Epidemiology of Superficial Fungal Infections in Hospital Settings in Togo and Senegal from 2019 to 2020
Introduction
Superficial fungal diseases are cosmopolitan affections caused by yeast and filamentous microscopic fungi (dermatophytes and moulds). Their very high prevalence and worldwide distribution make them one of the most common dermatological diseases [1]. Nearly one billion people have skin fungal diseases, which makes this disease only slightly less common on the planet than headaches and dental caries [2]. They characterize several symptoms including skin, nail and hair disorders. These symptoms are very unpleasant because they not only modify the aesthetics of the affected persons but also create discomfort and therefore affect their quality of life. Laboratory diagnosis of superficial mycoses is based mainly on direct examination of the sample followed by culture.
The distribution of the dermatomycoses, their aetiological agents and the predominating anatomical infection patterns vary with geographical location and a wide range of environmental and cultural factors [3]. Currently, Trichophyton rubrum, Trichophyton interdigitale, Trichophyton tonsurans, Microsporum canis, Malassezia spp. and Candida spp. are the main fungal species identified in superficial mycoses [4, 5]. Recent studies, in Senegal, have reported predominance of Trichophyton soudanense (24,9%) and Trichophyton rubrum (13,7%) among dermatophytes, Candida albicans (26,9%) and Candida sp. (6,6%) among yeasts, Fusarium solani (2,7%) and Fusarium oxysporum (0,9%) among moulds [6]. Most of the epidemiological studies in Africa are conducted using sometimes different laboratory procedures. It is therefore quite important to standardize the techniques used in order to better describe the profile of causative agents circulating in different settings. Our study aims to update the epidemiology of superficial mycoses and the profile of the circulating causative agents in Togo and Senegal.
Materials and Methods
Study area and Patients
This descriptive, prospective study was carried out at two sites: the Parasitology-Mycology laboratories of the Fann University Hospital (SENEGAL) between February 2019 and February 2020; and the Sylvanus Olympio University Hospital (TOGO) between October 2019 and March 2020. All the patients screened during the study period were enrolled.
Samples Collection
Hair, nail or skin fragments from all patients with suspected superficial mycosis (Tinea capitis, tinea ungium, tinea corporis or tinea versicolor) were sampled.
The removal of each lesion was carried out separately with sterile material, before or at distance from any antifungal treatment. Also, each patient was asked to wash the affected areas with ordinary soap and to protect them either with a cap (for ringworm of the scalp) or a sock (for intertrigos, keratodermias, and onychomycosis) before the sampling.
Tinea capitis
After an examination in Wood’s light, the area of alopecia was removed using a scalpel blade and the fluorescent hair was removed using tweezers.
Tinea ungium
The sampling was preceded by cleaning with Dakin and scraping the nail table to remove the superficial part. Then the nail fragments and flakes were collected with a scalpel blade.
Tinea corporis
The sampling started by cleaning with Dakin. Then a scraping on the periphery of the lesion was performed with a scalpel blade to collect the scales.
Tinea versicolor
A piece of tape was applied to the suspect lesion and placed on a microscopy slide.
Mycological Diagnosis
It was carried out with strict adherence to the following four steps: Direct Examination, Culture and Identification.
Direct Examination
Skin scraps, hairs, nails fragments were placed on a microscopy slide with few drops of 30% aqueous potassium hydroxide (KOH) and then covered with a slide. The observation was made under a microscope with x10 and x40 objectives looking for hyphae, isolated or “grape bunch” yeast.
Culture and Identification
Different samples were placed at several points on the surface of Sabouraud Chloramphenicol (SC) and Sabouraud Chloramphenicol plus cycloheximide (SCC) media at 25º C for up to 4 weeks for the culture. The identification of fungal species was done based on their cultural caracteristics including color of the colonies, their shape, relief, consistency, size and looked for the presence of pigment diffusing in the agar. Some particular aspects of dermatophytes were also researched microscopically such as hyphae appearance, presence of chlamydospores, microconidies and macroconidies [7].
The yeasts were identified based on morphological and physiological (germination test) characteristics. The
interpretation of the yeasts and moulds was based on the results of direct examination and the abundance of the colonies [8].
