Characterizing Fracture Distribution by Sex, Age, and Body Region: Insights from a Regional Population Study
This Rio Grande Valley region of South Texas is a unique, medically underserved region. We conducted this study to further the knowledge of orthopedics in this community and determine if certain body regions, based on sex and age, were at increased risk for fracture in this population. We hypothesized that females would have increased fracture frequency at older ages while males would have increased fracture frequency at younger ages. We also hypothesized that femur and forearm fractures would be increased in females compared to males. This study was a retrospective chart review from January 1, 2018, to September 4, 2024. We analyzed medical charts of individuals who sustained fractures of various regions of the body. Various statistical tests were utilized to analyze the data. Female’s most frequent fracture site is the forearm (27%). Males’ most frequent fracture site is the hand (30%). Females had a bimodal distribution, one peak in early childhood and another peak in older ages. The age distribution in males was unimodal and more uniform with a prominent peak occurring in early childhood. The most frequent co-occurrences were in hand and femur, with 432 cases (5%). These findings suggest that individuals should be mindful and possibly take precautions to prevent fractures in particular body regions based on the age and sex of individuals. Physicians and other healthcare workers should also keep this information in mind when evaluating, informing, and treating patients, especially those with bone conditions or those at higher risk of bone injury.
Introduction
Fractures
Fractures may refer to various bone disruptions, from a small hairline fracture to a compound fracture or a comminuted fracture [1]. Fractures are typically caused by trauma, which may be either considerable such as a fractured pelvis following a road accident, or minor and recurrent as seen with metatarsal fractures in ballerinas or long-distance athletes [1], Moreover, fractures may occur at any point in an individual’s lifetime, but the common causes may vary based on age range [1], The visual presentation of individuals may also vary from minor to severe, such as someone coming in on foot several days after an incident or on a stretcher after a major car accident [1], Most people who sustain a fracture make a full recovery and can resume their usual routine after healing has commenced [2]. However, some fractures may have a significant, long-term impact on an individual’s life, especially if concomitant injuries were sustained with the fracture [2].
Skull and Facial Bones
Most patients with facial trauma are male and have a mean age ranging from 24.6 to 51.0 years [3]. The most common causes of facial fracture are assault, traffic accidents, and falls [3], A fracture of the skull is common after vehicle accidents, falls, fights, and sports injuries [4]. Overall, skull fractures are more common in children because their skulls are thinner and more fragile compared to full-grown adults [4], At the other end of the age spectrum, adults 75 years or older are also at a higher risk of skull fractures because of frequent falls [4], However, individuals of any age are more likely to sustain a skull fracture if they engage in high-risk activities such as contact sports [4].
Cervical Vertebrae
The cervical vertebrae are tasked with maintaining a range of motion for the head and neck as well as protecting nervous innervation to the entire body [5]. In trauma patients, fractures of the cervical spine are a leading cause of mobility and mortality, and bone fractures are associated with 56% of cervical spinal cord injuries [5], Fractures of the cervical vertebrae result from various abnormal movements or a combination of such movements such as hyperflexion, hyperextension, axial loading, rotation, and lateral bending of the spinal column [5], Although they may occur in all age groups, cervical spine fractures are more common in males [5], The most common cause of cervical fractures are falls, followed by motor vehicle accidents, biking, and diving with mortality ranging from 5-10% [5].
Ribs, Sternum, or Thoracic Spine
Most rib and sternal fractures result from blunt trauma to the chest [6, 7]. The incidence and prevalence of rib fractures vary depending on the injury and severity of the trauma [6], Adults are more likely to sustain a rib fracture due to children having more elastic ribs [6], The elderly also tend to be more prone to rib fractures and have a higher mortality and morbidity compared to individuals of younger age [6], Sternal fractures are slightly more prevalent in women than men and are more common in older patients, which is likely due to the elastic chest wall of younger individuals [7], However, younger patients are more likely to sustain intrathoracic injury due to their sternum being less effective at absorbing the energy of impact [7], Regarding thoracic vertebrae fractures, they are underrepresented in current literature with most studies focusing on the thoracolumbar spine. Some of the most common mechanisms for thoracolumbar traumatic injuries include motor vehicle accidents, falls from height, recreational injuries, and work- related injuries [8]. Most of these injuries are high-velocity and high-energy injuries, typically involving additional injuries [8], Thoracolumbar traumatic injury has a median age of 35, with up to 75% of all spine fractures occurring in the T10-L2 region [8].
