Bone and Joint Infections: A Retrospective Chart Review of the Medically Underserved Rio Grande Valley
Background: The Rio Grande Valley (RGV) is a demographically unique region. The goal of this study was to expand the knowledge of orthopedics in the RGV and analyze disparities between individuals with osteomyelitis, septic arthritis, and periprosthetic joint infections. Methods: This was a retrospective chart review using the University of Texas Rio Grande Valley UTHealth electronic database from January 1, 2017, to January 1, 2024. We used ICD-10 codes to collect medical charts of individuals with osteomyelitis, septic arthritis, and periprosthetic joint infections. Bivariate analyses and binary logistic regression models were used to analyze the data. Results: Females were significantly less likely to have an infection (AOR=0.16, p
Martin BC¹*, Peiris M² and Sander MD¹
¹University of Texas Rio Grande Valley School of Medicine, Edinburg, Texas 78539, United States ²University of Texas Rio Grande Valley, Department of Mathematics and Statistics, Edinburg, Texas 78539, United States Keywords: Bone Infection; Joint Infection; Orthopedic Infection; Underserved
Abbreviations
RA: Rheumatoid Arthritis; RGV: Rio Grande Valley; UTRGV: University of Texas Rio Grande Valley.
Introduction
Osteomyelitis
Simply put, osteomyelitis is a bone infection [1]. It is an old disease that is an acute or chronic inflammatory Investigation Paper process involving the bone and its structures, secondary to infection [1], The infection is due to pyogenic organisms such as bacteria, fungi, and mycobacteria [1], The overall osteomyelitis incidence in the United States is largely unknown, however, it is approximated to be as high as 1 in 675 United States hospital admissions each year, adding up to around 50,000 cases annually [1], Other literature shows an overall incidence of osteomyelitis of 21.8 cases per 100,000 person-years [1, 2]. Men and individuals of increased age had a higher incidence [1], It is unknown why males had increased incidence, but increased age is mainly due to an increase in comorbid factors such as diabetes mellitus and peripheral vascular disease as individuals age [1].
Septic Arthritis
Septic arthritis is joint inflammation secondary to a bacterial (most common), fungal, mycobacterial, viral, or other uncommon infectious pathogens [3]. The lack of a limiting membrane in the highly vascularized joint synovium makes it prone to infection via hematogenous seeding from systemic infection [3], It is generally monoarticular involving one large joint such as the hip or knee, although polyarticular septic arthritis may also occur [3], Uncommon as it may be, septic arthritis is an orthopedic emergency that may lead to significant joint damage and increased morbidity and mortality [3], The incidence of septic arthritis varies based on various risk factors but is between 2 to 6 cases per 100,000 people [3], It is more common in children than in adults with the incidence peaking between the ages of 2 and 3 years of age and has a male predominance [3], Risk factors in children include being a neonate, immunocompromised, hemophiliacs with hemarthroses, and those undergoing chemotherapy treatment [3], In adults, being older than 80 years of age, having diabetes mellitus, rheumatoid arthritis, osteoarthritis, recent joint surgery, joint prosthesis, skin infections, previous intra-articular injection, Human immunodeficiency virus, and sexual activity are some of the risk factors for septic arthritis [3].
Prosthetic and Periprosthetic Joint Infections
Prosthetic and Periprosthetic joint infections are unique, largely different from infections involving native bones or joints [4]. There is no universally accepted exact definition of prosthetic joint infection as the clinical symptoms vary, although classical features of infection, such as fever, leukocytosis, and signs of sepsis, are often absent [4], Only a small microbial burden is needed to cause a prosthetic joint infection as microorganisms can adhere to the surfaces of artificial components and form biofilms [4], These biofilms exhibit a strong resistance to numerous antimicrobial agents and are proficient at evading the innate immune system [4], These infections pose a significant clinical problem as they greatly increase morbidity and mortality [4], With the number of hip and knee arthroplasties increasing over the past couple of decades and projected to continue this trend, there has been a parallel escalation in the incidence of prosthetic joint infection that is also expected to rise [4], Also, although the risk of developing prosthetic joint infection is most pronounced in the early postoperative period, prosthetic joint infection is a persistent risk extending throughout the lifespan of the prosthesis as a large number of prosthetic joint infections become clinically apparent after the first postoperative year [4], There are numerous risk factors for developing a prosthetic joint infection that fall into various risk categories including preoperative, modifiable, nonmodifiable, surgery- related, and postoperative factors [4], Some of these risk factors include morbid obesity, malnutrition, hyperglycemia, uncontrolled diabetes mellitus, rheumatoid arthritis (RA), preoperative anemia, cardiovascular disorders, chronic renal failure, smoking, alcohol abuse and depression [5].
Study Significance and Aim
The Rio Grande Valley (RGV) is a demographically unique region that is impoverished, medically underserved, and contains a large number of undocumented immigrants [6, 7]. It also has a high prevalence of chronic conditions including obesity and diabetes [8]. The machismo construct is another factor that plays a role in the health of this region as it may prevent Hispanic males from seeking medical care [9]. These factors warrant investigation of various health issues in the RGV. To our knowledge, no study has analyzed these bone and joint infections in this medically underserved community. The goal of this study was to expand the knowledge of orthopedics in the Rio Grande Valley and analyze individuals with osteomyelitis, septic arthritis, and periprosthetic joint infections to determine which infectious bone or joint conditions are most prevalent and determine if there were any demographic disparities between the various types of bone and joint infections. We hypothesized that age and BMI would be significant factors affecting bone and joint infections, specifically older age and higher BMI increasing risk for infection.
Material and Methods
Study Design and Data Collection
This was a retrospective chart review and IRB approval was obtained prior to starting this study. Data was gathered from the University of Texas Rio Grande Valley (UTRGV) UTHealth electronic database. Data collection included medical charts from January 1, 2017, to January 1, 2024. We collected and analyzed medical charts of individuals who were diagnosed with osteomyelitis, septic arthritis, and periprosthetic joint infections. The bone and joint infections were obtained by using ICD-10 diagnosis codes. The codes were as follows (ICD-10 codes): osteomyelitis (M86), septic arthritis (M00), periprosthetic joint infection (T84.5 or T84.7). For each patient, various demographics were collected, including age at diagnosis, sex, BMI, race/ethnicity, and marital status.
