Osteonecrosis of Femoral Head with a Special Note on COVID 19
Background: A prevalent condition in hip joint surgery is osteonecrosis of the femoral head (ONFH). The blood supply to the femoral head is damaged or disrupted for a variety of reasons, which is followed by a succession of pathological alterations and ultimately irreversible destruction of the hip joint. The disease SARS COVID 19 itself and the treatment of the condition with corticosteroids may cause ONFH. Various treatment methods have been described in literature depending on the stage of disease process. Purpose and Methods: The purpose of this review paper is to provide up to date details of the clinical evaluation, current diagnostic tools, and treatment modalities. We shall also mention a special note on the COVID 19. We reviewed several articles in the literature (Pubmed, Scopus, and Google Scholar) on this topic especially the mechanism of injury, diagnosis, and treatment methods to produce a review article. Conclusion: Osteonecrosis of the femoral head is caused by many conditions which ultimately cause the disruption of blood supply to the femoral head. The treatment methods vary with stage of the disease. The early stages can be managed with conservative methods and hip preserving surgeries whereas late stage condition with advanced osteoarthritis requires arthroplasty. The early recognition by clinical and radiological features the progression is reversed or slowed down. The high usage of corticosteroids during COVID 19 and its association with ONFH is a warning sign for the judicious usage of the same in future.
Introduction
Osteonecrosis of femoral head is characterized by bone cell death in a particular segment of the subchondral bone due to disturbance in blood supply to the femoral head. The prominent French anatomist Jean Cruveilhier documented extensive distortion of the femoral head as a consequence of trauma, possibly as a result of vascular injury [1]. On the other hand, Freund is widely regarded as the first author to provide a full description of the avascular necrosis of the both hips [2]. The aetiology of AVN in the hip is unknown, although it is the ultimate common mechanism of traumatic or nontraumatic events that harm the femoral head’s already vulnerable circulation. Gradually, the femoral head collapses and the hip joint is rapidly destroyed which ultimately leads to osteoarthritis.
Epidemiology
A prevalent condition in hip joint surgery is osteonecrosis of the femoral head (ONFH). The blood supply to the femoral head is damaged or disrupted for a variety of reasons, which is followed by a succession of pathological alterations and ultimately irreversible destruction of the hip joint. Statistics show that there are more than 20 million ONFH patients worldwide, with roughly 5-7.5 million instances in China, and that there are between 150 and 200 thousand new cases per year [3, 4]. The United States sees 10,000–20,000 new cases of ONFH each year [5, 6]. Males in their 40s and in females in their 30s are more likely to develop it in Japan [7]. According to reports, Korea’s peak age range is 40-59 years [8]. In the UK, patients’ ages were on average 57.6 years old [9].
Etiology
Among the factors that predispose a subject to ONFH are hip trauma, including femoral neck and acetabular fractures, hip dislocation, sprain or contusion (no fracture but sometimes intra‐articular hematoma) [10] long‐term high‐ dose glucocorticoids [11, 12, 13, 14] long‐term heavy consumption of alcohol [15] thrombophilia and hypofibrinolysis and autoimmune diseases treated with glucocorticoids [16, 17, 18] and a history of having used decompression chambers [19]. It is idiopathic in around 30% of individuals (Table 1) [20]. Males are more often affected than females, and bilateral presentation is usually noted [21]. Within two years, roughly 55% of patients could develop a contralateral hip problem [22]. Ongoing ONFH will be present in about 75% of patients with other sites of involvement [23].
| Deranged lipid metabolism, | Systemic steroid administration, Habitual alcohol use, Hyperlipidemia, Pancreatitis |
| Disturbed arterial supply | Trauma: Fractures and dislocations of the hip |
| Disturbed arterial supply | Iatrogenic: Following surgical intervention around hip |
| Embolic | Gauchers disease, Sickle cell disease Dysbarism (caissons disease) |
| Coagulation disorders (thrombotic) | Thalassemia, Polycythemia, Myeloproliferative disorders, Ionizing radiations |
| Miscellaneous and multifactorial | Slipped capital femoral epiphyses, Legg-Calve-Perthes disease, Congenital hip dislocation, Gout, Systemic lupus erythematosus, Rheumatoid arthritis, Organ transplantation, Pregnancy, Cytotoxic agents, HIV (Human immunodeficiency virus) |
Table 1: Prevalent causes of femoral head avascular necrosis.
Role of Covid-19 as a Disease Process and the Treatment with Steroids
The long-term effects of the COVID-19, which also affect the musculoskeletal system, have been extensively documented in investigations [24]. The physiology of bone and joint tissue in COVID-19 individuals may be influenced by systemic inflammation [25]. CXCL10, IL-17, and TNF- alpha are cytokines that COVID-19 induces [24]. They prevent osteoblasts from proliferating and differentiating as much. Furthermore, several genes encode proinflammatory proteins, such as IL-1b, IL-6, and IL-8, which are associated with hypercoagulability and bone necrosis in COVID-19 patients [26]. Vasculitis and hypercoagulability can interfere with the blood flow in bone vessels and contribute to bone necrosis if they are combined [26]. Viral invasion can cause ACE2 deficiency, which can result in bone matrix degradation [27]. Since Coronaviruses infect the upper respiratory tract by binding to ACE2 receptors in ATII cells, ACE2-dependent effects on bone tissue are also relevant. As a result of Infection with COVID19, ACE2 is a potential factor that regulates bone biology [28, 29].
The majority of COVID-19 hospital patients who get corticosteroids also experience negative effects on their bone tissue [30, 31]. After steroid therapy, there is a 6- to 1-year window during which AVN risk increases [32]. There is disagreement on the dose and length of corticosteroid therapy as a risk factor for developing AVN. According to one prospective study, a dose of more than 20 mg/day considerably increases the incidence of AVN [33].
Clinical Evaluation
A thorough history of the patient is obtained, followed by a physical examination is helpful, In order to suspect that ONFH is present. Symptoms of ONFH may not appear for some time after the onset. Most commonly, groin pain is the main clinical sign. In some cases, pain may occur in the buttocks or knees on the ipsilateral side. Rest cures the symptoms, while weight bearing worsens them. There is a restriction of range of motion, particularly on the inside and outside of the hips, and uncomfortable logrolling (passive rotation of the interior and exterior of the hips) is present [34].
