If SNI spontaneous recovery fails after two years, a surgical option, i.e., tendon transplant, may be considered.
References
-
Kilinc CY, Acan AE, Gultac E, Kilinc RM, Hapa O, et al. (2019) Treatment results for acetabulum fractures using the modified Stoppa approach. Acta Orthopaedica et Traumatologica Turcica 53(1): 6-14.
-
Matta JM, Mehne DK, Roffi R (1986) Fractures of the acetabulum. Early results of a prospective study. Clin Orthop Relat Res (205): 241-250.
-
Altun G, Saka G, Demir T, Elibol FKE, Polat MO (2019) Precontoured buttress plate vs reconstruction plate for acetabulum posterior wall fractures: A biomechanical study. World Journal of Orthopedics 10(5): 219.
-
Letournel E (1993) The treatment of acetabular fractures through the ilioinguinal approach. Clinical orthopaedics and related research 292: 62-76.
-
Cole JD, Bolhofner BR (1994) Acetabular fracture fixation via a modified Stoppa limited intrapelvic approach. Description of operative technique and preliminary treatment results. Clinical orthopaedics and related research 305: 112-123.
-
Stibolt RD, Patel HA, Huntley SR, Lehtonen EJ, Shah AB, et al. (2018) Total hip arthroplasty for posttraumatic osteoarthritis following acetabular fracture: A systematic review of characteristics, outcomes, and complications. Chinese journal of traumatology 21(3): 176-181.
-
Bueno TSP, Godoy GPDE, Furukava RB, Gaggioli NT, Tamaoki MJS, et al. (2021) Heterotopic ossification in acetabular fractures: systematic review and meta- analysis of prophylaxis. Acta Ortop Bras 29(6): 331-340.
-
Rinne PP, Laitinen MK, Huttunen T, Kannus P, Mattila VM (2017) The incidence and trauma mechanisms of acetabular fractures: A nationwide study in Finland between 1997 and 2014. Injury 48(10): 2157-2161.
-
Park JS, Kim WJ, Hong CH, Soh JW, Nho JH, et al. (2015) Sciatic Nerve Palsy Caused by Ruptured and Contracted Short External Rotator Muscles after Primary Total Hip Arthroplasty. Hip & pelvis 27(2): 120-124.
-
Issack PS, Helfet DL (2009) Sciatic nerve injury associated with acetabular fractures. HSS J 5(1): 12-18.
-
Fassler PR, Swiontkowski MF, Kilroy AW, Routt MLJ (1993) Injury of the sciatic nerve associated with acetabular fracture. JBJS 75(8): 1157-1166.
-
Lefaivre KA, Slobogean GP, Ngai JT, Broekhuyse HM, O’Brien PJ (2014) What outcomes are important for patients after pelvic trauma? Subjective responses and psychometric analysis of three published pelvic-specific outcome instruments. J Orthop Trauma 28(1): 23-27.
-
Zaidman CM, Seelig MJ, Baker JC, Mackinnon SE, Pestronk A (2013) Detection of peripheral nerve pathology: comparison of ultrasound and MRI. Neurology 80(18): 1634-1640.
-
Paksoy AE, Topal M, Aydin A, Zencirli K, Kose A, et al. (2019) Outcomes of surgical management of acetabular fractures treated with anterior approaches. The Eurasian Journal of Medicine 51(3): 257.
-
Moher D, Liberati A, Tetzlaff J, Altman DG, The PG (2009) Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLOS Medicine 6(7): e1000097.
-
Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, et al. (2003) Methodological index for non-randomized studies (MINORS): development and validation of a new instrument. ANZ Journal of Surgery 73(9): 712-716.
-
Al Adawy AS, Aziz AHA, El Sherief FA, Mahmoud WS, Mabrook M, et al. (2020) Modified Stoppa as an alternative surgical approach for fixation of anterior fracture acetabulum: a randomized control clinical trial. Journal of Orthopaedic Surgery and Research 15(1): 154.
-
de Almeida AGI, Garrido CA, Vaz Amaral LE, Vargas LFL (2011) Prospective study on seventy-six cases of fractured acetabulum with surgical treatment. Rev Bras Ortop 46(5): 520-525.
-
Anizar-Faizi A, Hisam A, Sudhagar KP, Moganadass M, Suresh C (2014) Outcome of Surgical Treatment for Displaced Acetabular Fractures. Malays Orthop J 8(3): 1-6.
-
Ebraheim NA, Patil V, Liu J, Sanford CG, Haman SP (2007) Reconstruction of comminuted posterior wall fractures using the buttress technique: a review of 32 fractures. International Orthopaedics 31(5): 671-675.
-
Giordano V, do Amaral NP, Pallottino A, Albuquerque RPe, Franklin CE, et al. (2009) Operative treatment of transverse acetabular fractures: is it really necessary to fix both columns? International Journal of Medical Sciences 6(4): 192-199.
-
Gultac E, İltar S, Özmeriç A, Koçak A, Aydoğan NH, et al. (2019) Surgical treatment of acetabulum posterior wall fractures: Comparison between under countering and marginal impaction reconstruction method with odd methods. J Clin Orthop Trauma 10(5): 900-903.
-
Gupta RK, Jindal N, Pruthi M (2015) Acetabular fractures labelled poor surgical choices: Analysis of operative outcome. Journal of Clinical Orthopaedics & Trauma 6(2): 94-100.
-
Gupta RK, Singh H, Dev B, Kansay R, Gupta P, et al. (2009) Results of operative treatment of acetabular fractures from the Third World—how local factors affect the outcome. International Orthopaedics 33(2): 347-352.