Inclusion and Exclusion Criteria
Individuals of all ages were included in this study in order to represent the entire spectrum of the population. Individuals over the age of 85 were included as a group indicated as >85 years of age. Individuals who were not seen by a UTRGV associated institution were not included in the study. If there were duplications of an individual’s medical chart, such as an individual having more than one appointment, the earliest date, the date the patient was diagnosed with any of the analyzed bone disorders, was included. If an individual was diagnosed with more than one of the bone or joint infections analyzed, all infections were included and analyzed based on the date of diagnosis and demographics of the patient at the point in time of that specific diagnosis.
Statistical Analysis
Bivariate analyses were performed to assess the associations between each predictor variable and the outcome of any bone and joint infection type (osteomyelitis, septic arthritis, prosthetic joint infection). For categorical variables (e.g., ethnicity, sex, marital status, BMI category, and Race), we used Chi-square tests with Yates’ correction to evaluate statistical independence with joint involvement. Fisher’s exact test was used when expected cell counts
Results
Demographics (Table 1)
were less than five to ensure accurate p-value estimation. For continuous variables (e.g., age at DOS), we assessed differences between groups using a two independent sample test.
To identify factors associated with any type of bone and joint infection (out of any three bone and joint infection types) and healthy controls (individuals without bone or joint infection), we performed a binary logistic regression analysis. The binary logistic regression model included having any type of bone and joint infection as the dependent variable and the demographics as predictors. The logistic regression model was used to estimate the log odds of having any type of bone and joint infection, producing coefficients (log odds) for each predictor. Results were reported as odds ratios with 95% confidence intervals. Statistical significance was defined at the 0.05 level.
All analyses were performed with R statistical software (Version: 4.2.2 R Core Team, 2022).
| N=4984 (100 %) | |
|---|---|
| Gender | |
| ■ Male | 2246 (45.0 %) |
| ■ Female | 2738 (55.0 %) |
| BMI | |
| ■ Underweight | 149 (3.0 %) |
| ■ Normal | 311 (6.2 %) |
| ■ Overweight | 570 (11.4 %) |
| ■ Obese | 1093(22.0 %) |
| ■ NA | 2861 (57.4 %) |
| Ethnicity | |
| ■ Hispanic or Latino | 3712 (83.8%) |
| ■ Not Hispanic or Latino | 514 (8.4%) |
| ■ Patient Declined | 758 (7.8%) |
| Race | |
| ■ White | 4071 (74.5 %) |
| ■ Other (including Black African Americans) | 210 (10.3 %) |
| ■ Patient Declined | 703 (15.2 %) |
| Marital status | |
| ■ Single | 1444 (30.0 %) |
| ■ Married | 1782 (35.7 %) |
| ■ Other | 507 (10.2 %) |
| ■ Patient Declined | 1758 (25.1 %) |
| Type | |
| ■ Osteomyelitis | 959 (19.2 %) |
| ■ Prosthetic Joint Infection | 76 (1.5 %) |
| ■ Septic Arthritis | 232 (4.7 %) |
| ■ Healthy | 3717 (74.6 %) |
Table 1: Patient demographics.
The dataset highlights key demographic and clinical characteristics of individuals with bone and joint infections, as well as those without such conditions. Males represent 45.0% of the population, while females make up 55.0%. The BMI distribution shows a high percentage of individuals with missing BMI data (57.4%), followed by 22.0% classified as Obese and 11.4% as Overweight, reflecting potential challenges in weight-related health management. Most participants are Hispanic or Latino (83.8%), with White individuals comprising 74.5% of the population, and 35.7%
Osteomyelitis (Figures 1-3)
are married. Notably, 25.1% of marital statuses were declined to be reported.
Clinically, the most common condition observed is osteomyelitis (19.2%), followed by septic arthritis (4.7%), and prosthetic joint infection (1.5%). A significant majority (74.6%) are classified as healthy (individuals without bone or joint infection), indicating that a smaller subset of the population had active bone or joint infections.
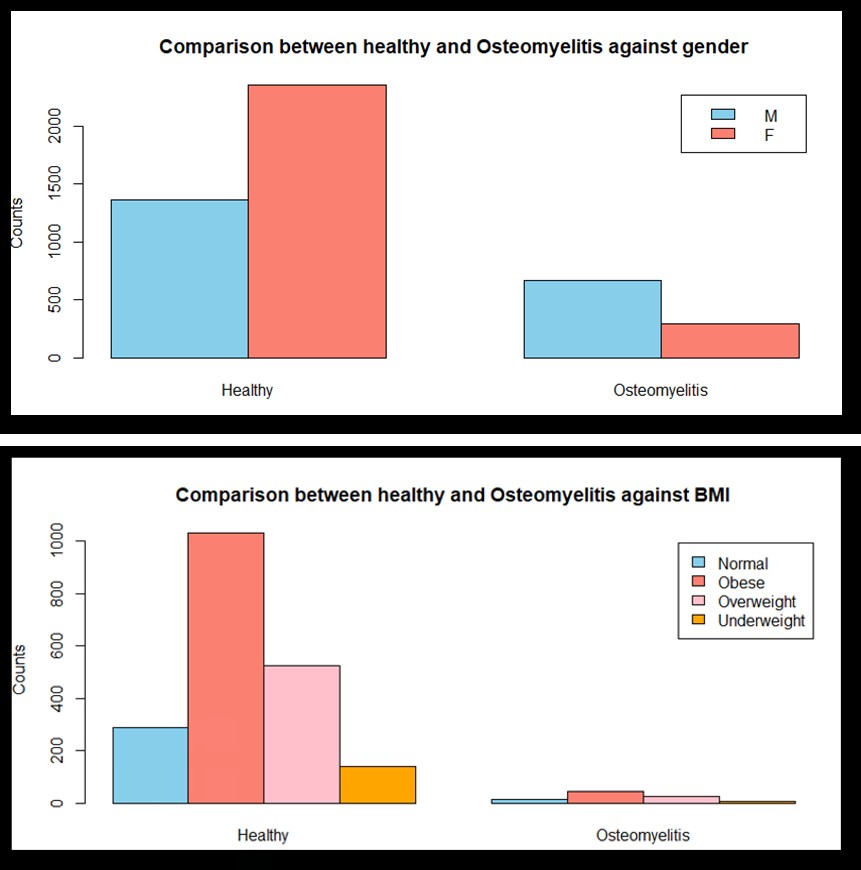
Figure 1A: Comparison between healthy and osteomyelitis individuals against Gender. Healthy M: 1365, Healthy F: 2352, Osteomyelitis M: 664, Osteomyelitis F: 295.