Lumbar Spine or Pelvis
The lumbar vertebrae, like the thoracic vertebrae, are underrepresented in current literature with most studies focusing on the thoracolumbar spine. The mechanisms and epidemiology of thoracolumbar injuries are as discussed previously in the “Rib, Sternum, and Thoracic Spine” section. Regarding the pelvis, fractures are often a result of high- impact trauma such as motor vehicle accidents and are frequently accompanied by other injuries elsewhere in the body [9].
However, these fractures may also arise from low- impact trauma such as during athletic activities and falls in the elderly [9], In the United States, pelvic fractures are approximated to occur in 37 out of 100,000 individuals per year with the incidence being highest in individuals ages 15 to 28 [9], In terms of sex, men younger than 35 years of age and women older than 35 years of age are most commonly affected [9].
Shoulder and Upper Arm
Proximal humerus fractures (PHFs) account for 5 to 6 percent of all adult fractures and often occur in elderly individuals who experience low-energy falls with these events contributing to the global impact of direct and indirect costs of osteoporosis and fragility fractures [10]. The overall incidence of these fractures is estimated to be around 4% to 6% with a 2:1 female to male ratio [10], Moving down the humerus, humeral shaft fractures comprise 1-5% of all bony fractures, with these fractures having a bimodal age distribution where individuals most vulnerable are in the 3rd or 7th decade of life [11]. Around 70% of individuals with humeral shaft fractures younger than 50 years are men, whereas around 70% of individuals older than 50 years are women [11], In younger individuals, these fractures are mostly due to high-energy trauma while in older individuals, the damage is typically caused by low-impact forces [11], Further down the upper arm, distal humerus fractures in the adult population represent about 2% of all fractures and generally present in a bimodal distribution as either younger males or elderly females [12]. Like other humerus fractures, they are typically the result of high-energy trauma in younger populations and low-energy falls in elderly populations [12].
Forearm
Fractures of the forearm are commonly seen in trauma and emergencies, especially in the pediatric age group, with such injuries occurring because of direct as well as indirect trauma [13]. The most common mechanism of this injury is axial loading applied to the forearm (fall on an outstretched hand), while other common modes of injury include motor vehicle accidents, athletic injuries, and falls from height [13], Forearm fractures occur commonly in the pediatric population, with an incidence of around 1 in 100 children each year, with the peak incidence occurring in the 5 to 14 years age range, accounting for around 34% of the fractures [13], In the adult population, the incidence is most common between 25 to 34 years of age [13], The most common site for forearm fractures is the distal end of the ulna or radius, and the least common location being the proximal end of these bones [13].
Wrist or Hand
Although distal radius fractures may be included as wrist fractures in some studies, the ICD-10 code for wrist and hand fractures (S62), as used in this study, only includes carpal bones and the bones distal to them. Hand and wrist fractures comprise about a fifth of all fractures treated in an emergency setting with an annual incidence of about 3–4 incidents per 100,000 people [14]. Compared to fractures of the metacarpals and phalanxes, carpal fractures are rare, comprising only 8% of these hand and wrist fractures [14], Metacarpal fractures occur via various mechanisms, most sustained in contact-sport athletes such as football players and boxers, and manual laborers [15]. These fractures are the third most common fracture of the upper extremity and are the second most common hand fractures behind the phalanxes, accounting for around 40% of all hand injuries [15], Gender appears to be a significant variable, as 76% of metacarpal injuries occur in males [15], Phalanx fractures are some of the most common fractures, second most in the upper extremity, and most common fracture of the hand [15, 16]. They also present with numerous complications regardless of treatment and are often related to blunt, penetrating, or crush trauma [16], the incidence of phalanx fractures is approximately 0.012% of people per year in the United States, being more common in males than females in both children and adults [16].