The efficacy of ON treatment is correlated with the stage at which care is began, hence early identification is essential [35].
Over 16 different classifications have been published in the literature for ONFH, based primarily on MRI and radiography. It allows for the determination of prognosis and provides directions for treatment options. The classification systems Ficat and Arlet (63% of studies; Table 2; Figure 1), Steinberg (20%; Table 3), Association Research Circulation Osseous (ARCO) (12%), and the Japanese Orthopedic Association (5%), are the most frequently employed in the literature [36].
| Stage | Findings |
| 1 | Normal radiograph |
| 2 | Normal femoral head sphericity. Some signs of bone remodelling such as cysts or osteosclerotic regions |
| 3 | Subchondral collapse or flattening of the femoral head |
| 4 | Degenerative changes are seen in the acetabulum with narrowing of the joint space |
Table 2: Ficat and Arlet classification.
| Stage | Findings |
| 0 | No symptoms |
| Normal radiograph | |
| MRI non-specific | |
| 1 | Mild pain in the affected hip, or pain with internal rotation |
| Normal radiograph | |
| MRI diagnostic | |
| 2 | Worsening or persistent pain |
| Increased sclerosis or cysts in the femoral head | |
| 3 | Subchondral collapse (crescent sign) |
| 4 | Flattening of the femoral head |
| Normal joint space | |
| 5 | Narrowing of the joint space with/without femoral head involvement |
| 6 | Advanced degenerative changes |
Table 3: Steinberg classification.
Ultimately, all of these classifications are meant to distinguish between pre-collapse lesions, which can be treated conservatively, and post-collapse lesions, which typically require total hip arthroplasty.
Role of Radiology in Treatment and Prevention
Common hip joint disorders like ONFH can be a turning point in the development of a disease. Patients enter the irreversible late stage once it happens [37]. For the purpose of choosing the best course of treatment and enhancing the prognosis, it is essential to be able to estimate the likelihood of femoral head collapse. According to studies, the size and location of the lesion play a significant role in femoral head collapse [38, 39, 40, 41]. The location and extent of the lesion have been depicted using a variety of methods, although they have always relied on MRI or radiography [38, 39, 40, 41, 42, 43].
The following auxiliary investigations are advised in addition to collecting the history and clinical symptoms and signs, which is the first step in making a diagnosis.
Plain Radiography
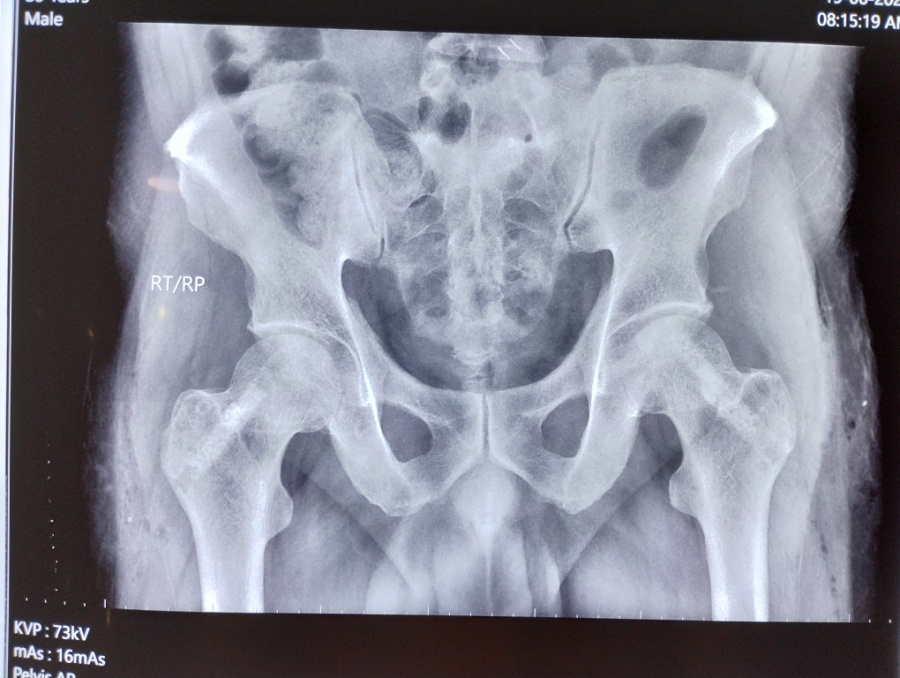
Ankylosing spondylitis, hip dysplasia, osteoarthritis, and rheumatoid arthritis can all be ruled out using X-ray films. ONFH can be diagnosed by identifying the crescent sign, which represents segmental collapse and necrosis surrounded by sclerotic bone. In advanced cases global arthritis of hip joint is seen. (Figure 1).

Stage 1 : X-Ray Pelvis with both hips showing no radiological changes Stage 2: The femoral head contour is still normal with early signs of reactive change in the subchondral area.
Stage 3: Signs of osteonecrosis with evidence of structural damage and distortion of the bone outline. Collapse of the necrotic segment Figure 1: Various stages of osteonecrosis of femoral head.
Magnetic Resonance Imaging
MRI is the standard method for ONFH diagnosis [44]. The recommended sequence is T1WI, T2WI and fat suppression T2WI, coronal and axial scans, with specificity and sensitivity above 99%. The presence of bone marrow edema and joint effusion on T2WI with fat suppression indicates that the disease has advanced to the pre-collapse or subsidence stage.
CT Scanning
Although a coronal and axial two-dimensional reconstruction CT scan is advised, it cannot directly
Stage 4: Collapse of the articular surface and signs of secondary osteoarthritis determine the stage of ONFH but can clearly demonstrate subchondral bone plate fractures, necrosis, and the level of repair [45].
Scintigraphy
With a high sensitivity and low specificity, scintigraphy can offer hints for detecting stage I.
Treatment Methods
Depending on the cause of the condition, different treatments are used.
Nonoperative Treatment
Restricted weight bearing, pharmacological medications, and biophysical therapy methods are included in the nonoperative management of ONFH [46].