Figure 1B: Comparison between healthy and osteomyelitis individuals against BMI. Healthy Normal: 288, Healthy Obese: 1031, Healthy Overweight: 527, Healthy Underweight: 141, Osteomyelitis Normal: 13, Osteomyelitis Obese: 44, Osteomyelitis Overweight: 27, Osteomyelitis Underweight: 6.
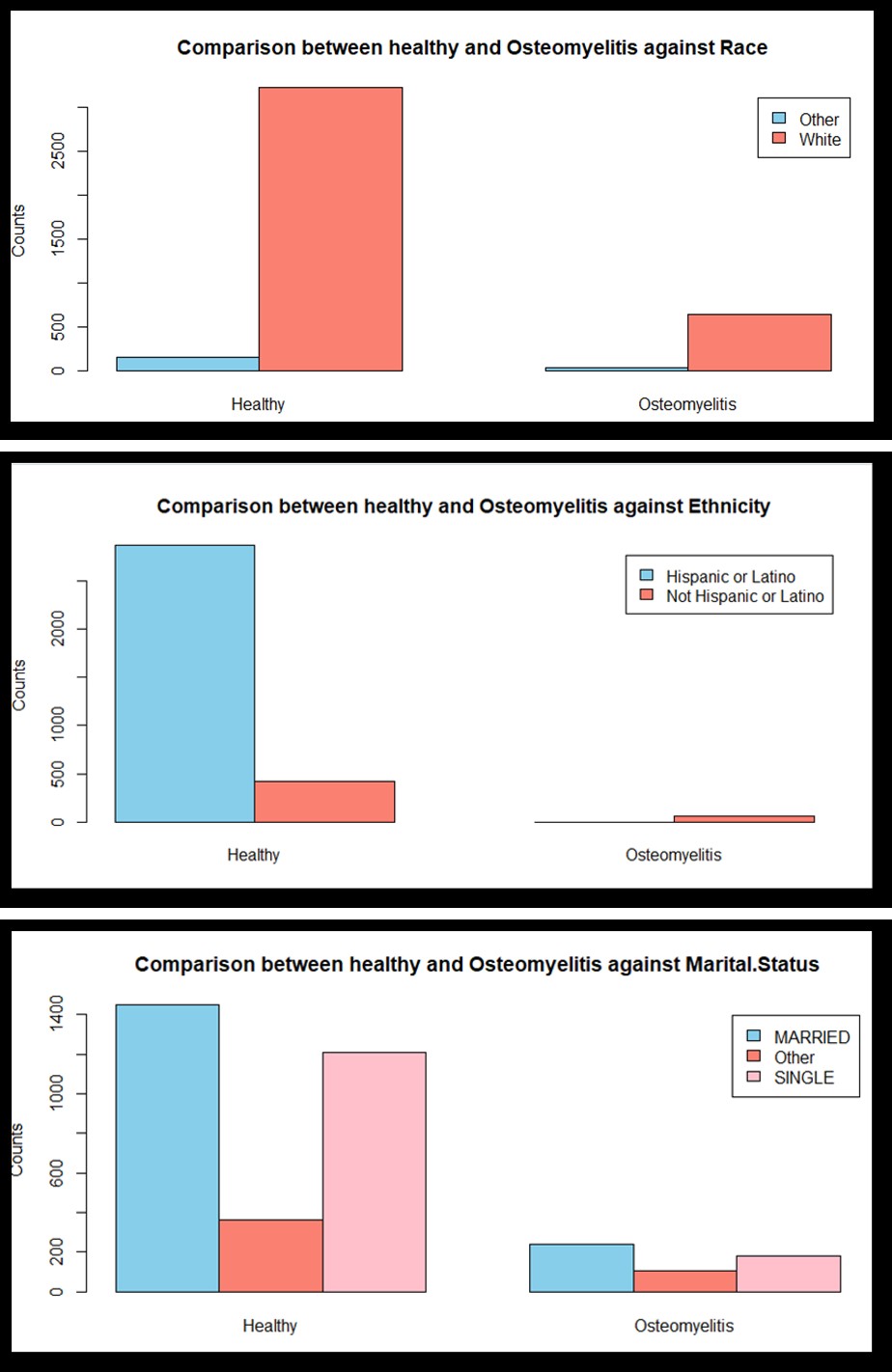
Figure 1C: Comparison between healthy and osteomyelitis individuals against Race. Healthy Other: 159, Healthy White: 3223, Osteomyelitis Other: 36, Osteomyelitis White: 639.
Figure 1D: Comparison between healthy and osteomyelitis individuals against Ethnicity. Healthy Hispanic/Latino: 2865, Healthy Not Hispanic/Latino: 419, Osteomyelitis Hispanic/Latino: 0, Osteomyelitis Not Hispanic/Latino: 59.
Figure 1E: Comparison between healthy and osteomyelitis individuals against Marital Status. Healthy Married: 1448, Healthy Other: 363, Healthy Single: 1207, Osteomyelitis Married: 239, Osteomyelitis Other: 107, Osteomyelitis Single: 182.