Femur
The femoral head articulates with the acetabulum to make the hip joint, and this junctional location makes the femoral neck prone to fracture [17]. This fracture is a very common type of fracture, with around 1.6 million occurring annually [17], Considerable risk factors include female gender (especially white females), low bone density, and decreased mobility [17], Femoral shaft fractures are also common among orthopedic injuries, mostly due to automobile accidents, falls from heights, ground-level falls in individuals with osteoporosis, and gunshots [18]. The incidence of these fractures worldwide is around 10 and 21 per 100,000 per year, demonstrating a bimodal distribution [18], This injury is more likely to occur in men between the ages of 15 to 35, while women begin to show a steady increase starting at age 60 [18], Moving distally, distal femur fractures, although not as common, require prompt diagnosis and treatment to prevent high morbidity and mortality correlated to the fracture [19]. These fractures account for less than 1% of all fractures and only about 3 to 6% of all femoral fractures [19], They occur in a bimodal distribution with young males and elderly females [19].
Lower Leg or Ankle
Tibial shaft fractures are the most common long bone fractures and occur in 4 percent of the elderly population [20]. These fractures occur in a bimodal pattern involving both low-energy and high-energy mechanisms such as direct trauma [20], On the other hand, although fibula fractures are relatively common as well, they are rare when not associated with concomitant ligament or tibia injuries [21]. Fibula shaft fractures are commonly associated with damage to the peroneal nerve as it runs near the fibula on the lateral and anterior side of the leg [21], Further down, ankle injuries may result from crush and twisting injuries in both the elderly as well as the young patient population [22]. The incidence of ankle fractures in adults is around 187 per 100000 adults every year [22], The highest incidence in the male population is between 15 to 24 years of age, while in the female population it is between 75 and 84 years of age [22].
Foot and Toe
Although there are several tarsal bones, the calcaneus is the most fractured, primarily involved in around 60% of tarsal fractures [23]. In the United States, 90% of these fractures occur in middle aged men, especially those who work in construction or industrial jobs [23], moving distally, fractures of the metatarsals (forefoot) and phalanges of the foot (toes) are common and may result from a direct trauma such as kicking something or dropping a heavy object on these bones [24]. They may also occur due to repetitive stress and overuse such as competitive participation in high- impact sports [24], the fifth metatarsal is the most fractured, followed by the third metatarsal [25]. Metatarsal fractures also consist of 61% of foot fractures in children [25].
Study Significance and Aim
This Rio Grande Valley (RGV) region of South Texas is a unique region that is impoverished, medically underserved, has a substantial population of undocumented immigrants, and has a high prevalence of various chronic conditions such as diabetes and obesity [26, 27, 28]. The construct of machismo is another factor that may further contribute to the health of this population as this may deter Hispanic males from seeking medical help due to it being perceived as feminine [29]. To our knowledge, there is no study that has analyzed fractures by body region in this population. We conducted this study to further the knowledge of orthopedics in this unique, medically underserved community. We sought to characterize the distribution of fractures in RGV as a function of sex and age. We hypothesized that females would have increased fracture frequency at older ages while males would have increased fracture frequency at younger ages. We also hypothesized that femur and forearm fractures would be increased in females compared to males.
Material and Methods
Study Design and Data Collection
This was a retrospective chart review and IRB approval was obtained prior to starting this study. Data was gathered from the University of Texas Rio Grande Valley (UTRGV) UTHealth electronic database. Data collection included medical charts from January 1, 2018, to September 4, 2024. We collected and analyzed medical charts of individuals who sustained fractures of skull and facial bones, cervical vertebrae, ribs, sternum, or thoracic spine, lumbar spine or pelvis, shoulder and upper arm, forearm, wrist or hand, femur, lower leg or ankle, as well as foot and toe. The various regions of fracture were obtained by using ICD-10 diagnosis codes. The codes were as follows (ICD-10 codes): skull and facial bones (S02), cervical vertebrae (S12), ribs, sternum, or thoracic spine (S22), lumbar spine or pelvis (S32), shoulder and upper arm (S42), forearm (S52), wrist or hand (S62), femur (S72), lower leg or ankle (S82), foot and toe (S92). For each patient, various demographics were collected, including BMI, sex, age at diagnosis, race/ethnicity, county of residence, and marital status.
Inclusion and Exclusion Criteria
Individuals over the age of 90 were not included in the study due to the small number of these individuals. UTRGV did not allow us to analyze these individuals due to the increased risk of identifying these individuals’ identities. Individuals who were not seen by a UTRGV associated institution were not included in the study. If there were duplications of an individual’s medical chart, such as an individual having more than one appointment, the earliest date, the date the patient was diagnosed with any of the analyzed fracture regions, was included. If an individual was diagnosed with more than one of the fracture regions analyzed, all conditions were included and analyzed based on the date of diagnosis and demographics of the patient at the point in time of that specific diagnosis.