Non-Weight Bearing: During the early stages of osteonecrosis of the hip causing ON, restrictions of weight- bearing with a cane, crutches, or walker are beneficial (Ficat and Arlet Stage-I and II) [47].
Bisphosphonates: In osteonecrotic lesions, bisphosphonates are beneficial because they reduce osteoclast activity. When ON hip is treated in early stages, it delays the onset of subchondral fractures or collapses, and when collapse has already occurred, it delays the need for total hip replacement (THR) [48, 49, 50, 51, 52, 53, 54, 55].
Anticoagulants, Statins and Other Vasodilators: The pre-collapse stage of ONFH can be treated with anticoagulants (low molecular weight heparin), fibrinolysis promoters, and vasodilators. Thrombophilia and hypo fibrinolysis can be associated with ON, resulting in venous stasis, decreased arterial flow, increased intraosseous pressure, and hypoxic bone death [56, 57]. Systemic anticoagulation therapy initiated before irreversible segmental collapse of the femur head may be able to stop or, speculatively, reverse the progression of ischemia ON [58, 59]. In cases of idiopathic ON and/or corticosteroid-induced ON, anticoagulant medication has stopped the disease from progressing from the precollapsed stage to the advanced state [60]. Agents that reduce cholesterol are beneficial in ONFH, especially in cases where ON was brought on by steroids [61]. There is also an increase in fat content of the femoral head as a result of steroids causing hyperlipidemia [62]. Sinusoidal collapse and osteonecrosis occur due to increased intracortical pressure. Known as lipid-clearing drugs, statins reduce lipid levels in blood and tissues dramatically.
Physical Therapy: These techniques include extracorporeal shockwaves, high-frequency magnetic field therapy, hyperbaric oxygen therapy, and others.
- Extracorporeal Shock Wave Therapy: It is still unclear exactly how ESWT helps in ONFH. However, researchers claim that it promotes neovascularization by encouraging the expression of angiogenic growth factors [63, 64, 65].
- Pulsed Electromagnetic Therapy: Through promotion of osteogenesis and angiogenesis, similar to ESWT, pulsed electromagnetic therapy is expected to benefit early- stage ON [66, 67, 68, 69, 70]. There is currently little evidence in favour of electromagnetic stimulation, and more study is required to determine its potential impact on early- stage ON.
- Hyperbaric Oxygen: An increase in microcirculation and a decrease in intraosseous pressure are the results of hyperbaric oxygen therapy’s improved oxygenation, vasoconstriction induced edema reduction, and angioneogenesis-induced edema reduction [71, 72, 73].
Surgical Treatment
Core Decompression: The most often used surgical technique for treating early ONFH is core decompression. It boosts neobone development by increasing blood flow to the necrotic area and reducing intraosseous pressure in the femoral head. The outcome of the treatment is heavily reliant on the etiology and radiographic factors such lesion size, location, or collapse [74, 75]. It has been thought to be the only surgical technique for ONFH that is cost effective [76, 77].
Implanting mesenchymal stem cells or using growth factor based therapies as treatments: An very promising strategy for treating ONFH in the precollapsing stage is the application of adult tissue derived mesenchymal stem cells (MSCs) [78]. Numerous studies have shown that people with ONFH have less colony forming units and endothelial progenitor cells than healthy individuals [79, 80]. Additional factors include increased cellular senescence and decreased angiogenesis in ONFH patients due to diminished endothelial progenitor cell migration capacity and cellular senescence [78].
Implantation Methods
Combination of Core Decompression and MSC Transplantation: The most common method for treating ONFH in its early stages is core decompression (CD), which lowers intraosseous pressure, eliminates necrotic tissue, and encourages the growth of new bone [81]. Positive results are only seen in patients with modest necrotic lesions, and core decompression’s effectiveness is inconsistent [82]. Consequently, a typical method for treating ONFH now involves combining core decompression with MSC transplantation. Together in brief, stem cells are separated from the pertinent tissue and then injected, after core decompression, into the necrotic area of the femoral head. Coupled core decompression and autologous bone marrow transplantation improved the Western Ontario and McMaster Universities Arthritis Index (WOMAC), visual analogue scale (VAS), Harris hip score (HHS), clinical score, and mean hip survival, promoted the repair of necrotic areas, reduced the size of lesions, improved the clinical symptoms, and slowed the disease progression of ONFH, according to a few studies [83, 84, 85] (Figure 2).
MSCs Arterial Perfusion: Another approach of treating ONFH is to increase the blood flow to the femoral head by perfusing MSCs through the arterial system. Multiple studies examining the beneficial effects of MSCs on angiogenesis found that arterial perfusion of MSCs encouraged angiogenesis and vascular repair of the femoral head by increasing the expression of VEGF, basic fibroblast growth factor (bFGF), and by increasing microvessel density (MVD), which helped improve the blood supply and renovation of the necrotic area [86, 87, 88].
Cytokine pretreated or gene-modified MSCs transplantation: Numerous cytokines, such as BMP, VEGF, bFGF, and tumor necrosis factor, have been shown in the recent research to contribute to MSCs’ osteogenesis and angiogenesis and to improve the repair of ONFH (TNF). Combination therapy could promote the growth of new bone in the necrotic region and stop the femoral head from collapsing; as a result, cytokines were thought to be used as a pretreatment for MSCs in ONFH [89, 90].
MSCs Transplantation and bone tissue engineering technology: The three main components of bone tissue engineering technology are seed cells, carriers, and scaffolds. Due to their great capacity for differentiation, high levels of proliferative activity, and low immunogenicity, MSCs are the best seed cells for bone tissue creation. In addition to integrating cells and receptors, the carriers or scaffolds can also be employed to support the necrotic area of the femoral head biomechanically, which can be used to regulate cellular function. As a result, a novel strategy for treating ONFH involves combining MSCs with carriers or scaffolds [91].