Septic Arthritis
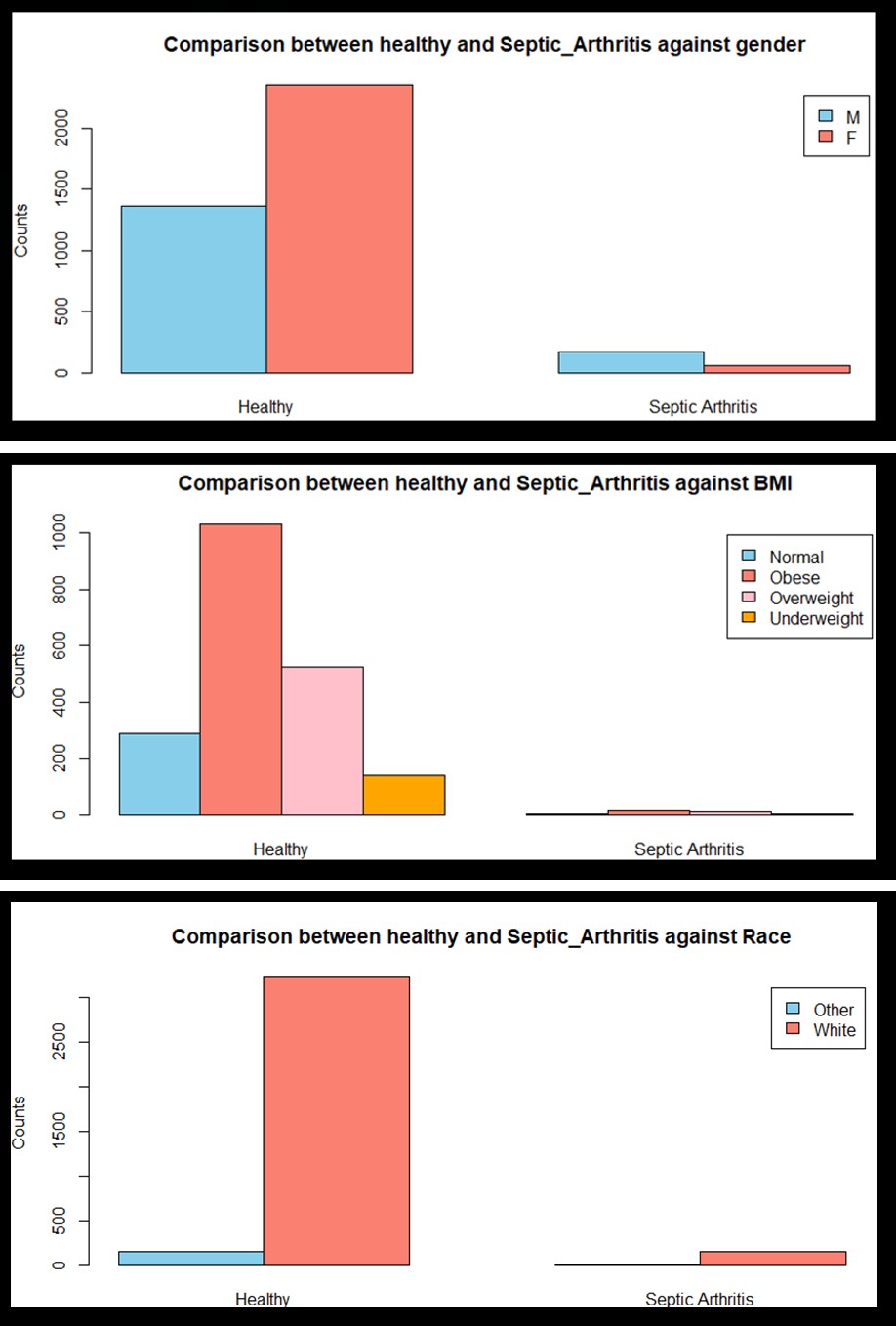
Figure 2A: Comparison between healthy and septic arthritis individuals against Gender. Healthy M: 1365, Healthy F: 2352, Septic Arthritis M: 176, Septic Arthritis M: 56.
Figure 2B: Comparison between healthy and septic arthritis individuals against BMI. Healthy Normal: 288, Healthy Obese: 1031, Healthy Overweight: 527, Healthy Underweight: 141, Septic Arthritis Normal: 5, Septic Arthritis Obese: 13, Septic Arthritis Overweight: 11, Septic Arthritis Underweight: 2.
Figure 2C: Comparison between healthy and septic arthritis individuals against Race. Healthy Other: 159, Healthy White: 3223, Septic Arthritis Other: 11, Septic Arthritis White: 154.
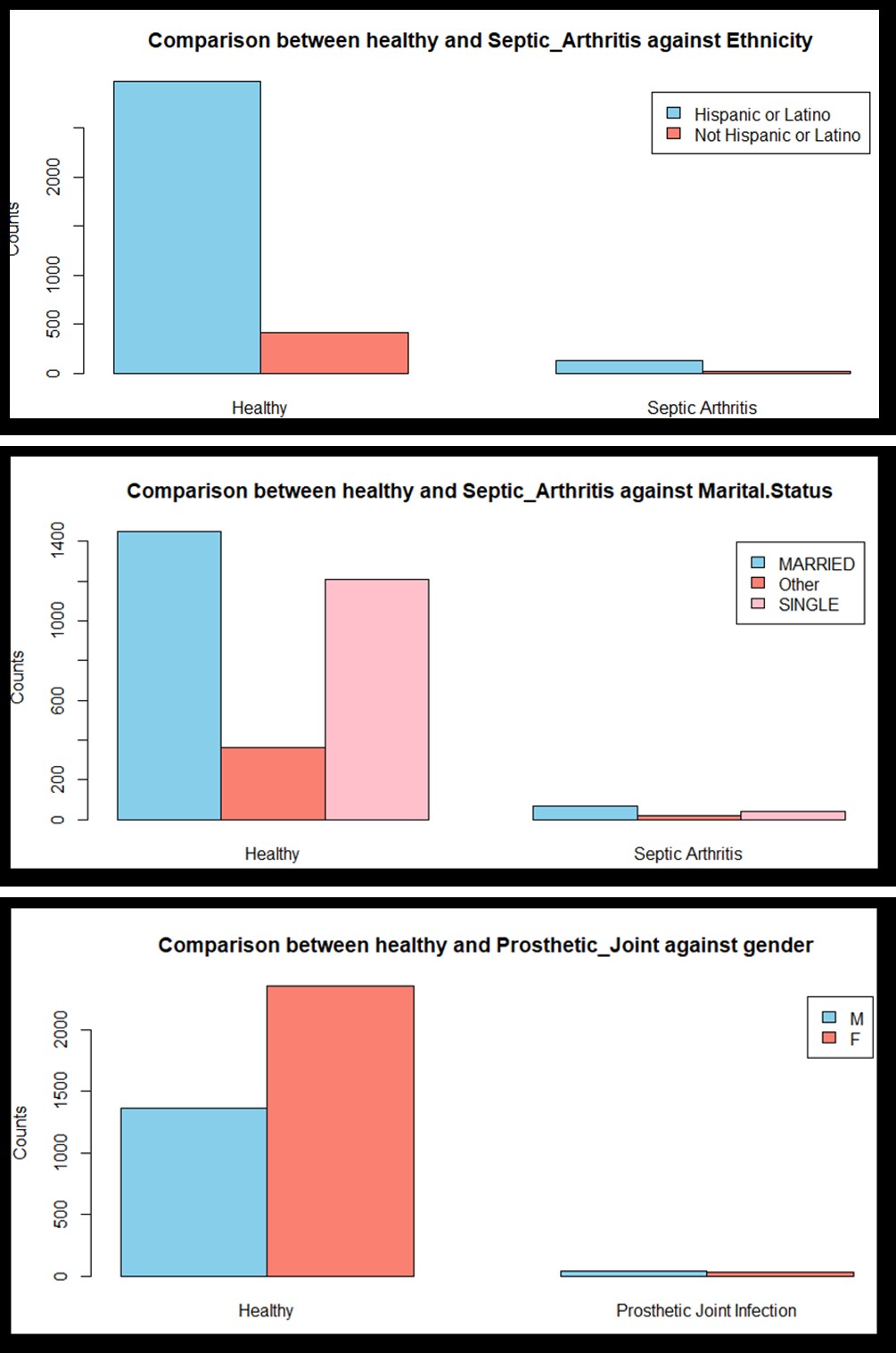
Figure 2D: Comparison between healthy and septic arthritis individuals against Ethnicity. Healthy Hispanic/Latino: 2974, Healthy Not Hispanic/Latino: 419, Septic Arthritis Hispanic/Latino: 126, Septic Arthritis Not Hispanic/Latino: 23.