Ethical Considerations
This study has been approved by the Ethics Committee of the Cheikh Anta Diop University of SENEGAL (Reference number: 0413/2019/CER/UCAD) and by the Bioethics Committee for Health Research of TOGO (Reference number: 19/2020/CBRS).
Statistical Analysis
All the data collected from this study were entered into Excel and analyzed using Epi-info 7.2 software. Quantitative data are presented in averages and qualitative data in numbers and percentages.
Results
A total of 602 patients in Senegal and 135 in Togo were sampled. In Senegal we collected 677 samples of which the most common infection site was scalp with 307 (45,34%) of the total cases followed by nail fragments 204 (30,13%) and skin scales 166 (24,51 %). In Togo we collected 143 samples and skin scales was the most common infection site 93 (65,0.3%) followed by nail fragments 41 (28,67%) and scalp 9 (6,29%). 293 (48,67%) and 91 (67,41%) were confirmed to have superficial mycoses respectively in Senegal and Togo. The mean age was 31.21 years (range 0.5-89 years) in Senegal and 32.93 years (range 0.16-75 years) in Togo. Most cases were between 0 and 10 years of age (17,17%) in Senegal and 31 to 40 years of age (22,96%) in Togo (table 1). In both countries, women have been represented more than men, with frequencies of 64.95% in Senegal and 60% in Togo (Table 1).
| SENEGAL | % | TOGO | % | |
|---|---|---|---|---|
| Number | Number | |||
| SEX | ||||
| Female | 391 | 64,95 | 81 | 60 |
| Male | 203 | 33,72 | 52 | 38,52 |
| No precise | 8 | 1,33 | 2 | 1,48 |
| Total | 602 | 100 | 135 | 100 |
| Age Group (Year) | ||||
| 0 -10 | 107 | 17,77 | 9 | 6,67 |
| 20-Nov | 64 | 10,63 | 25 | 18,52 |
| 21 - 30 | 100 | 16,61 | 25 | 18,52 |
| 31 - 40 | 81 | 13,46 | 31 | 22,96 |
| 41 - 50 | 66 | 10,96 | 20 | 14,81 |
| More than 50 | 101 | 16,78 | 19 | 14,07 |
| No precise | 83 | 13,79 | 6 | 4,44 |
| Total | 602 | 100 | 135 | 100 |
| Sampling Type | ||||
| Scalp | 307 | 45,34 | 9 | 6,29 |
| Nail | 204 | 30,13 | 41 | 28,67 |
| Skin | 166 | 24,51 | 93 | 65,03 |
| • ITO | 96 | 14,18 | 43 | 30,06 |
| • K | 48 | 7,09 | 2 | 1,40 |
| • EP | 13 | 1,92 | 20 | 13,98 |
| • PV | 9 | 1,32 | 28 | 19,59 |
| Total | 677 | 100 | 143 | 100 |
Table 1: Socio-demographic and clinical distribution of the population in Senegal and Togo.
ITO: Intertrigo; K: Keratoderma; EP: Epidermophytosis, TV: Tinea versicolor Table 1: Socio-demographic and clinical distribution of the population in Senegal and Togo.