Role of Stem Cell Therapy
ONFH is a progressive disease that occurs when the blood supply to the femoral head is critically reduced, and intraosseous pressure is elevated. It is well acknowledged that a variety of traumatic and non-traumatic insults affect the femoral head’s already fragile circulation, resulting in bone marrow and osteocyte death—and ultimately the collapse of the necrotic segment. Molecular pathways implicated in the pathophysiology of ONFH have been the subject of recent research. In a study published in Baksh D, et al. [92] showed that multipotent mesenchymal stem cells (MSCs) can differentiate into a variety of cellular types, including osteoblasts, osteocytes, chondrocytes, and adipocytes while still maintaining mitotic proliferation [92]. When implanted in areas of necrotic bone, MSCs have been demonstrated to improve tissue regeneration [93]. According to Hernigou P, et al. [94]. S theory, multipotent MSCs in the bone marrow aspirate could repopulate the trabeculae of the necrotic zone within the femoral head, promoting regeneration and remodelling of the necrotic bone [94]. A study reviewed results implied that the implantation of autologous mesenchymal stem cells (MSCs) into the core decompression track, particularly when used at early (pre-collapse) phases of ONFH, might increase the survival of femoral heads and lessen the need for hip arthroplasty [95].
Nonvascularized Bone Graft
After removing the necrotic lesion from the femoral head, nonvascularized bone-grafts are employed to maintain the subchondral bone and articular cartilage. The osteonecrotic lesion is helped to heal by the osteoconductive and osteoinductive qualities of the bone graft. In precollapse and early postcollapse (2 mm collapse) ONFH cases when the articular cartilage is largely unharmed, this mode of treatment has been reported to be effective. When CD fails in Ficat stages I and II ONFH, the surgeons frequently use this method [58].
Porous Tantalum Implant
Porous tantalum implants offer structural support similar to that of a bone graft while minimizing the risks of infection problems and donor site morbidity associated with using allografts and autografts, respectively. Due to the high level of porosity (>80% volume) in these rods, bone can grow quickly and securely [96, 97, 98, 99].
Vascularized Bone Graft
A suggested mode of treatment for early ONFH is vascularized bone grafting (Ficat stage I to III) [100, 101, 102, 103]. Joint collapse is avoided by the graft, which offers a strong structural support (for example, a vascularized fibula graft or iliac crest graft) [104]. In addition to enhancing bone repair at the site of the necrotic lesion, the graft possesses inherent osteogenic potential and preserves vascularity. The prognosis is less favorable in severe lesions, though, when the collapse is greater than 2 mm and more than 50% of the femoral head is involved. No patients should be considered for the surgery if they have a history of smoking, drinking, peripheral vascular disease, or any other risk factors. This technique’s primary drawbacks are the difficulty of the surgery and the longer surgery time [105, 106, 107, 108].
Vascularized Iliac Crest Graft
When necrosis does not yet encompass the entire femoral head, the procedure described is advised for therapy in Ficat stages II and early III. The use of vascularized iliac crest grafts in ONFH was found to have a 74% success rate (17 of 23 hips) in a research by Iwato H, et al. [104].
Proximal Femoral Osteotomy
The basic idea behind proximal femoral osteotomies in ONFH is to rotate the necrotic femur head away from the area that bears weight and replace it with the healthy, unaffected part of the head. Furthermore, it enhances vascularity and lowers intraosseus venous pressure. There are primarily two types of osteotomies discussed: transtrochanteric rotational osteotomies and intertrochanteric varus or valgus osteotomies (combined with flexion or extension). The reported success rates for these osteotomies range from 70% to 93% [109, 110, 111, 112]. The best candidates for osteotomies are those who are not receiving longterm steroid therapy, have little osteoarthritic alterations, no acetabular involvement or loss of joint space, and a small combined necrotic angle (Kerboul’s angle <200) [20].
Arthroplasty
When all other forms of therapy have failed or the joint is arthritic as a result of advanced collapse, patients with ONFH may require THR (more than 2 mm). Because ONFH victims are typically young individuals with significant functional demands and a high likelihood of needing revision arthroplasty, THR is regarded as a last resort of treatment. Sickle cell disease, Gaucher disease, end-stage kidney illness, and transplant patients all had greater revision rates when the patients were categorized according to their related risk factors. Patients with SLE, those without a known cause, and those who underwent heart surgery had a lower revision rate [20].
Conclusion
Osteonecrosis of the femoral head with subsequent arthrosis is one of the leading conditions for the total hip arthroplasty. It is caused by many conditions which ultimately causes the disruption of blood supply to the femoral head. COVID 19 disease itself and the treatment with steroids for the same, is implicated as a cause for the outbreak of ONFH following COVID 19. During initial stages it causes the collapse of femoral head but in advanced stages it is associated with secondary osteoarthritis results in more disability. The treatment methods vary with stage of the disease. The early stages can be managed with conservative methods and hip preserving surgeries whereas late stage condition with advanced osteoarthritis requires arthroplasty. The early recognition by clinical and radiological features the progression may be reversed or slowed down. The high usage of corticosteroids during COVID 19 and its association with ONFH is a warning sign for the judicious usage of the same in future.
Disclosures
- Acknowledgement: None
- Conflict of interest: None
- Financial disclosures: None to disclose
- Authors’ contribution: RI: Conceptualization, writing, revision, and final approval; RSR: Literature search, revision and final approval.
- Ethical approval: Not required, being a narrative review and not involving any patients data or identity.
References
-
Steinberg ME (1987) Avascular Necrosis of the Femoral Head. In: Tronzo RG (Eds.), Surgery of the Hip Joint. Springer, New York, USA, pp: 1-29.
-
Freund E (1936) Bilateral aseptic necrosis of the femoral head: problems arising in a compensation case. ann surg 104(1): 100-106.
-
Zhao D, Xie H, Xu Y, Wang Y, Yu A, et al. (2017) Management of osteonecrosis of the femoral head with pedicled iliac bone flap transfer: A multicenter study of 2190 patients. Microsurgery 37(8): 896-901.
-
Zheng J, Wang H, Gao Y, Ai Z (2021) A Study on the Evaluation of a Risk Score of Osteonecrosis of the Femoral Head Based on Survival Analysis. J Arthroplasty 36(1): 62-71.
-
Lieberman JR, Berry DJ, Mont MA, Aaron RK, Callaghan JJ, et al. (2003) Osteonecrosis of the hip: Management in the 21st century. Instr Course Lect 52: 337-355.