-
Gupta S, Singh J, Virk JS (2017) The role of trochanteric flip osteotomy in fixation of certain acetabular fractures. Chin J Traumatol 20(3): 161-165.
-
Gupta S, Mittal N, Virk JS (2018) Use of tricortical iliac crest strut autograft in comminuted posterior wall acetabular fractures: A case series. Chin J Traumatol 21(1): 58-62.
-
Harnroongroj T, Riansuwan K, Sudjai N, Harnroongroj T (2013) Posterior acetabular arc angle of unstable posterior hip fracture-dislocation. Int Orthop 37(12): 2443-2449.
-
Iqbal F, Taufiq I, Najjad MK, Khan N, Zia OB (2016) Fucntional and Radiological Outcome of Surgical Management of Acetabular Fractures in Tertiary Care Hospital. Hip Pelvis 28(4): 217-224.
-
Kim HT, Ahn JM, Hur JO, Lee JS, Cheon SJ (2011) Reconstruction of Acetabular Posterior Wall Fractures. Clin Orthop Surg 3(2): 114-120.
-
Kim HY, Yang DS, Park CK, Choy WS (2015) Modified Stoppa Approach for Surgical Treatment of Acetabular Fracture. Clin Orthop Surg. 7(1): 29-38.
-
Liu X, Xu S, Zhang C, Su J, Yu B (2010) Application of a shape-memory alloy internal fixator for treatment of acetabular fractures with a follow-up of two to nine years in China. International Orthopaedics 34(7): 1033-1040.
-
Magu NK, Gogna P, Singh A, Singla R, Rohilla R, et al. (2014) Long term results after surgical management of posterior wall acetabular fractures. Journal of Orthopaedics and Traumatology 15(3): 173-179.
-
Malhotra R, Gautam D (2019) Acute total hip arthroplasty in acetabular fractures using modern porous metal cup. Journal of Orthopaedic Surgery 27(2): 2309499019855438.
-
Masse A, Aprato A, Rollero L, Bersano A, Ganz R (2013) Surgical dislocation technique for the treatment of acetabular fractures. Clin Orthop Relat Res 471(12): 4056-4064.
-
Wang SX, Li BH, Li J, Huang FG, Xiang Z, et al. (2018) Middle-term follow-up results of Pipkin type IV femoral head fracture patients treated by reconstruction plate and bioabsorbable screws. Chin J Traumatol 21(3): 170- 175.
-
Yang Y, Sun J, Xiang Z (2022) The Short- and Mid-term Follow-Up of Single-Column Fixation in Transverse and Posterior Wall Acetabular Fractures. Orthop Surg 14(1): 65-72.
-
John M, Taylor S, Ahmed A, Mir H (2021) Complete Traumatic Laceration of the Sciatic Nerve Secondary to Acetabular Fracture: A Case Report. Journal of Orthopaedic Experience & Innovation 2021: 27442.
-
Giannoudis PV, Da Costa AA, Raman R, Mohamed AK, Smith RM (2005) Double-crush syndrome after acetabular fractures. The Journal of Bone and Joint Surgery British volume 87-B(3): 401-407.
-
Schmeling G (2003) Early complications of acetabular fractures. Fractures of the Pelvis and Acetabulum.
-
Ayık Ö, Kozanoğlu E, Önol Y, Durmaz H (2021) Post- traumatic double crush pudendal nerve entrapment syndrome after fracture of the pelvis: A case report. Acta Orthop Traumatol Turc 55(3): 277-280.
-
Issack PS, Toro JB, Buly RL, Helfet DL (2007) Sciatic Nerve Release Following Fracture or Reconstructive Surgery of the Acetabulum. JBJS 89(7).
-
Pavelka T, Houcek P (2009) Complications associated with the surgical treatment of acetabular fractures. Acta Chir Orthop Traumatol Cech 76(3): 186-193.
-
Helfet DL, Hissa EA, Sergay S, Mast JW (1991) Somatosensory Evoked Potential Monitoring in the Surgical Management of Acute Acetabular Fractures. Journal of Orthopaedic Trauma 5(2): 161-166.
-
Helfet DL, Anand N, Malkani ALL, Heise C, Quinn TJ, et al. (1997) Intraoperative Monitoring of Motor Pathways During Operative Fixation of Acute Acetabular Fractures. Journal of Orthopaedic Trauma 11(1): 2-6.
-
Letournel E, Judet R, Elson RA (1993) Late complications of operative treatment within three weeks of injury. Fractures of the acetabulum: Springer pp: 541-63.
-
Koenig RW, Schmidt TE, Heinen CP, Wirtz CR, Kretschmer T, et al. (2011) Intraoperative high-resolution ultrasound: a new technique in the management of peripheral nerve disorders. Journal of neurosurgery 114(2): 514-521.
-
Agarwal A, Chandra A, Jaipal U, Bagarhatta M, Mendiratta K, et al. (2019) Can imaging be the new yardstick for diagnosing peripheral neuropathy?—a comparison between high resolution ultrasound and MR neurography with an approach to diagnosis. Insights into Imaging 10(1): 104.
-
Hannaford A, Vucic S, Kiernan MC, Simon NG (2021) Review Article “Spotlight on Ultrasonography in the Diagnosis of Peripheral Nerve Disease: The Evidence to Date”. International Journal of General Medicine 14: 4579-4604.
-
Tezcan AH (2017) Peripheral nerve injury and current treatment strategies. Peripheral Nerve Regeneration- From Surgery to New Therapeutic Approaches Including Biomaterials and Cell-Based Therapies Development. 2017: 3-30.
-
Taha A, Taha J (1998) Results of suture of the sciatic nerve after missile injury. Journal of Trauma and Acute Care Surgery 45(2): 340-344.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results