Data Analysis
We used descriptive statistics, including frequencies and percentages, median values, and quantile distribution. The distribution was visualized with histograms and dot plots. The number of fractures was analyzed with negative binomial regression. The hazard ratio for the five most common fractures was analyzed to compare sexes and modeled over age, and proportional risk was tested. All analyses were performed with Stata version 18.5 (StataCorp, College Station, TX).
Results
Figure 1 shows a skeleton representation of the significant body regions with the locations of fractures and their respective frequencies by sex. Female’s most frequent fracture site is the forearm (27%), followed by the shoulder (17%) and ankle (16%). The hand (16%) and femur (12%) are also common fracture sites. Less frequent fractures include the foot/toe (8%), thorax (1%), and cervical region/ skull (<1%) (Table 1 and Figure 1). Male’s most frequent fracture site is the hand (30%), followed by the forearm (22%) and shoulder (15%). The ankle (12%), foot/toe (6%), and femur (12%) are less common. No sex differences were found in the thorax (1%), and cervical region/skull (<1%). These results may be seen in Table 1 and Figure 1.
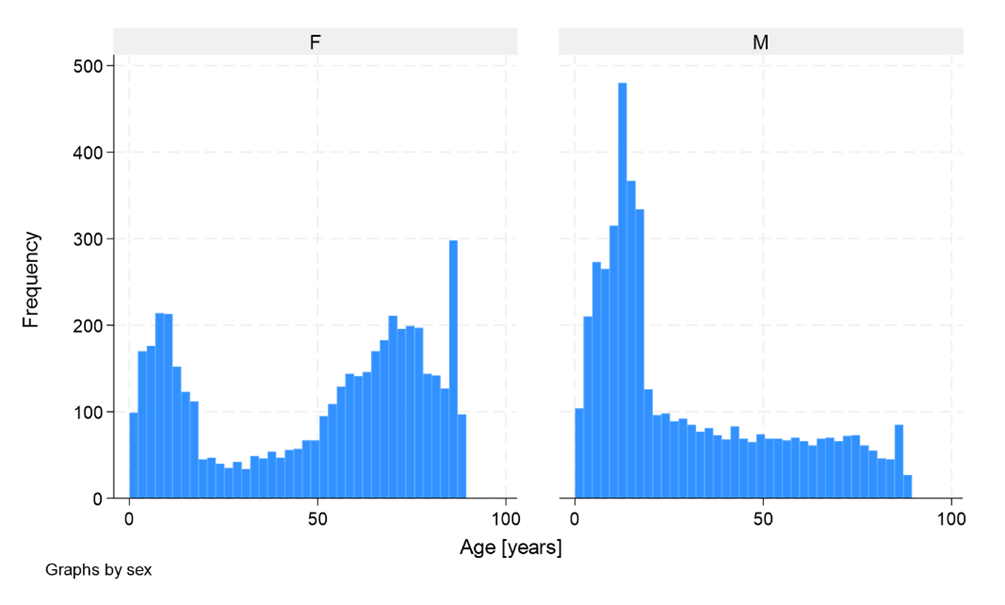
The lifetime distribution of fractures by sex and age showed that females had a bimodal distribution, one peak in early childhood (likely around 0–15 years) and another peak in older ages, especially after 50, with a significant rise toward older age groups. There was a clear dominance of fractures in older females compared to younger females (Figure 2). The age distribution in males was unimodal and more uniform than that of females. The most prominent peak occurs in early childhood (0–15 years), but the frequency of fractures stays stable or slightly declines gradually across the lifespan, with fewer fractures observed at older ages (above 50 years) (Figure 2).
Most fractures were unique to one site, with significant percentages for the forearm (24%), hand (19%), shoulder (16%), and ankle (14%). Other sites, such as the femur (7%) and foot/toe (7%), had lower frequencies, while sites like the pelvis (1%), thorax (<1%), skull (<1%), and cervical (<1%) were much less common. The most frequent co-occurrences were in the hand and femur, with 432 cases (5%), followed by the forearm and hand, with 127 cases (1%). Fractures in less common sites like the thorax, skull, and cervical region showed minimal co-occurrence (Table 2).