Figure 2E: Comparison between healthy and septic arthritis individuals against Marital Status. Healthy Married: 1448, Healthy Other: 363, Healthy Single: 1207, Septic Arthritis Married: 67, Septic Arthritis Other: 21, Septic Arthritis Single: 44.
Prosthetic Joint Infection
Figure 3A: Comparison between healthy and prosthetic joint infection individuals against Gender. Healthy M: 1365, Healthy F: 2352, Prosthetic joint infection M: 41, Prosthetic joint infection F: 35.
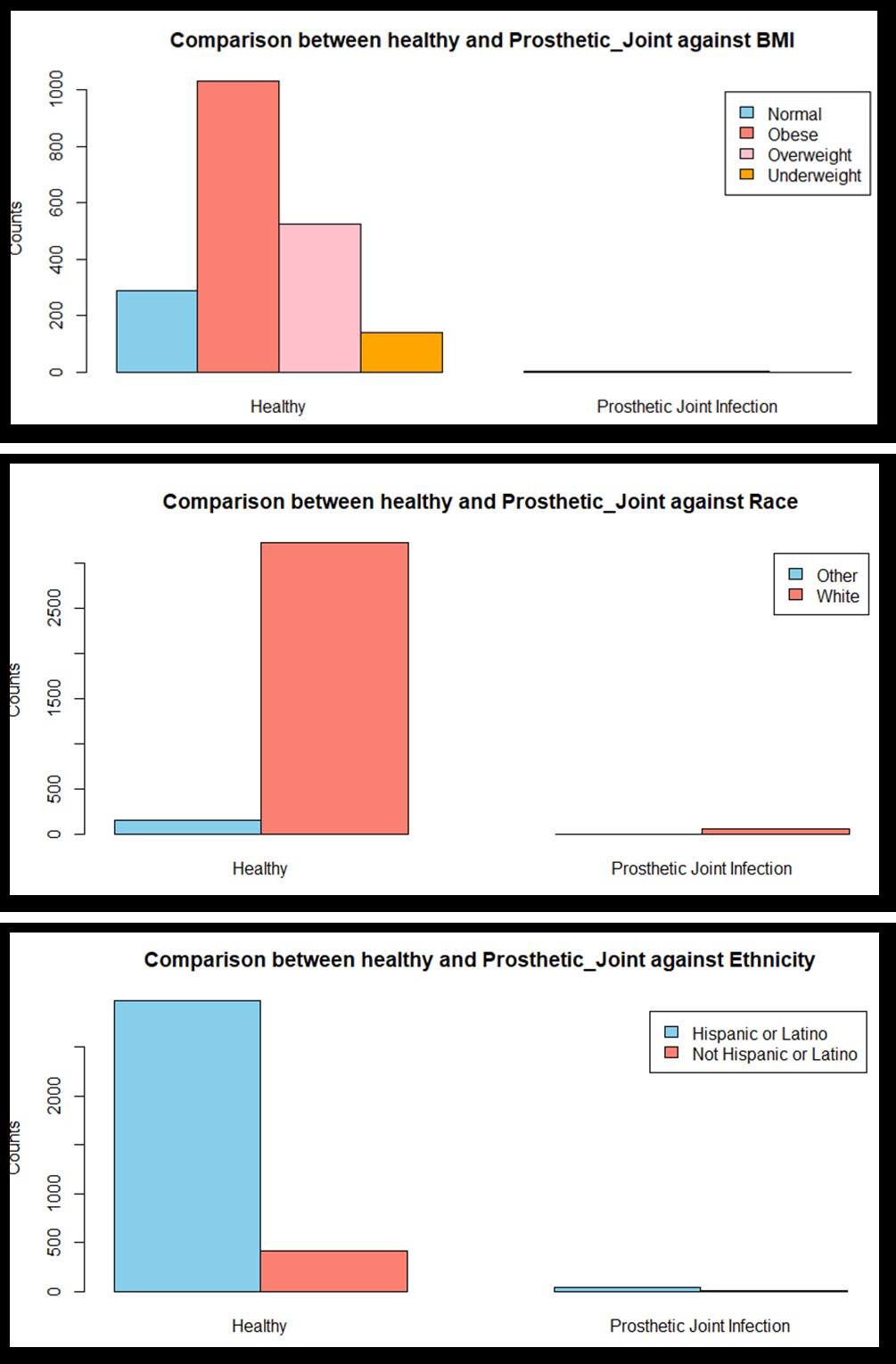
Figure 3B: Comparison between healthy and prosthetic joint infection individuals against BMI. Healthy Normal: 288, Healthy Obese: 1031, Healthy Overweight: 527, Healthy Underweight: 141, Prosthetic joint infection Normal: 5, Prosthetic joint infection Obese: 5, Prosthetic joint infection Overweight: 5, Prosthetic joint infection Underweight: 0.