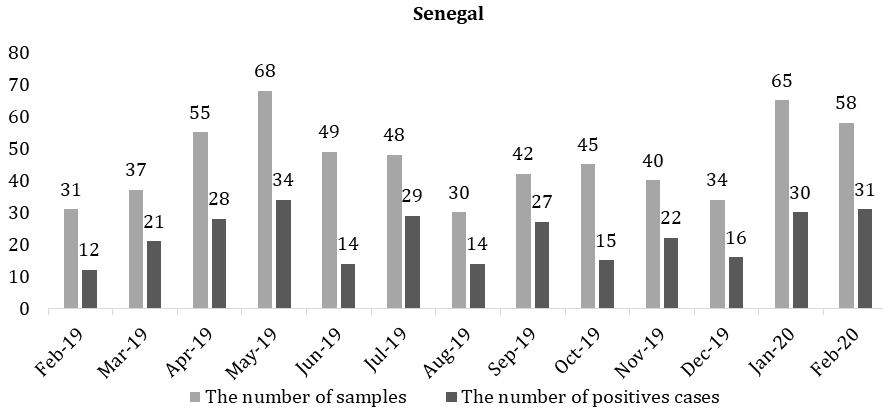
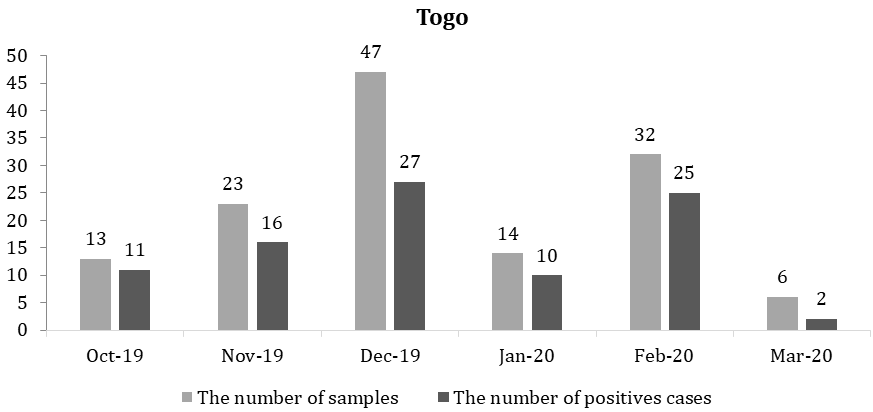
The number of samples and positive cases, in Senegal, varied monthly, with an averages of 46.31 samples and 22.54 positive cases and the most affected month was September with 27 positive cases out of 42 (Figure 1). In Togo the averages of 22.5 samples and 15.17 positive cases were obtained and the month registrated a highest number of positive cases was October with 11 of 13 (Figure 2).
In Senegal, 316 of 677 samples analyzed, were positive with a prevalence of 46.68%. The sampling sites were classified into the following three categories: scalp scales 36.71% (116), nails fragments 32.91% (104) and skin scales 30.38% (96) (Table 2). Overall, 194 (61.39%) were women (most of cases in scalp: 75 followed by nails: 73 and skin: 46) while 118 (37,34%) were men (Table 2). According to the age group, superficial infections were more frequently encountered in children under 10 years (n=74) followed by adults over 50 years (n=62) and those with age from 31 to 40 years. Most of tinea capitis were found in children under 10 years (n=65) while the cases of tinea ungium (n=25) and tinea corporis (n=33) were common in adults over 50 years old (Table 2).
In Togo, 97 of 143 samples collected, were positive with a prevalence of 67,83%. The sampling sites were classified into the following three categories: skin scales 68, 04 (n=66), nails fragments 29,9% (n=29) and scalp scales 2,06% (n=2) (table 2). Overall, 58,76% (n=57) were women (most of cases in skin scales : 35 followed by nails: 22) while 37 (38,14%) were men (Table 2). According to the age group superficial infections were more frequently found in adults aged 31 to 40 years (n=21) followed by those aged 21 to 30 years (n=20). All of tinea capitis cases were found in children under 10 years (n=2) while most cases of tinea ungium (n=8) were found in adult from 21 and 30 years and most of tinea corporis (n=17) in adults from 31 to 40 years old (Table 2).