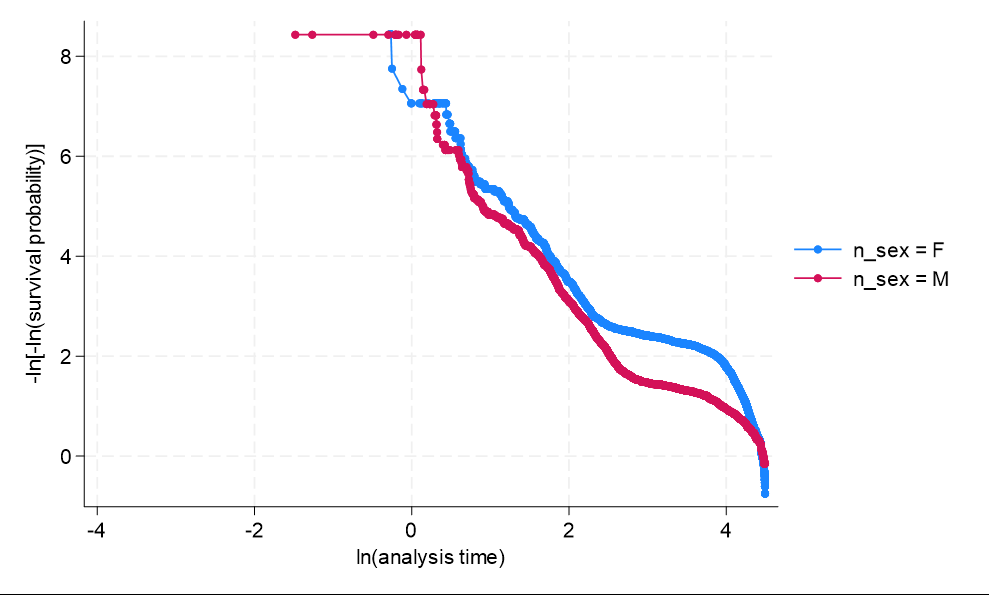
The negative binomial analysis did not show any satisfactory predictor. The hazard ratio between sexes for the five most common fractures showed a higher risk of fractures for males. The test for proportional ratios showed the risk of fractures by sex changes over time. Figure 3 shows that the proportional hazards for males and females are not parallel, suggesting that the relative risk of fractures between males and females changes over time (Figure 3).
| Female | Males | Total | Ratio F/M | |
|---|---|---|---|---|
| Forearm | 1420 (27%) | 1177 (22%) | 2597 (25%) | 1.21* |
| Hand | 833 (16%) | 1554 (30%) | 2387 (23%) | 0.54* |
| Shoulder | 900 (17%) | 797 (15%) | 1697 (16%) | 1.13* |
| Ankle | 844 (16%) | 645 (12%) | 1489 (14%) | 1.31* |
| Femur | 642 (12%) | 618 (12%) | 1260 (12%) | 1.04 |
| Foot toe | 424 (8%) | 295 (6%) | 719 (7%) | 1.44* |
| Pelvis | 109 (2%) | 63 (1%) | 172 (2%) | 1.74* |
| Thorax | 36 (1%) | 55 (1%) | 91 (1%) | 0.66 |
| Skull | 14 (<1%) | 21 (<1%) | 35 (<1%) | 0.68 |
| Cervical | 4 (<1%) | 8 (<1%) | 12 (<1%) | 0.53 |
| Total | 5226 (100%) | 5233 (100%) | 10459 (100%) |
Table 1: Frequency of fractured regions by sex.