Figure 3C: Comparison between healthy and prosthetic joint infection individuals against Race. Healthy Other: 159, Healthy White: 3223, Prosthetic joint infection Other: 4, Prosthetic joint infection White: 55.
Figure 3D: Comparison between healthy and prosthetic joint infection individuals against Ethnicity. Healthy Hispanic/Latino: 2974, Healthy Not Hispanic/Latino: 419, Prosthetic joint infection Hispanic/Latino: 44, Prosthetic joint infection Not Hispanic/ Latino: 13.
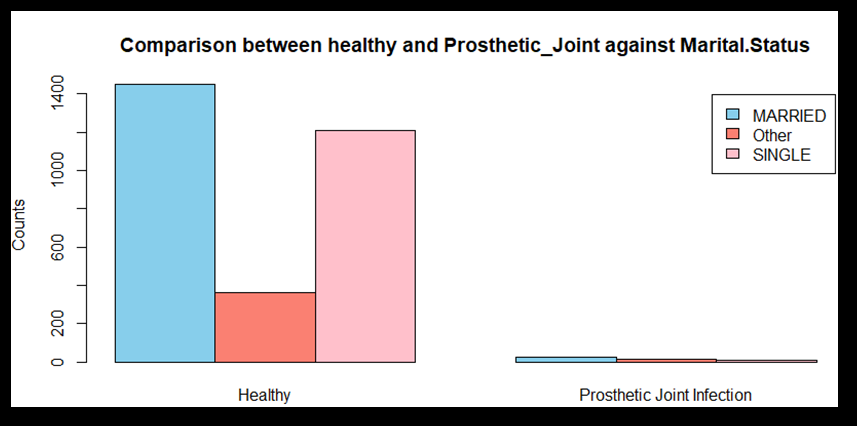
Figure 3E: Comparison between healthy and prosthetic joint infection individuals against Marital Status. Healthy Married: 1448, Healthy Other: 363, Healthy Single: 1207, Prosthetic joint infection Married: 28, Prosthetic joint infection Other: 16, Prosthetic joint infection Single: 11.
Bivariate Analysis (Table 2)
| Osteomyelitis | Septic Arthritis | Prosthetic Joint Infection | |||||
|---|---|---|---|---|---|---|---|
| Odds Ratio (95% CI) | p-value | Odds Ratio (95% CI) | p-value | Odds Ratio (95% CI) | p-value | ||
| Gender | Male | Ref | <0.001 | Ref | <0.001 | Ref | 0.003 |
| Female | 0.258 | 0.185 | 0.495 | ||||
| (0.221,0.300) | (0.135, 0.250) | (0.312,0.782) | |||||
| BMI | Normal | Ref | 0.905 | Ref | 0.632* | Ref | 0.119* |
| Obese | 0.938 | 0.712 | 0.28 | ||||
| (0.511, 1.842) | (0.263,2.286) | (0.085, 0.925) | |||||
| Overweight | 1.128 | 1.182 | 0.548 | ||||
| (0.582, 2.300) | (0.419,3.872) | (0.166, 1.810) | |||||
| Underweight | 0.955 | 0.853 | 0.379 | ||||
| (0.324, 2.500) | (0.109,4.198) | (0.0145, 2.330) | |||||
| Race | Other | Ref | 0.547 | Ref | 0.333 | Ref | 0.360* |
| White | 0.872 | 0.682 | 0.655 | ||||
| (0.609, 1.284) | (0.378, 1.363) | (0.264, 2.227) | |||||
| Ethnicity | Not Hispanic or Latino | Ref | <0.001* | Ref | 0.322 | Ref | 0.03 |
| Hispanic or Latino | 0.003 | 1.303 | 0.473 | ||||
| (0.000, 0.012) | (0.805, 2.017) | (0.259,0.925) | |||||
| Marital Status | Single | Ref | <0.001 | Ref | 0.204 | Ref | <0.001 |
| Married | 1.094 | 1.267 | 2.102 | ||||
| (0.889, 1.348) | (0.862, 1.881) | (1.067. 4.453) | |||||
| Other | 1.955 | 1.593 | 4.809 | ||||
| (1.495, 2.548) | (0.916, 2.686) | (2.216,10.832) |
Table 2: Summary of Chi Square/ Fisher’s Exact Test results for assessing the relationship between the three types of bone and jo
Table 2: Summary of Chi Square/ Fisher’s Exact Test results for assessing the relationship between the three types of bone and joint infections vs Healthy (individuals without bone or joint infection) control variations and the Demographic variables. Note: 95% CI represents the 95% confidence interval for crude Odds Ratio. The p-values based on Fisher’s Exact tests are denoted by *.
Gender
- Osteomyelitis: Females had significantly lower odds (OR=0.258) compared to males (p<0.001).
- Septic Arthritis: Females had significantly lower odds (OR=0.185) compared to males (p<0.001).
- Prosthetic joint infection: Females had lower odds (OR=0.495) compared to males (p=0.003).
BMI
• Across different bone and joint infections, none of the BMI categories showed significant differences (all p-values are non-significant, p=0.905, p=0.632 and p=0.119).
Race
• No significant differences were observed across racial groups for all bone and joint infections (p=0.547, p=0.333, and p=0.360).
Ethnicity
• Osteomyelitis: Hispanic or Latino individuals had spectacularly lower odds (OR=0.003) compared to non- Hispanics (p<0.001). • Septic Arthritis: There was no significant association (p=0.322) • Prosthetic Joint Infection: Hispanic or Latino individuals had lower odds (OR=0.473) compared to non-Hispanics (p=0.030).
Marital Status
• Osteomyelitis: Significant associations were observed, with “Other” marital status showing the highest odds (OR=1.955, p<0.001) • Septic Arthritis: No significant associations (p=0.204). • Prosthetic joint infection: Significant higher odds were observed for “Married” (OR=2.102) and “Other” (OR=4.809, p<0.00).
Overall, being female was strongly protective against all three bone disorders. Hispanic or Latino individuals had significantly reduced odds of osteomyelitis and Prosthetic joint infections compared to non-Hispanics. Being married or in “Other” categories significantly increased the odds of Prosthetic joint infections, and “Other” marital status was also a risk factor for osteomyelitis.