| Senegal | Togo | |||||||
|---|---|---|---|---|---|---|---|---|
| Scalp | Nails | Skin | Total (%) | Scalp | Nails | Skin | Total (%) | |
| Total Samples | 307 | 204 | 166 | 677 | 9 | 41 | 93 | 143 |
| Positive Samples | 116 | 104 | 96 | 316 (46,68) | 2 | 29 | 66 | 97 (67,83) |
| % | 36,71 | 32,91 | 30,38 | 100 | 2,06 | 29,9 | 68,04 | 100 |
| Sex | ||||||||
| F | 75 | 73 | 46 | 194 (61,39) | - | 22 | 35 | 57 (58,76) |
| M | 40 | 29 | 49 | 118 (37,34) | 2 | 6 | 29 | 37 (38,14) |
| No precise | 1 | 2 | 1 | 4 (0,59) | - | 1 | 2 | 3 (3,1) |
| TOTAL | 116 | 104 | 96 | 316 | 2 | 29 | 66 | 97 |
| Age group (year) | ||||||||
| 0 - 10 | 65 | 6 | 3 | 74 (23,42) | 2 | - | 5 | 7 (7,22) |
| 20-Nov | 9 | 4 | 4 | 17 (5,38) | - | 5 | 12 | 17 (17,53) |
| 21 - 30 | 8 | 18 | 12 | 38 (12,02) | - | 8 | 12 | 20 (20,62) |
| 31 - 40 | 6 | 21 | 16 | 43 (13,61) | - | 4 | 17 | 21 (21,65) |
| 41 – 50 | 2 | 19 | 21 | 42 (13,29) | - | 5 | 7 | 12 (12,37) |
| > 50 | 4 | 25 | 33 | 62 (19,62) | - | 6 | 10 | 16 (16,49) |
| No precise | 22 | 11 | 7 | 40 (12,66) | - | 1 | 3 | 4 (4,12) |
| TOTAL | 116 | 104 | 96 | 316 | 2 | 29 | 66 | 97 |
Table 2: Prevalence of superficial mycoses according to age, sex and sampling site in Senegal and Togo.
In Senegal, 293 patients with single or associated fungus were found, of which 273 (93.1%) isolated and 20 (6.82%) in association. In single infections, T. soudanense was the most common dermatophyte found in 89 or 30.37% cases (Tinea capitis=72, onychomycosis=3, K=3, ITO=2, associations=9) followed by M. langeronii in 21/7.16% cases (Tinea capitis=17, Onychomycosis=1, associations=3). Other dermatophyte species were also found such as T. violaceum in 9 cases (Tinea capitis=7, K=1, associations=1), T. mentagrophytes in 5 cases (Onychomycosis=1, ITO=1, Associations=3), T. rubrum in 5 cases (Tinea capitis=3, associations=2), T. verrucosum in 3 associations and E. floccosum in one case of ITO. Overall, C. albicans/dubliniensis/africana was the most isolated yeast with a prevalence of 26.96% (79 cases), followed by C. sp. with a prevalence of 12.96% (n=38), Malassezia furfur (1.02%, n=3) and Trichosporon sp. (0.34%, n=1). Among the moulds, Fusarium oxysporum was the most found (n=9, %=3.07) followed by Fusarium sp. (n=5, 1.70%), Acremonium sp. (n=2, 0.68%) and Aspergillus candidus, Fusarium sp., Neoscytalidium dimidiatum which were found in the same proportions (Table 3). In co-infections, we found associations between dermatophytes (T. soudanense + M. langeronii), between yeasts and dermatophytes (T. soudanense associated with C.
In Togo, 91 patients with single or associated fungus were found including 88 (96.70%) isolated and 3 (3.27%) in associations. In single infections the most common dermatophytes were T. mentagrophytes (n=8, %=8.79, ITO=6, Onychomycosis=2) and T. rubrum (n=8, %=8.79, ITO=3, EP=3, Onychomycosis=1, associations=1). Other species of dermatophytes were found with, in decreasing order: T. soudanense (n=3, %=3.29, ITO=2, association=1), T. tonsurans (n=3, %=3.29, Onychomycosis=1, ITO=1, EP=1), M. langeronii (n=2, %=2.19, tinea capitis=1, EP=1), E. floccosum (n=2, %=2.19, EP=2) and T. verrucosum (n=1, %=1.09, EP=1). As far as yeasts are concerned, the following results were obtained in descending order: M. furfur (n=26), C. albicans (n=18), C. sp. (n=10), Trichosporon sp. (n=5). The moulds found were Fusarium sp. (n=1) and Neoscytalidium dimidiatum (n=1) (Table 4). In co-infections we found three associations including T. mentagrophytes + C. sp. (n=1), C. albicans + T. rubum (n=1) and C. albicans + A. sp (n=1) (Table 4).
albicans and C. sp.), between dermatophytes and moulds (T. verrucosum + F. sp. and F. oxysporum + T. mentagrophytes) and the rest between yeasts and moulds (Table 3).