-
Steinberg ME, Steinberg DR (2014) Osteonecrosis: Historical perspective. In: Koo KH, Mont MA, Jones LC (Eds.), Osteonecrosis_._ Heidelberg, Springer, pp: 3-15.
-
Fukushima W, Fujioka M, Kubo T, Tamakoshi A, Nagai M, et al. (2010) Nationwide epidemiologic survey of idiopathic osteonecrosis of the femoral head. Clin Orthop Relat Res 468(10): 2715-2724.
-
Kang JS, Park S, Song JH, Jung YY, Cho MR, et al. (2009) Prevalence of osteonecrosis of the femoral head: A nationwide epidemiologic analysis in Korea. J Arthroplasty 24(8): 1178-1183.
-
Cooper C, Steinbuch M, Stevenson R, Miday R, Watts NB, et al. (2010) The epidemiology of osteonecrosis: Findings from the GPRD and THIN databases in the UK. Osteoporos Int 21(4): 569-577.
-
Bachiller FG, Caballer AP, Portal LF (2002) Avascular necrosis of the femoral head after femoral neck fracture. Clin Orthop Relat Res 399: 87-109.
-
Powell C, Chang C, Naguwa SM, Cheema G, Gershwin ME, et al. (2010) Steroid induced osteonecrosis: an analysis of steroid dosing risk. Autoimmun Rev 9(11): 721-743.
-
Saito M, Ueshima K, Fujioka M, Ishida M, Goto T, et al. (2014) Corticosteroid administration within 2 weeks after renal transplantation affects the incidence of femoral head osteonecrosis. Acta Orthop 85(3): 266- 270.
-
Li ZR, Sun W, Qu H, Zhou YX, Dou BX, et al. (2005) Clinical research on correlation between osteonecrosis and steroid. Zhonghua Wai Ke Za Zhi 43(16): 1048-1053.
-
Lieberman JR, Berry DJ, Mont MA, et al. (2002) Osteonecrosis of the hip: management in the 21th century. J Bone Joint Surg Am 84(5): 834-853.
-
Wang YS, Li YB, Yin L, Li J, Xiong TB, et al. (2006) The pathogenesis of alcohol‐induced osteonecrosis and the preventive effect of puerarin. Zhonghua Xian Wei Wai Ke Za Zhi 29: 209-212.
-
Korompilias AV, Ortel TL, Urbaniak JR (2004) Coagulation abnormalities in patients with hip osteonecrosis. Orthop Clin North Am 35(3): 265-271.
-
Sun W, Li ZR, Shi ZC, Zhang NF, Zhang YC, et al. (2006) Changes in coagulation and fibrinolysis of post‐SARS osteonecrosis in a Chinese population. Int Orthop 30(3): 143-146.
-
Nakamura J, Harada Y, Oinuma K, Iida S, Kishida S, et al. (2010) Spontaneous repair of asymptomatic osteonecrosis associated with corticosteroid therapy in systemic lupus erythematosus: 10‐year minimum follow‐up with MRI. Lupus 19(11): 1307-1314.
-
Zhao DW, Yang L, Tian FD_, et al_. (2012) Incidence of osteonecrosis of the femoral head in divers: an epidemiologic analysis in Dalian. Zhonghua Gu Ke Za Zhi 32: 521-525.
-
Tripathy SK, Goyal T, Sen RK (2015) Management of femoral head osteonecrosis: Current concepts. Indian J Orthop 49(1): 28-45.
-
Powell C, Chang C, Naguwa SM, Cheema G, Gershwin ME, et al. (2010) Steroid induced osteonecrosis: An analysis of steroid dosing risk. Autoimmun Rev 9(11): 721-743.
-
Assouline-Dayan Y, Chang C, Greenspan A, Shoenfeld Y, Gershwin ME, et al. (2002) Pathogenesis and natural history of osteonecrosis. Semin Arthritis Rheum 32(2): 94-124.
-
LaPorte DM, Mont MA, Mohan V, Jones LC, Hungerford DS, et al. (1998) Multifocal osteonecrosis. J Rheumatol 25(10): 1968-1974.
-
Huang C, Wang Y, Li X, Zhao J, Hu Y, et al. (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395(10223): 497-506.
-
Disser NP, De Micheli AJ, Schonk MM, Konnaris MA, Piacentini AN, et al. (2020) Musculoskeletal Consequences of COVID-19. J Bone Jt Surg Am 102(14): 1197-1204.
-
Griffith JF (2011) Musculoskeletal complications of severe acute respiratory syndrome. Semin Musculoskelet Radiol 15(5): 554-560.
-
Salvio G, Gianfelice C, Firmani F, Lunetti S, Balercia G, et al. (2020) Bone Metabolism in SARS-CoV-2 Disease: Possible Osteoimmunology and Gender Implications. Clin Rev Bone Miner Metab 18(4): 51-57.
-
Tao H, Bai J, Zhang W, Zheng K, Guan P, et al. (2020) Bone biology and COVID-19 infection: Is ACE2 a potential influence factor. Med Hypotheses 144: 110178.
-
Barlow A, Landolf KM, Barlow B, Yeung SYA, Heavner JJ, et al. (2020) Review of Emerging Pharmacotherapy for the Treatment of Coronavirus Disease 2019. Pharmacother J Hum Pharmacol Drug Ther 40(5): 416-437.
-
Liu J, Li S, Liang B, Wang X, Wang H, et al. (2020) Longitudinal characteristics of lymphocyte responses and cytokine profiles in the peripheral blood of SARS- CoV-2 infected patients. EBioMedicine 55: 102763.
-
Shen J, Liang BL, Zeng QS, Chen JY, Liu QY, et al. (2004) Report on the investigation of lower extremity osteonecrosis with magnetic resonance imaging in recovered severe acute respiratory syndrome in Guangzhou. Zhonghua Yi Xue Za Zhi 84(21): 1814-1817.
-
Agarwala SR, Vijayvargiya M, Pandey P (2021) Avascular necrosis as a part of long COVID-19. BMJ Case Rep 14(7): e242101.