| Forearm | Hand | Shoulder | Ankle | Femur | Foot/toe | Pelvis | Thorax | Skull | Cervical | |
| Forearm | 2224 | 127 | 107 | 32 | 27 | 12 | 9 | 2 | 3 | 0 |
| Forearm | -24% | -1% | -1% | (<1%) | (<1%) | (<1%) | (<1%) | (<1%) | (<1%) | 0 |
| Hand | 1725 | 22 | 10 | 432 | 17 | 0 | 2 | 0 | 0 | |
| Hand | -19% | (<1%) | (<1%) | -5% | (<1%) | 0 | (<1%) | 0 | 0 | |
| Shoulder | 1451 | 19 | 19 | 6 | 23 | 6 | 2 | 0 | ||
| Shoulder | -16% | (<1%) | (<1%) | (<1%) | (<1%) | (<1%) | (<1%) | 0 | ||
| Ankle | 1328 | 29 | 41 | 1 | 0 | 1 | 0 | |||
| Ankle | -14% | (<1%) | (<1%) | (<1%) | 0 | (<1%) | 0 | |||
| Femur | 673 | 4 | 4 | 2 | 0 | 0 | ||||
| Femur | -7% | (<1%) | (<1%) | (<1%) | 0 | 0 | ||||
| Foot toe | 0 | 2 | 0 | 0 | ||||||
| Foot toe | 0 | 2 | 0 | 0 | -7% | |||||
| Pelvis | 121 | 2 | 0 | 0 | ||||||
| Pelvis | -1% | (<1%) | 0 | 0 | ||||||
| Thorax | 71 | 0 | 1 | 0 | ||||||
| Thorax | 71 | 0 | 1 | 0 | (<1%) | |||||
| Skull | 27 | 0 | ||||||||
| Skull | (<1%) | 0 | ||||||||
| Cervical | 11 | |||||||||
| Cervical | (<1%) |
Table 2: Distribution of fractures across different body sites.
Table 2: Distribution of fractures across different body sites. The main diagonal represents the count and percentage of unique Table 2: Distribution of fractures across different body sites. The main diagonal represents the count and percentage of unique fractures for each body site (e.g., forearm, hand, etc.). The off-diagonal cells in the upper right triangular portion represent the concordance between fractures at different body sites. The table does not include individuals with three or more concurrent fractures.
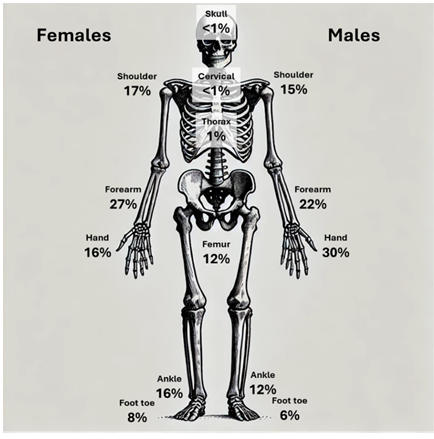
Figure 1: Distribution of fractures across different body regions by sex. Female Data: The frequencies of fractures as percentages are shown on the left side of the skeleton. Male Data: The frequencies of fractures as percentages are shown on the right side of the skeleton. Frequencies in the middle indicate no significant differences between sexes.
Discussion
Sex-Specific Patterns in Fractures
Females are more likely to have fractures in the forearm, shoulder, and ankle than males, but males experience more fractures in the hand/wrist. Current literature states that forearm fractures, shoulder, ankle are more prevalent in females, but hand/wrist fractures are more common in males which agrees with our study results [30]. Increased rates of osteoporosis in females may be a contributing factor to increase in fractures in these regions as the ankle is a weight-bearing region and the forearm and shoulder being used to brace against falls because fragility fractures when falling on an outstretched arm is common in individuals with osteoporosis. Furthermore, the highest incidence of ankle fractures in the male population is between 15 to 24 years of age, while in the female population it is between 75 and 84 years of age [22], This further indicates osteoporosis may play a crucial role in ankle fractures in females. Regarding the hand/wrist, the increased fracture rate in males compared to females might be due to occupational or recreational activities that involve more manual labor or physical impact such as working in construction or getting into physical altercations [15, 16].
Moving to the skull, cervical and thoracic vertebrae, we did not see enough fractures to make any conclusion besides the fact that they were rare in our study population. However, current literature states that skull and cervical fractures are more common in males whereas thoracic fractures are typically equal among males and females [31, 32, 33]. An increased sample size in future studies would help us distinguish if the RGV population follows these trends.
Femur fractures occur at similar frequencies in males and females in our study. Current literature states that femur fractures are more common in females, most likely due to osteoporosis in older aged women, which does not agree with our results [30], This could be because of the low SES, lack of documentation and health insurance of Hispanic individuals in the RGV causing the number of diagnoses to decrease [26, 27, 29, 34, 35]. This would have a greater effect on females, if they had more femur fractures than males, because an increased number of diagnoses in females would be more susceptible to changes to the population. However, the rate of osteoporosis in the RGV is higher which does not coincide with the decreased femur fractures in females in this population [36]. Further studies can focus on femur fractures in this underserved population and evaluate various demographics and other factors that could play a role in protection against femur fractures in females.