Genus species Tinea capitis(a) Onycho mycosis (b) Tinea corporis Co-Infections Total (%) ITO (c) K (d) EP (e) PV (f) Single Infections Trichophyton T. violaceum 7 - - 1 - - a+c (1) 9 (3,07) T. rubrum 3 - - - - - a+d (1); a+b (1) 5 (1,70) Microsporum M. langeronii 17 1 - - - - a+b (2); a+e (1) 21 (7,16) Epidermophyton E. floccosum - - 1 - - - - 1 (0,34) Candida Trichosporon T. sp. - 1 - - - - - 1 (0,34) Malassezia M. furfur - - - - - 3 - 3 (1,02) Aspergillus A. candidus - 1 - - - - - 1 (0,34) Acremonium A. sp. - - 2 - - - - 2 (0,68) Fusarium F. oxysporum - 3 6 - - - - 9 (3,07) F. solani - - 1 - - - - 1 (0,34) F. sp. - 2 3 - - - - 5 (1,70) Neoscytalidium N. dimidiatum - - - 1 - - - 1 (0,34) Total 99 73 39 15 2 3 42 273 (93,17) Co-Infections T. soudanense + M. langeronii 1 - - - - - - 1 (0,34) T. soudanense + C. albicans - 1 - 1 - - a+b+d (1) 3(1,02) S. apiospermum + C. sp. - - - - - - b+e (1) 1 (0,34) F.sp. + T. verrucosum - - - - - - a+c (1) 1 (0,34) F. oxysporum + T. mentagrophytes - - 1 - - - - 1 (0,34) F. oxysporum + C. albicans - - - - - - b+c (1) 1 (0,34) C. sp. + T. soudanense - 1 - - - - b+c (1) 2 (0,68) C. sp. + O. sp. - - - - - - b+c (1) 1 (0,34) C. sp. + F. sp. - 1 - - - - c+d (1) 2 (0,68) C. sp. + F. oxysporum - - 1 - - - - 1 (0,34) C. albicans + F. sp. - 2 - - - - b+c (1) 3 (1,02) C. albicans + F. solani - - - - - - c+d (1); b+c (1) 2 (0,68) C. albicans + A. candidus - - - - - - b+c (1) 1 (0,34) Total 1 5 2 1 - - 11 20 (6,82) T. mentagrophytes - 1 1 - - - c+d (1); b+c (2) 5 (1,70) T. soudanense 72 3 2 3 - - a+d (1); a+b (7); a+e (1) 89 (30,37) T. verrucosum - - - - - - c+d (1); a+b(1); a+e (1) 3(1,02) C. albicans/ dubliniensis / africana - 44 13 4 2 - d+b (2); b+c (10); a+c (3); a+b+e (1) 79 (26,96) C. sp. - 17 10 6 - - b+c (2); a+c (1); a+b (2) 38 (12,96)
- ITO: Intertrigo; K: Keratoderma; EP: Epidermophytosis, TV: Tinea versicolor.
Table 3: Distribution of species found in single infections and co-infections depending on the indications in Senegal.