-
Shah KN, Racine J, Jones LC, Aaron RK (2015) Pathophysiology and risk factors for osteonecrosis. Curr Rev Musculoskelet Med 8(3): 201-209.
-
Gasbarra E, Perrone FL, Baldi J, Bilotta V, Moretti A, et al. (2015) Conservative surgery for the treatment of osteonecrosis of the femoral head: current options. Clin Cases Miner Bone Metab 12(1): 43-50.
-
Hungerford DS (1979) Bone marrow pressure, venography and core decompression in ischemic necrosis of the femoral head. In: Riley LH (Eds.), the Hip: Proceedings of the Seventh Open Scientific Meeting of the Hip Society. St Louis, MO: CV Mosby, pp: 218-237.
-
Carli A, Albers A, Seguin C, Harvey EJ (2014) the medical and surgical treatment of ARCO Stage-I and II osteonecrosis of the femoral head: a critical analysis review. JBJS Rev 2(2): 1-10.
-
Mont MA, Hungerford DS (1995) Non-traumatic avascular necrosis of the femoral head. J Bone Joint Surg Am 77(3): 459-474.
-
Nam KW, Kim YL, Yoo JJ, Koo KH, Yoon KS, et al. (2008) Fate of untreated asymptomatic osteonecrosis of the femoral head. J Bone Joint Surg Am 90(3): 477-484.
-
Lieberman JR, Engstrom SM, Meneghini RM, SooHoo NF (2012) Which factors influence preservation of the osteonecrotic femoral head. Clin Orthop Relat Res 470(2): 525-534.
-
Nishii T, Sugano N, Ohzono K, Sakai T, Sato Y, et al. (2002) Significance of lesion size and location in the prediction of collapse of osteonecrosis of the femoral head: a new three-dimensional quantification using magnetic resonance imaging. J Orthop Res 20(1): 130-136.
-
Sugano N, Takaoka K, Ohzono K, Matsui M, Masuhara K, et al. (1994) Prognostication of nontraumatic avascular necrosis of the femoral head. Significant of location and size of the necrotic lesion. Clin Orthop Relat Res 303: 155-164.
-
Hernigou P, Lambotte JC (2001) Volumetric analysis of osteonecrosis of the femur. Anatomical correlation using MRI. J Bone Joint Surg Br 83(5): 672-675.
-
Kishida Y, Nishii T, Sugano N, Nakanishi K, Sakai T, et al. (2003) Measurement of lesion area and volume by three-dimensional spoiled gradient-echo MR imaging in osteonecrosis of the femoral head. J Orthop Res 21(5): 850-858.
-
Sugano N, Kubo T, Takaoka K, Ohzono K, Hotokebuchi T, et al. (1999) Diagnostic criteria for non-traumatic osteonecrosis of the femoral head: a multicentre study. J Bone Joint Surg Br 81(4): 590-595.
-
Stevens K, Tao C, Lee SU, et al. (2003) Subchondral fractures in osteonecrosis of the femoral head: comparison of radiography, CT, and MR imaging. AJR Am J Roentgenol 180(2): 363-368.
-
Konishiike T, Makihata E, Tago H, Sato T, Inoue H, et al. (1999) Acute fracture of the neck of the femur. An assessment of perfusion of the head by dynamic MRI. J Bone Joint Surg Br 81(4): 596-599.
-
Mont MA, Cherian JJ, Sierra RJ, Jones LC, Lieberman JR. Nontraumatic Osteonecrosis of the Femoral Head: Where Do We Stand Today? A Ten-Year Update. J Bone Joint Surg Am. 2015 Oct 7;97(19):1604-27.
-
Agarwala S, Jain D, Joshi VR, Sule A (2005) Efficacy of alendronate, a bisphosphonate, in the treatment of AVN of the hip. A prospective open-label study. Rheumatology Oxford 44: 352-359.
-
Agarwala S, Shah S, Joshi VR (2009) the use of alendronate in the treatment of avascular necrosis of the femoral head: Followup to eight years. J Bone Joint Surg Br 91(8): 1013-1018.
-
Agarwala S, Shah SB (2011) Ten-year followup of avascular necrosis of femoral head treated with alendronate for 3 years. J Arthroplasty 26(7): 1128- 1134.
-
Nishii T, Sugano N, Miki H, Hashimoto J, Yoshikawa H, et al. (2006) Does alendronate prevent collapse in osteonecrosis of the femoral head. Clin Orthop Relat Res 443: 273-279.
-
Lai KA, Shen WJ, Yang CY, Shao CJ, Hsu JT, et al. (2005) The use of alendronate to prevent early collapse of the femoral head in patients with nontraumatic osteonecrosis. A randomized clinical study. J Bone Joint Surg Am 87(10): 2155-2159.
-
Chen CH, Chang JK, Lai KA, Hou SM, Chang CH, et al. (2012) Alendronate in the prevention of collapse of the femoral head in nontraumatic osteonecrosis: A two-year multicenter, prospective, randomized, double-blind, placebo-controlled study. Arthritis Rheum 64(5): 1572- 1578.
-
Kang P, Pei F, Shen B, Zhou Z, Yang J, et al. (2012) Are the results of multiple drilling and alendronate for osteonecrosis of the femoral head better than those of multiple drilling? A pilot study. Joint Bone Spine 79(1): 67-72.
-
Wong T, Wang CJ, Hsu SL, Chou WY, Lin PC, et al. (2008) Cocktail therapy for hip necrosis in SARS patients. Chang Gung Med J 31(6): 546-553.
-
Glueck CJ, Freiberg RA, Fontaine RN, Sieve-Smith L, Wang P, et al. (2001) Anticoagulant therapy for osteonecrosis associated with heritable hypofibrinolysis and thrombophilia. Expert Opin Investig Drugs 10(7): 1309- 1316.
-
Glueck CJ, Freiberg RA, Fontaine RN, Tracy T, Wang P, et al. (2005) Hypofibrinolysis, thrombophilia, osteonecrosis. Clin Orthop Relat Res 386: 19-33.
-
Banerjee S, Issa K, Pivec R, Kapadia BH, Khanuja HS, et al. (2013) Osteonecrosis of the hip: Treatment options and outcomes. Orthop Clin North Am 44(4): 463-476.