Foot/toe fractures occur at similar frequencies in males and females in our study, though females show a slightly higher frequency. Literature also shows that although fractures of certain bones may slightly vary between sexes in the foot and toe, the overall frequency of fracture is relatively similar [30], The differences in fractures between different bones of the foot and toe could be due to various factors including anatomical dissimilarities (body and bone size) and the effect of osteoporosis. Further studies may be conducted and focus on specific bones of the foot and toe to further evaluate fractures of these regions in the RGV population.
Distribution by Age
Our data suggests that age and sex differences in fracture occurrence are significant. Females have a bimodal distribution across a lifetime, one sharp peak in childhood (around 0-15 years) and one broader peak in older age (around 55-75 years). Male fractures are more evenly distributed across a lifetime with a sharp peak in childhood (0-15 years) and then a stable rate for the rest of their life with a much smaller number of fractures in older age groups compared to females. Females exhibit a significant increase in fractures at older ages (postmenopausal), likely linked to higher rates of osteoporosis in females compared to males [37]. Our results show that both sexes display a peak in fractures during early childhood (around 0–15 years), though the peak for males appears slightly more prominent. Current literature agrees with our results as it states that although both boys and girls experience an increase in fractures as children, boys typically have a greater increase in fractures compared to girls [38].
Co-occurrence of Fractures
Most fractures were unique to one site, with significant percentages for the forearm, hand, shoulder, and ankle. Other sites, such as the femur and foot/toe, had lower frequencies, while sites like the pelvis, thorax, skull, and cervical were much less common overall. The most frequent co-occurrences were in the hand and femur, followed by the forearm and hand. These co-occurrences often involved the forearm, hand, or femur, which suggests a potential biomechanical or injury-related relationship between these regions. High impact trauma such as car accidents or fragility fractures from fall such as in individuals with osteoporosis are possible injury mechanisms that could be the cause of co-occurring fractures. Future studies may focus on mechanisms of injury and fracture co-occurrence to determine the connection between fractures in different regions of the body.
Limitations and Future Studies
This study has its limitations. Data was collected solely from UTRGV UTHealth electronic databases, therefore, individuals who sought care at an institution not affiliated with UTRGV were not considered in this study. Due to this, our study may not be completely generalized to the South Texas population. Most of the patients analyzed in this study were Hispanic, which shows that our results may not be comparable to the United States as a whole or another nation’s general population whose ethnicity landscape differs from the one in our study. The RGV is a poverty stricken, medically underserved area with a substantial population of undocumented immigrants and individuals without health insurance [26, 27], This patient population is yet another reason the results of this study may not be universally applied. Fractures were analyzed by body region, not by specific bones or portions of bones. Although this may be good in terms of generalizability, it limits the use of the study when looking at fractures of very specific types or locations.
Future studies should focus on obtaining a larger study size, obtaining data from a more generalized population, and including more demographic factors that could play a role in the occurrence of fractures in various body regions to increase study validity and generalizability.
Conclusion
These findings suggest that individuals should be mindful and possibly take precautions to prevent fractures in particular body regions based on the age and sex of individuals. Physicians and other healthcare workers should also keep this information in mind when evaluating, informing, and treating patients, especially those with bone conditions or those at higher risk of bone injury.
Acknowledgements
We would like to sincerely acknowledge the assistance of Gumara Almanza, Jamie Diaz, and Manases Cepeda in data collection.
References
-
Whiteing NL (2008) Fractures: pathophysiology, treatment and nursing care. Nurs Stand 23(2): 49-57.
-
(2022) Bone Fractures. Cleveland Clinic.
-
Gómez Roselló E, Quiles Granado AM, Artajona Garcia M, Juanpere Martí S, Laguillo Sala G, et al. (2020) Facial fractures: classification and highlights for a useful report. Insights Imaging 11(1): 49.
-
(2023) Cleveland Clinic. Skull Fractures: Types, Treatment and Prevention. Cleveland Clinic.