Age at Diagnosis
The Kruskal-Wallis test, with a p-value<0.0001, showed that there are significant differences between age at diagnosis across the three bone and joint infection groups and healthy controls(individuals without bone or joint infection) (chi- squared = 194.9, degrees of freedom (df) = 3, p-value < 2.2e-16). Dunn’s Test with Bonferroni adjustment was used to evaluate multiple comparisons. There are significant differences in median age at diagnosis between most group pairs except Osteomyelitis vs. Septic Arthritis (p-value adjusted = 0.601). The strongest differences are between Healthy vs. Osteomyelitis (Z = -11.88, p-value adjusted = 8.87e-32) and Healthy vs. Prosthetic Joint Infection (Z = -7.38, p-value adjusted = 9.26e-13) as indicated by the large Z-values and extremely small p-values.
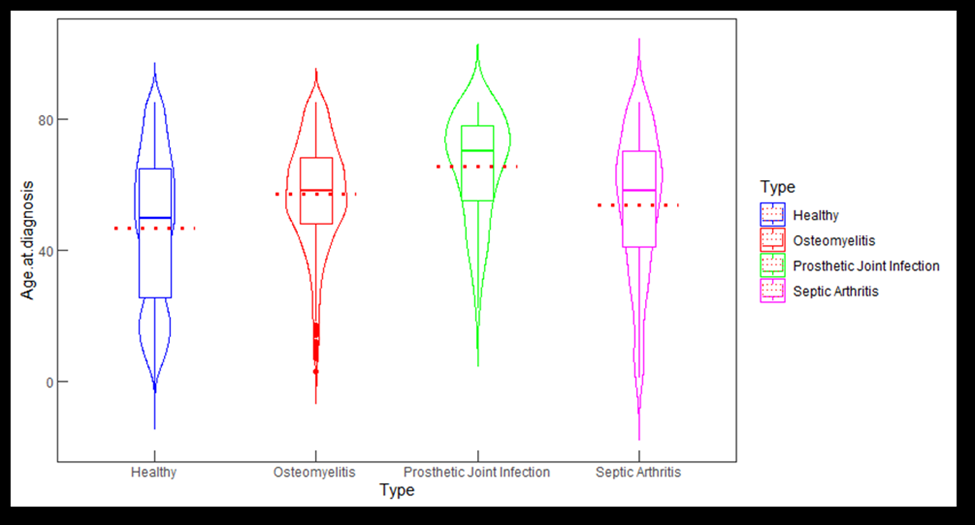
The violin plot (Figure 4) illustrates the distribution of age at diagnosis across four groups: Healthy (individuals without bone or joint infection), osteomyelitis, Prosthetic joint infection, and Septic Arthritis. Osteomyelitis and Septic Arthritis show lower median ages compared to Prosthetic joint infections, indicating these conditions were more common in younger individuals. These differences were supported by statistical tests (Kruskal-Wallis and Dunn’s Test) and suggest distinct age-related patterns in the diagnosis of bone and joint infections.
Binary Logistic Regression
The binary logistic regression model identified significant predictors of having a bone or joint infection compared to being healthy (individuals without bone or joint infection). Females were significantly less likely to have an infection than males (AOR=0.16, p<0.001), while married individuals also had reduced odds of infection (AOR=0.47, p=0.01) compared to single individuals. While bivariate analysis showed higher odds of bone or joint infection for married individuals, this association diminished in the multivariate logistic regression model. Obesity was associated with increased odds of infection (AOR=1.36, p=0.021), whereas overweight and underweight categories did not show significant differences. White individuals had significantly lower odds of infection compared to other races (AOR=0.44, p=0.028). Age at diagnosis slightly increased the odds of infection (AOR=1.02, p<0.001), indicating that older individuals were at a marginally higher risk. Ethnicity (Hispanic vs. non-Hispanic) and marital status categorized as “Other” did not significantly impact the odds. Overall, the model highlights the importance of demographic and health- related factors such as sex, BMI, and race in predicting the likelihood of a bone or joint infection.
Discussion
Our results showed that females are significantly less likely to have an infection than males, while married individuals also have reduced odds of infection compared to single individuals. Current literature states that men are more likely to get OM, SA, and PJI compared to females which agrees with our results [1, 3, 10]. However, according to our knowledge, there are no studies evaluating the effect of marital status on bone and joint infections to compare our results with. An explanation for our findings is that increased social support can boost the immune system as positive experiences of social connection have been shown to be a factor in reducing inflammation and bolstering antiviral responses [11]. Married individuals have more social support than the average individual as they have a constant companion, or more if they have children, to live life with. The Hispanic views on marriage and family may further explain this phenomenon as Hispanic couples tend to have more children and place a strong emphasis on family bonds, both of which can increase social support and therefore boost the immune system [12, 13].
Our study also showed that obesity is associated with increased odds of infection. Current studies indicate that the risk of PJI is increased in obese individuals [5], Current literature also states that obesity may increase the risk of developing SA because joint damage from any cause, such as osteoarthritis from obesity, has been shown to increase the risk of SA [14]. Our results agree with these previous findings regarding PJI and SA. However, BMI is not associated with increased risk of OM at any point in life according to current literature, although it may affect complication rates once an individual has OM [15]. This does not agree with our results. Various factors in our study population could help explain this. The RGV is a region with increased obesity rates compared to national average which would increase the number of OM individuals who are obese compared to OM individuals who are not. There is also a high prevalence of diabetes which tends to involve higher BMI individuals.
White individuals have significantly lower odds of infection compared to other races. To our knowledge, no studies have analyzed the effect of race on risk of osteomyelitis, only the effect of race on length of hospital stay in individuals with osteomyelitis. Regarding PJIs, Black individuals are at an increased risk of getting a PJI compared to white individuals which agrees with our study results [16]. An explanation for this is racial disparities in various factors such as reduced access to high-quality obesity management, smoking cessation resources, and high-quality diabetes care, all of which are factors that are known to increase the risk of PJI [16], Furthermore, non-white individuals in this region may be at increased risk of infection due to the machismo construct. Within this construct, traditional beliefs about masculinity and masculine identity are socially constructed and greatly influence behaviors and an individual’s perception of what they believe it means to be a man, especially in the Latino culture [9], As a result, male behavior is shaped by trying to explicitly avoid behaviors that are thought to be feminine, such as eating healthy, applying sunscreen, and possibly avoiding seeking help for mental health or other medical conditions [9], Delaying seeking medical advice or help may increase risks of infection in individuals who abide by this construct. Regarding septic arthritis, although we did not find any adult studies, one study on pediatric patients found that whites were more likely to have septic arthritis compared to other races [17]. This does not agree with our results. The anatomical and physiological differences between children and adults may play a role in this disagreement as these two populations differ in many ways [18]. The anatomical and physiological conditions unite to produce various, unique responses to injuries and healing that are absent in adults [18], Furthermore, there are many differences in physiological factors at play due to the presence of growth plates in children [18].