-
Glueck CJ, Freiberg RA, Sieve L, Wang P (2005) Enoxaparin prevents progression of stages I and II osteonecrosis of the hip. Clin Orthop Relat Res 435: 164-170.
-
Chotanaphuti T, Thongprasert S, Laoruengthana A (2013) Low molecular weight heparin prevents the progression of precollapse osteonecrosis of the hip. J Med Assoc Thai 96(10): 1326-1330.
-
Oinuma K, Harada Y, Nawata Y, Takabayashi K, Abe I, et al. (2000) Sustained hemostatic abnormality in patients with steroid-induced osteonecrosis in the early period after high-dose corticosteroid therapy. J Orthop Sci 5(4): 374-379.
-
Wang GJ, Cui Q, Balian G (2000) The Nicolas Andry award. The pathogenesis and prevention of steroid-induced osteonecrosis. Clin Orthop Relat Res 370: 295-310.
-
Rajpura A, Wright AC, Board TN (2011) Medical management of osteonecrosis of the hip: A review. Hip Int 21(4): 385-392.
-
Ma HZ, Zeng BF, Li XL (2007) Upregulation of VEGF in subchondral bone of necrotic femoral heads in rabbits with use of extracorporeal shock waves. Calcif Tissue Int 81(2): 124-131.
-
Wang CJ, Huang CC, Wang JW, Wong T, Yang YJ (2012) Long term results of extracorporeal shockwave therapy and core decompression in osteonecrosis of the femoral head with eight- to nine-year followup. Biomed J 35(6): 481-485.
-
Eftekhar NS, Schink-Ascani MM, Mitchell SN, Bassett CA (1983) Osteonecrosis of the femoral head treated by pulsed electromagnetic fields (PEMFs): A preliminary report. Hip pp: 306-330.
-
Aaron RK, Lennox D, Bunce GE, Ebert T (1989) The conservative treatment of osteonecrosis of the femoral head. A comparison of core decompression and pulsing electromagnetic fields. Clin Orthop Relat Res 249: 209- 218.
-
Bassett CA, Schink-Ascani M, Lewis SM (1989) Effects of pulsed electromagnetic fields on Steinberg ratings of femoral head osteonecrosis. Clin Orthop Relat Res 246: 172-185.
-
Aaron RK, Steinberg ME (1991) Electrical stimulation of osteonecrosis of the femoral head. Semin Arthroplasty 2: 214-221.
-
Massari L, Fini M, Cadossi R, Setti S, Traina GC (2006) Biophysical stimulation with pulsed electromagnetic fields in osteonecrosis of the femoral head. J Bone Joint Surg Am 88(3): 56-60.
-
Reis ND, Schwartz O, Militianu D, Ramon Y, Levin D, et al. (2003) Hyperbaric oxygen therapy as a treatment for stage-I avascular necrosis of the femoral head. J Bone Joint Surg Br 85(3): 371-375.
-
Camporesi EM, Vezzani G, Bosco G, Mangar D, Bernasek TL (2010) Hyperbaric oxygen therapy in femoral head necrosis. J Arthroplasty 25(6): 118-123.
-
Kot J, Mathieu D (2011) Controversial issues in hyperbaric oxygen therapy: A European Committee for Hyperbaric Medicine Workshop. Diving Hyperb Med 41(2): 101-104.
-
Ficat RP, Arlet J (1980) Ischemia and Necroses of Bone. In: Hungerford DS, editor. Baltimore: Williams and Wilkins.
-
Hungerford DS (1983) Treatment of ischemic necrosis of the femoral head. In: Evarts CD, editor. Sugery of the Musculoskeletal System. Vol. 3. New York: Churchill Livingstone pp: 5029–5043.
-
Soohoo NF, Vyas S, Manunga J, Sharifi H, Kominski G, et al. (2006) Cost-effectiveness analysis of core decompression. J Arthroplasty 21(5): 670-681.
-
Wang GJ, Dughman SS, Reger SI, Stamp WG (1985) The effect of core decompression on femoral head blood flow in steroid-induced avascular necrosis of the femoral head. J Bone Joint Surg Am 67(1): 121-124.
-
Rackwitz L, Eden L, Reppenhagen S, Reichert JC, Jakob F, et al. (2012) Stem cell- and growth factor-based regenerative therapies for avascular necrosis of the femoral head. Stem Cell Res Ther 3(1): 7.
-
Hernigou P, Beaujean F, Lambotte JC (1999) Decrease in the mesenchymal stem-cell pool in the proximal femur in corticosteroid-induced osteonecrosis. J Bone Joint Surg Br 81(2): 349-355.
-
Feng Y, Yang SH, Xiao BJ, Xu WH, Ye SN, et al. (2010) Decreased in the number and function of circulation endothelial progenitor cells in patients with avascular necrosis of the femoral head. Bone 46(1): 32-40.
-
Mont MA, Ragland PS, Etienne G (2004) Core decompression of the femoral head for osteonecrosis using percutaneous multiple small-diameter drilling. Clin Orthop Relat Res 429: 131-138.
-
Rajagopal M, Balch Samora J, Ellis TJ (2012) Efficacy of core decompression as treatment for osteonecrosis of the hip: a systematic review. Hip Int 22(5): 489-493.
-
Tabatabaee RM, Saberi S, Parvizi J, Mortazavi SM, Farzan M (2015) Combining concentrated autologous bone marrow stem cells injection with Core decompression improves outcome for patients with early-stage osteonecrosis of the femoral head: a comparative study. J Arthroplasty 30(9): 11-15.
-
Rastogi S, Sankineani SR, Nag HL, Mohanty S, Shivanand G, et al. (2013) Intralesional autologous mesenchymal stem cells in management of osteonecrosis of femur: a preliminary study. Musculoskelet Surg 97(3): 223–228.
-
Sen RK, Tripathy SK, Aggarwal S, Marwaha N, Sharma RR, et al. (2012) Early results of core decompression and autologous bone marrow mononuclear cells instillation in femoral head osteonecrosis: a randomized control study. J Arthroplasty 27(5): 679-686.