| Genus | Species | Tinea capitis (a) | Onychomycosis (b) | Tinea corporis | Co- Infections | Total (%) | |||
|---|---|---|---|---|---|---|---|---|---|
| ITO (c) | K (d) | EP (e) | TV (f) | ||||||
| Single Infections | |||||||||
| Trichohyton | T. mentagrophytes | - | 2 | 6 | - | - | - | - | 8 (8,79) |
| T. soudanense | - | - | 2 | - | - | - | c+e (1) | 3 (3,29) | |
| T. verrucosum | - | - | - | - | 1 | - | - | 1 (1,09) | |
| T. tonsurans | - | 1 | 1 | - | 1 | - | - | 3 (3,29) | |
| T. rubrum | - | 1 | 3 | - | 3 | - | c+e (1) | 8 (8,79) | |
| Microsporum | M. langeronii | 1 | - | - | - | 1 | - | - | 2 (2,19) |
| Epidermophyton | E. floccosum | - | - | - | - | 2 | - | - | 2 (2,19) |
| Candida | C. albicans :dubliniensis/ africana | - | 10 | 4 | - | 1 | - | b+c (3) | 18 (19,78) |
| C. sp. | - | 8 | 2 | - | - | - | - | 10 (10,98) | |
| Trichosporon | T. sp. | *1 | 1 | 3 | - | - | - | - | 5 (5,49) |
| Malassezia | M. furfur | - | - | - | - | - | 26 | - | 26 (28,57) |
| Fusarium | F. sp. | - | - | - | - | - | - | d+b (1) | 1 (1,09) |
| Neoscytalidium | N. dimidiatum | - | 1 | - | - | - | - | - | 1 (1,09) |
| Total | 2 | 24 | 21 | - | 9 | 26 | 6 | 88 (96,70) | |
| Co-Infections | |||||||||
| T. mentagrophytes + C. sp. | - | - | 1 | - | - | - | - | 1 (1,09) | |
| C. albicans + T. rubum | - | - | - | - | - | - | c+e (1) | 1 (1,09) | |
| C. albicans + A. sp. | - | 1 | - | - | - | - | - | 1 (1,09) | |
| Total | - | 1 | 1 | - | - | - | 1 | 3 (3,27) |
Table 4: Distribution of species found in the single infections and co-infections depending on the indications in Togo.
ITO: Intertrigo; K: Keratoderma; EP: Epidermophytosis, TV: Tinea versicolor. * It was a case of white piedra Table 4: Distribution of species found in the single infections and co-infections depending on the indications in Togo.
Discussion
Our study was carried out over a period of 1 year in Senegal (February 2019 to February 2020) and 6 months in Togo (October 2019 to March 2020), revealing overall prevalence rates of superficial fungal diseases of 48.67% and 67.41% respectively. The prevalence rate found in Togo is very high compared to the figure in Senegal despite the study period half shorter than the one in Senegal. This could be explained, partly, by the quasi-absence of a mycology laboratory in Togo, whereas mycoses are the main reason for consulting a dermatology clinic, according to a study by Kombate K, et al. [9]; and also, partly, by the socio-economic circumstances which makes access to care difficult [10]. Our prevalence, however, is above the 34.2% reported by Diongue K, et al. [6] between 2011 and 2015 and those reported in other studies: 42.7% (EMR + CULT +) by Silva-Rocha et al. in northeast Brazil, 36.3% by Faure-cognet O, et al. [12], in the Grenoble region and 32% by Zahra VL, et al. in Malta [11, 12, 13].
Our high prevalence rates reported could be explained by the climatic conditions that prevailed in both countries during the study period. Indeed, hot weather conditions prevailed almost all along our study period in both countries, making it easier for fungi to proliferate. Moreover, a study conducted in Mali (located in the same region as Togo and Senegal) by Coulibaly et al. reported a prevalence of 52.9%, which is in line with our results.
Distribution by gender showed that superficial fungal infections are more frequent among women than men, with prevalences of 61.39% in Senegal and 58.76% in Togo. This same trend was reported by Silva-Rocha (64.6%) in northeast Brazil [11]. This predominance of women is maintained in positive hair and nail samples in Senegal and in positive nail and skin samples in Togo. On the contrary, men were more represented in positive skin samples in Senegal and in positive hair samples in Togo. These observations could be explained by several reasons, namely, attendance of hair salons, performance of household chores, and the wearing of tight clothing by either men or women, from one category of samples to another.
A high prevalence of superficial mycoses is observed in Senegal among young patients (under 10 years of age) and in Togo among patients between 31 and 40 years of age. This is probably due in part to their representation in our sample (in Senegal children less than 10 years of age were the most numerous and in Togo patients between 31 and 40 years of age were the most numerous). The other probable reason is that in Senegal we found more ringworm of the scalp (common in infants) and in Togo more Pityriasis versicolor (common in young adults) [14, 15]. This could also explain the fact that the majority of our positive cases were found in scalp specimens (36.71%) in Senegal and in skin samples (68.04%) in Togo.