Age at diagnosis slightly increases the odds of infection, indicating that older individuals are at a marginally higher risk. Current literature states that there are no associations between age and risk of PJI [19]. However, it has been shown that older individuals have an increased risk of OM, agreeing with our results, but children are more at risk for SA compared to adults [1, 3], An explanation for this is that elderly individuals above the age of 80 years also have an increased risk of SA [3], This bimodal distribution of ages in the SA population would explain why the average age of diagnosis for SA in our population was focused on the older adult range, but only marginally. The high number of comorbidities in the RGV, our study population, could also increase the frequency of septic arthritis in adults in our population [3, 8]. This study has limitations. Most individuals analyzed in this study were Hispanic, indicating that the results may not be generalizable to Texas, United States, or other nations whose ethnicity landscape differs from the one in our study. Data for the study was collected solely from the UTRGV UTHealth electronic databases, so individuals who received care at an institution not affiliated with UTRGV were not considered in this study. Due to this, the results may not be generalizable to the entire South Texas Population. Also of note, the RGV is an impoverished, medically underserved area with a large population of undocumented immigrants and individuals without health insurance [6, 7], This patient community is another reason the results of this study may not be universally applied. Future studies should obtain data from a more generalizable source, obtain a larger sample size, and include more patient characteristics and comorbidities that may play a role in the development of these bone and joint infections to increase study validity and generalizability.
Conclusion
This study highlights the importance of demographic and health-related factors such as sex, age, BMI, and race in predicting the likelihood of a bone or joint infection. These patient demographics may be targeted as areas of focus when conducting further research on bone and joint infections to improve the overall orthopedic knowledge and care of individuals in this region in this region.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflicts of Interest
The authors declare no conflict of interest.
Author Contributions
BCM contributed to the conception and design of the work, acquisition, analysis and interpretation of the data, drafting and reviewing of the manuscript text. MP contributed to the design of the work, analysis and interpretation of data, and drafting of the manuscript. MS contributed to the interpretation of data, reviewing of the manuscript, and served as a mentor. All authors approved the final version to be published and agree to be responsible for all aspects of the work.
Data Sharing Statement
Data used is property of the University of Texas Rio Grande Valley and is not publicly accessible but may be made available upon request.
References
-
Momodu II, Savaliya V (2024) Osteomyelitis. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
Kremers HM, Nwojo ME, Ransom JE, Wood-Wentz CM, Melton LJ, et al. (2015) in the epidemiology of osteomyelitis: a population-based study, 1969 to 2009. J Bone Joint Surg Am. 97(10): 837-845.
-
Momodu II, Savaliya V (2024) Septic Arthritis. In: StatPearls [Internet], Treasure Island (FL), StatPearls Publishing.
-
Ayoade F, Li D, Mabrouk A, Todd JR (2024) Periprosthetic Joint Infection. In: StatPearls, Treasure Island (FL), StatPearls Publishing.
-
Eka A, Chen AF (2015) Patient-related medical risk factors for periprosthetic joint infection of the hip and knee. Ann Transl Med 3(16): 233.
-
Kuruvilla R, Raghavan R (2014) Health care for undocumented immigrants in Texas: past, present, and future. Tex Med 110(7): e1.
-
Ramirez AG, Thompson IM, Vela L (2013) The South Texas Health Status Review: A Health Disparities Roadmap. Springer Cham (H), Germany.
-
(2018) Get out and go running: UTRGV’s South Texas Diabetes and Obesity Institute working to bring attention to diabetes.
-
Valdez LA, Jaeger EC, Garcia DO, Griffith DM (2023) Breaking Down Machismo: Shifting Definitions and Embodiments of Latino Manhood in Middle-Aged Latino Men. Am J Mens Health 17(5): 15579883231195118.
-
De Mauro D, Meschini C, Balato G, Ascione T, Festa E, et al. (2024) Sex-related differences in periprosthetic joint infection research. J Bone Jt Infect 9(2): 137-142.
-
Leschak CJ, Eisenberger NI (2019) Two Distinct Immune Pathways Linking Social Relationships with Health: Inflammatory and Antiviral Processes. Psychosom Med 81(8): 711-719.
-
Hispanics and Latinos. Healthy Marriage and Responsible Fatherhood.
-
Canún N (2022) The Powerful Role of Family in Hispanic Culture [Unlike U.S. Culture].
-
Alexandersson H, Dehlin M, Jin T (2024) Increased Incidence and Clinical Features of Septic Arthritis in Patients Aged 80 Years and above: A Comparative Analysis with Younger Cohorts. Pathogens 13(10): 891.
-
Liu HZ, Liang J, Hu AX (2024) Type 2 diabetes mediates the causal relationship between obesity and osteomyelitis: A Mendelian randomization study. Medicine (Baltimore) 103(20): e38214.
-
Pinkney JA, Davis JB, Collins JE, Shebl FM, Jamison MP, et al. (2023) Racial Disparities in Periprosthetic Joint Infections after Primary Total Joint Arthroplasty: A Retrospective Study. Antibiotics (Basel) 12(11): 1629.
-
Tretiakov M, Cautela FS, Walker SE, Dekis JC, Beyer GA, et al. (2019) Septic arthritis of the hip and knee treated surgically in pediatric patients: Analysis of the Kids’ Inpatient Database. J Orthop 16(1): 97-100.
-
(2021) Themes UFO. Differences between Pediatric and Adult Musculoskeletal Systems [Internet]. Musculoskeletal Key.
-
Blom AW, Beswick AD, Burston A, Carroll FE, Garfield K, et al. (2022) Infection after total joint replacement of the hip and knee: research programme including the INFORM RCT. Programme Grants for Applied Research, Southampton, UK.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results