-
McMordie JH, Viswanathan VK, Gillis CC (2024) Cervical Spine Fractures Overview. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
Kuo K, Kim AM (2024) Rib Fracture. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
Bentley TP, Ponnarasu S, Journey JD (2024) Sternal Fractures. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
Fernández-de Thomas RJ, De Jesus O (2024) Thoracolumbar Spine Fracture. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
Davis DD, Tiwari V, Kane SM, Kane SM, Waseem M (2024) Pelvic Fracture. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
Pencle F, Varacallo M (2024) Proximal Humerus Fracture. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
Bounds EJ, Frane N, Jajou L, Weishuhn LJ, Kok SJ (2024) Humeral Shaft Fractures. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
Crean TE, Nallamothu SV (2024) Distal Humerus Fractures. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
Rafi BM, Tiwari V (2024) Forearm Fractures. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
Boeddrich O, Sander AL, Lustenberger T, Marzi I, Frank J, et al. (2023) Epidemiology of carpal fractures: is it only about the scaphoid?. Eur J Trauma Emerg Surg 49(3): 1499-1503.
-
Werntz RL, Varacallo M (2024) Metacarpal Fracture. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
McDaniel DJ, Rehman UH (2024) Phalanx Fractures of the Hand. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
Kazley J, Bagchi K (2024) Femoral Neck Fractures. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
Denisiuk M, Afsari A (2024) Femoral Shaft Fractures. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
Coon MS, Best BJ (2024) Distal Femur Fractures. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
Thompson JH, Koutsogiannis P, Jahangir A (2024) Tibia Fractures Overview. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
Walters BB, Constant D, Anand P (2024) Fibula Fractures. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
Hermena S, Slane VH (2024) Ankle Fractures. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
(2024) Musculoskeletal Medicine for Medical Students. Calcaneal fractures.
-
(2016) Toe and Forefoot Fractures. OrthoInfo - AAOS.
-
Agrawal U, Tiwari V (2024) Metatarsal Fractures. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
Kuruvilla R, Raghavan R (2014) Health care for undocumented immigrants in Texas: past, present, and future. Tex Med 110(7): e1.
-
Ramirez AG, Thompson IM, Vela L (2013) The South Texas Health Status Review: A Health Disparities Roadmap. Cham (CH): Springer.
-
(2025) Get out and go running: UTRGV’s South Texas Diabetes and Obesity Institute working to bring attention to diabetes.
-
Valdez LA, Jaeger EC, Garcia DO, Griffith DM (2023) Breaking Down Machismo: Shifting Definitions and Embodiments of Latino Manhood in Middle-Aged Latino Men. Am J Mens Health 17(5): 15579883231195118.
-
Bergh C, Wennergren D, Möller M, Brisby H (2020) Fracture incidence in adults in relation to age and gender: A study of 27,169 fractures in the Swedish Fracture Register in a well-defined catchment area. In: Blank RD (Ed.), Plos One 15(12): e0244291.
-
Alter SM, Gonzalez MR, Solano JJ, Clayton LM, Hughes PG (2023) Comparing rates of skull fractures in female versus male geriatric patients who sustain head injuries. The American Journal of Emergency Medicine 65: 168-171.
-
Fredø HL, Rizvi SAM, Lied B, Rønning P, Helseth E (2012) The epidemiology of traumatic cervical spine fractures: a prospective population study from Norway. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 20(1): 85.
-
Kuharski MJ, Balmaceno-Criss M, Mansour A, Nadella A, Meininger K, et al. (2024) The Epidemiology of Recreation-Related Cervical and Thoracic Fractures. The Spine Journal 25(1): 136-144.
-
(2017) Ethnic and racial minorities & socioeconomic status. American Psychological Association.
-
Amenta AJB, Smith RA (2016) Hispanic/Latino Socioeconomic Status and Class.
-
Bialaszewski RP, Gaddis JM, Martin B, Dentino P, Ronnau J (2023) Bridging Bone Health: Osteoporosis Disparities in the Rio Grande Valley. Cureus 15(12): e51115.
-
Keen MU, Reddivari AKR (2024) Osteoporosis in Females. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
Valerio G, Gallè F, Mancusi C, Di Onofrio V, Colapietro M, et al. (2010) Pattern of fractures across pediatric age groups: analysis of individual and lifestyle factors. BMC Public Health 10: 656.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results