Almost the same species of dermatophytes are to be found in both countries except for Trichophyton violaceum found only in Senegal and Trichophyton tonsurans found only in Togo. Since the two countries are located in the same region, it seems logical to find the same species in both countries except for a few. On the contrary, Trichophyton soudanense (30.37%) is the predominant dermatophyte in Senegal while in Togo Trichophyton rubrum and Trichophyton mentagrophytes are the predominant species (8.79% each). We have no previous data on the epidemiology of superficial mycoses in Togo as this is the first study, however in Senegal, previous studies have revealed a predominance of Trichophyton soudanense [4, 6]. Trichophyton rubrum and Trichophyton mentagrophytes, following each other in first place, have been reported in other studies [10, 12, 16, 17, 18]. The three predominant dermatophytes found in our study are consistent with the observations made by Binazzi M, et al. [19].
Candida albicans was predominant with a prevalence of 26.96% in Senegal, which confirms the results reported by Diongue K, et al. in Senegal [6], who attributed this observation to the wide distribution of this yeast and its commensal character. In Togo, Malassezia furfur was the most often isolated yeast with a prevalence of 28.57%. This observation is logical considering that tinea versicolor is one of the most common pigmentation disorders in the world, frequently observed in tropical regions with a prevalence of up to 40% [20].On the other hand, in Senegal it accounted for 1.02% of superficial mycoses. Indeed, the case of Senegal is quite particular because the majority of our cases of pityriasis versicolor received at the laboratory, claimed to have already made treatments without prior mycological diagnosis, a treatment which in the end did not work. This demonstrates a trend among clinicians to directly prescribe treatments in cases that were not diagnosed as mycological and therefore the patient only arrived at the laboratory when the perceived treatment did not work. We therefore believe that the prevalence rate we found may not reflect the reality of this pathology in the Senegalese population. We also found in our study a case of Trichosporon in the scalp (in Togo). This was a case of white piedra rarely reported in West Africa although most cases occur in tropical regions [14].
The genus Fusarium, which dominates moulds in Senegal, is found in the same proportions as other moulds in Togo. Usually found in soil, they are increasingly involved in human pathology [21, 22]. They determine, as superficial pathologies, onychomycosis, keratitis and more rarely intertrigos, which are increasingly described in the literature [6, 21, 23].
Conclusion
Superficial mycoses remain a real public health issue in Togo and Senegal. The same species are present in both countries with the exception of Trichophyton tonsurans, Trichophyton violaceum and Aspergillus candidus. Dermatophytes are dominated by Trichophyton soudanense in Senegal and Trichophyton rubrum/mentagrophytes in Togo. Yeasts and moulds are dominated by Candida albicans and the genus Fusarium in both countries. Children less than 10 years of age are the most affected in Senegal while adults between 31 and 40 years of age are the most affected in Togo. This study has allowed us to screen the species responsible for superficial mycosis in both countries, which could improve their management.
References
-
Simonnet C, Berger F, Gantier JC (2011) Epidemiology of superficial fungal diseases in French Guiana: a three- year retrospective analysis. Med Mycol 49(6): 608‑611.
-
Rodrigues ML, Nosanchuk JD (2020) Fungal diseases as neglected pathogens: A wake-up call to public health officials. Plos Negl Trop Dis 14(2): e0007964.
-
Havlickova B, Czaika VA, Friedrich M (2008) Epidemiological trends in skin mycoses worldwide. Mycoses 51(S4): 2‑15.
-
Ameen M (2010) Epidemiology of superficial fungal infections. Clin Dermatol 28(2): 197‑201.
-
Zhan P, Liu W (2017) The Changing Face of Dermatophytic Infections Worldwide. Mycopathologia 182(1-2): 77‑86.
-
Diongue K, Diallo MA, Ndiaye M, Badiane AS, Seck MC, et al. (2016) Causative agents of superficial mycoses isolated in Dakar, Senegal: Retrospective study from 2011 to 2015. J Mycol Med 26(4): 368‑376.
-
Chabasse D, Bouchara JP, De Gentile L, Brun S, Cimon B, et al. (2004) Les dermatophytes. Cahier de formation Bioforma, pp: 159.