-
Kinnaird T, Stabile E, Burnett MS, Lee CW, Barr S, et al. (2004) Marrow-derived stromal cells express genes encoding a broad spectrum of arteriogenic cytokines and promote in vitro and in vivo arteriogenesis through paracrine mechanisms. Circ Res 94(5): 678-685.
-
Qian HG, Zhu DX, Zhu JZ, Zhao JD, Miao ZN (2008) Promotive effect of autologous bone marrow mesenchymal stem cell transplantation on angiogenesis in rabbit ischemic limbs. J Clin Rehabilitative Tissue Eng Res 12: 10095-10097.
-
Jin H, Xia B, Yu N, He B, Shen Y, et al. (2012) The effects of autologous bone marrow mesenchymal stem cell arterial perfusion on vascular repair and angiogenesis in osteonecrosis of the femoral head in dogs. Int Orthop 36(12): 2589-2596.
-
Zuo SL, Gong YK (2012) Application and prospect of bone marrow mesenchymal stem cells and cytokines in the treatment of femoral head necrosis. Chin J Tissue Eng Res 16: 2621-26214.
-
Wang ZL, He RZ, Tu B, He JS, Cao X, et al. (2018) Drilling combined with adipose-derived stem cells and bone morphogenetic protein-2 to treat femoral head epiphyseal necrosis in juvenile rabbits. Curr Med Sci 38(2): 277-288.
-
Xu Y, Jiang Y, Xia C, Wang Y, Zhao Z, et al. (2020) Stem cell therapy for osteonecrosis of femoral head: Opportunities and challenges. Regen Ther 15: 295-304.
-
Baksh D, Song L, Tuan RS (2004) Adult mesenchymal stem cells: characterization, differentiation and application in cell and gene therapy. J Cell Mol Med 8(3): 301-316.
-
Yan Z, Hang D, Guo C, Chen Z (2009) Fate of mesenchymal stem cells transplanted to osteonecrosis of femoral head. J Orthop Res 27(4): 442-446.
-
Hernigou P, Manicom O, Poignard A, Nogier A, Filippini P, et al. (2004) Core decompression with marrow stem cells. Operative Tech Orthop 14(2): 68-74.
-
Papakostidis Costas, Tosounidis Theodoros H, Jones Elena, Giannoudis Peter V (2016) The role of “cell therapy” in osteonecrosis of the femoral head. Acta Orthopaedica, 87(1): 72-78.
-
Veillette CJ, Mehdian H, Schemitsch EH, McKee MD (2006) Survivorship analysis and radiographic outcome following tantalum rod insertion for osteonecrosis of the femoral head. J Bone Joint Surg Am 88(3): 48-55.
-
Shuler MS, Rooks MD, Roberson JR (2007) Porous tantalum implant in early osteonecrosis of the hip: preliminary report on operative, survival, and outcomes results. J Arthroplasty 22(1): 26-31.
-
Floerkemeier T, Thorey F, Daentzer D, Lerch M, Klages P, et al. (2011) Clinical and radiological outcome of the treatment of osteonecrosis of the femoral head using the osteonecrosis intervention implant. Int Orthop 35(4): 489-95.
-
Babis GC, Sakellariou V, Parvizi J, Soucacos P (2011) Osteonecrosis of the femoral head. Orthopedics 34(1): 39.
-
Meyers MH (1978) The treatment of osteonecrosis of the hip with fresh osteochondral allografts and with the muscle pedicle graft technique. Clin Orthop Relat Res 130: 202-209.
-
Lee CK, Rehmatullah N (1981) Muscle-pedicle bone graft and cancellous bone graft for the “silent hip” of idiopathic ischemic necrosis of the femoral head in adults. Clin Orthop Relat Res 158: 185-194.
-
Baksi DP (1991) Treatment of osteonecrosis of the femoral head by drilling and muscle-pedicle bone grafting. J Bone Joint Surg Br 73(2): 241-245.
-
Iwata H, Torii S, Hasegawa Y, Itoh H, Mizuno M, et al. (1993) Indications and results of vascularized pedicle iliac bone graft in avascular necrosis of the femoral head. Clin Orthop Relat Res 295: 281-288.
-
Matsusaki H, Noguchi M, Kawakami T, Tani T (2005) Use of vascularized pedicle iliac bone graft combined with transtrochanteric rotational osteotomy in the treatment of avascular necrosis of the femoral head. Arch Orthop Trauma Surg 125(2): 95-101.
-
Zhang C, Zeng B, Xu Z, Song W, Shao L, et al. (2005) Treatment of femoral head necrosis with free vascularized fibula grafting: A preliminary report. Microsurgery 25(4): 305-309.
-
Marciniak D, Furey C, Shaffer JW (2005) Osteonecrosis of the femoral head. A study of 101 hips treated with vascularized fibular grafting. J Bone Joint Surg Am 87(4): 742-747.
-
Yoo MC, Kim KI, Hahn CS, Parvizi J (2008) Long term followup of vascularized fibular grafting for femoral head necrosis. Clin Orthop Relat Res 466(5): 1133-1140.
-
Aldridge JM, Urbaniak JR (2008) Vascularized fibular grafting for osteonecrosis of the femoral head with unusual indications. Clin Orthop Relat Res 466(5): 1117-1124.
-
Sen RK (2009) Management of avascular necrosis of femoral head at pre-collapse stage. Indian J Orthop 43(1): 6-16.
-
Sugioka Y, Katsuki I, Hotokebuchi T (1982) Transtrochanteric rotational osteotomy of the femoral head for the treatment of osteonecrosis. Followup statistics. Clin Orthop Relat Res 169: 115-126.
-
Hasegawa Y, Sakano S, Iwase T, Iwasada S, Torii S, et al. (2003) Pedicle bone grafting versus transtrochanteric rotational osteotomy for avascular necrosis of the femoral head. J Bone Joint Surg Br 85(2): 191-198.
-
Sugioka Y, Hotokebuchi T, Tsutsui H (1992) Transtrochanteric anterior rotational osteotomy for idiopathic and steroid-induced necrosis of the femoral head. Indications and long term results. Clin Orthop Relat Res 277: 111-120.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results