-
Bouchara JP, Pihet M, de Gentile L, Cimon B, Chabasse D (2010) Les levures et levuroses. Bioforma Paris, pp: 201.
-
Kombaté K, Saka B, Mouhari-Toure A, Barruet RK, Gnassingbé W, et al. (2014) Skin pathology in the elderly in dermatology in Lome, Togo: study of 325 cases. Pan Afr Med J 18: 151.
-
Zida A, Barro-Traoré F, Dera M, Bazié Z, Niamba P, et al. (2015) Epidemiological and etiological aspects of superficial fungal infections among prison inmates in Ouagadougou, Burkina Faso. J Mycol Med 25(2): e73-e79.
-
Silva-Rocha WP, de Azevedo MF, Chaves GM (2017) Epidemiology and fungal species distribution of superficial mycoses in Northeast Brazil. J Mycol Med 27(1): 57‑64.
-
Faure-Cognet O, Fricker-Hidalgo H, Pelloux H, Leccia MT (2016) Superficial Fungal Infections in a French Teaching Hospital in Grenoble Area: Retrospective Study on 5470 Samples from 2001 to 2011. Mycopathologia 181(1-2): 59‑66.
-
Zahra VL, Gatt P, Boffa MJ, Borg E, Mifsud E, et al. (2003) Characteristics of superficial mycoses in Malta. Int J Dermatol 42(4): 265‑271.
-
Bonifaz A, Gómez-Daza F, Paredes V, Ponce RM (2010) Tinea versicolor, tinea nigra, white piedra, and black piedra. Clin Dermatol 28(2): 140‑145.
-
Gupta AK, Batra R, Bluhm R, Faergemann J (2003) Pityriasis versicolor. Dermatol Clin 21(3): 413‑429.
-
Adefemi SA, Abayomi MA, Abu JM (2010) Superficial fungal infections seen at a tertiary health centre: clinical and mycological studies. West Afr J Med 29(4): 267‑270.
-
Di Chiacchio N, Madeira CL, Humaire CR, Silva CS, Fernandes LHG, et al. (2014) Superficial mycoses at the Hospital do Servidor Público Municipal de São Paulo between 2005 and 2011. An Bras Dermatol 89(1): 67‑71.
-
Coloe S, Baird R (2010) Dermatophyte infections in Melbourne: Trends from 1961/64 to 2008/09. Australas J Dermatol 51(4): 258‑262.
-
Binazzi M, Papini M, Simonetti S (1983) Skin mycoses--geographic distribution and present-day pathomorphosis. Int J Dermatol 22(2): 92‑97.
-
Schwartz RA (2004) Superficial fungal infections. Lancet 364(9440): 1173‑1182.
-
Bissan AT, Iken M, Doumbia M, Ou-Khedda N, El- Alaoui M, et al. (2017) Fusarioses to Fusarium solani in an immunocompetent and immunocompromised diagnosed in military hospital of Rabat. J Mycol Med 27(3): 382‑386.
-
Néji S, Trabelsi H, Cheikhrouhou F, Sellami H, Guidara R, et al. (2013) Fusariosis diagnosed in the laboratory of an UH in Tunisia: Epidemiological, clinical and mycological study. J Mycol Med 23(2): 130‑135.
-
Anane S, Chtourou O, Chedi A, Kaouech E, Belhadj S, et al. (2009) Tinea pedis due to Fusarium solani. J Mycol Med 19 (3): 200‑202.
- Diversity of Candida sp and Antifungal Susceptibility Patterns in Digestive Candidiasis among People Living with HIV in CHU of Libreville, Gabon
- Vulvovaginal candidiasis: Retrospective study (2019- 2021) at the Centre Hospitalier National de Pikine, Suburban Dakar, Senegal
- Identification of Environmental Fungal Species in Clinical Services of University Hospital of Angre, Abidjan (Cote d’Ivoire)
- New Location of some Gasteroid Basidiomycetes in Western Kazakhstan
- Evaluation of Various Extracellular Enzymes of Ectomycorrhizal Mushrooms
- Morphology and Phylogeny of Lactarius Wallichianae sp. nov and Xerula magnispora sp. nov. from India