Mucormycosis Caused by Lichtheimia Spp. (Clinical Case, Overview of Register Data and Literature Review)
The article presents the first case of disseminated mucormycosis caused by Lichtheimia ornata, as well as an overview of our register data and analysis of publications on mucormycosis caused by Lichtheimia spp. Main underlying conditions in our patients with Lichtheimia mucormycosis were hematological malignancies (83%). Main risk factor was prolonged (median -47 days) severe neutropenia (72%), and steroids were used relatively rarely (55%). Lichtheimia mucormycosis was severe disease with ≥ 2 organs involvement in 66% patients. Combination therapy (lipid forms amphotericin B with echinocandins) and surgical treatment were often used for the treatment of Lichtheimia mucormycosis. The 12-weeks overall survival rate of patients with Lichtheimia mucormycosis was 44%.
Introduction
Mucormycosis (zygomycosis) is a severe opportunistic infection with a high mortality rate. The causative agents of mucormycosis are fungi belonging to the order Mucorales of the phylum-Mucoromycota [1, 2]. Lichtheimia spp. are common pathogens of mucormycosis [3, 4]. The genus Lichtheimia includes six species: L. blakesleeana, L. brasiliensis, L. sphaerocystis, L. corymbifera, L. ornata, and L. ramosa, the last three are recognized as clinically important [5, 6, 7]. L. ornata is a cryptic species, phenotypically indistinguishable from L. corymbifera. This species can only be identified by molecular genetic methods. We present the first case of disseminated mucormycosis caused by L. ornata. We also provide an overview of our register data and a review of publications on mucormycosis caused by Lichtheimia spp.
Materials and Methods
The article reports a clinical case of disseminated mucormycosis caused by L. ornata in a patient with chronic lymphocytic leukemia. The ECMM/MSG ERC 2020 criteria were used for the diagnosis of mucormycosis [3].
Mycological Study
Direct microscopy of biomaterials (aspirate from the paranasal sinuses, biopsy of the maxillary sinus mucosa) was performed by the “wet smear” method, using a 10% solution of KOH in a 10% aqueous solution of glycerol with the addition of a solution of white calcofluor as a mounting fluid. The preparations were examined in a Leica DM LB2 fluorescence microscope at magnifications of 100X, 200X, and 400X.
The biomaterials were cultured on Sabouraud agar medium and incubated at temperatures of 28° and 35°C.
The isolated mold culture was identified by morphological features, and then species identification was conducted by DNA sequencing methodology recommended by the Clinical and Laboratory Standards Institute documents (ММ18-А, CLSI). Species identification was performed by ITS region DNA sequencing with ITS-5 (5`-GGAAGTAAAAGTCGTAACAAGG-3`) and ITS-4 (5`- TCCTCCGCTTATTGATATGC-3`) primers and the TEF1α gene locus sequencing with Al33_ F1 (5`-GAYTTCATCAAGAACATGAT-3`) and Al33_R2 (5`-GACGTTGAADCCRACRTTGTC-3`) primers, using BigDye Terminator v3.1 Cycle Sequencing Kit (Applied Biosystems, Austin, TX, USA) on an ABI PRISM 3500 Genetic Analyzer (Applied Bio systems, USA).
We analyzed the literature for the last 10 years in the databases PubMed (January 2021) and Web of Science (January 2020). When searching for information, we used the keywords: Lichtheimia spp., Lichtheimia ornata, mucormycosis, and zygomycosis.
Case Report
Patient K. 74 years old was hospitalized in the Department of Hematology in May 2012. Complaints: severe weakness increased sweating at night and fever (38.5°C) for three days.
Anamnesis. The patient was diagnosed with chronic lymphocytic leukemia in March 2002 and received chlorambucil from August 2004 to 2006. In June 2009, cytostatic therapy (fludarabine, cyclophosphamide, and rituximab (FCR)) was continued.
In November 2011, Bowen’s disease (intraepidermal squamous cell carcinoma of the lower third of the right tibia T0N0M0) was diagnosed and surgical treatment was performed. Since August 2011, she suffered from pain in the lower jaw on the right. She repeatedly went to the dentist, was diagnosed with odontogenic periostitis, and received antibacterial therapy without clinical effect. In January 2012 according to the results of a biopsy of the right submandibular lymph node, chronic lymphocytic leukemia was suspected, and the patient was hospitalized in the Department of Hematology.
The progression of chronic lymphocytic leukemia was diagnosed in April 2012 and the first course of FCR chemotherapy (fludarabine, cyclophosphamide, rituximab) was performed. After the treatment, the patient had severe neutropenia (< 0.5*109/l), lymphocytopenia (< 1.0*109/l), and anemia.
After discharge from the hospital, the patient noted an increase in body temperature to 38.5° C. On 02.05.2012, the patient was hospitalized for the next course of chemotherapy. During the examination on the first day of hospitalization in the clinical blood test: white blood cells -0,8*109/l (neutrophils– 0,4*109/l), hemoglobin -92g/l, platelets -77*109/l. The patient was treated with antibiotics and antifungals prophylaxis -fluconazole starting dose of 800mg/ day, then 600mg/day. During the treatment, the patient had pain in the area of the maxillary sinus on the right, later there was redness and swelling of the paranasal area. On the next day, the skin in the area of inflammation became cyanotic, there were foci of necrosis, the area of edema spread to the periorbital zone (Figure 1).

The patient’s condition worsened: the intoxication and impaired consciousness progressed. On 10.05.2012, a surgical sanation of the sinuses was performed with the collection of material for culture and microscopy and biopsy. Then fluconazole was replaced with posaconazole at a dose of 800 mg/day.
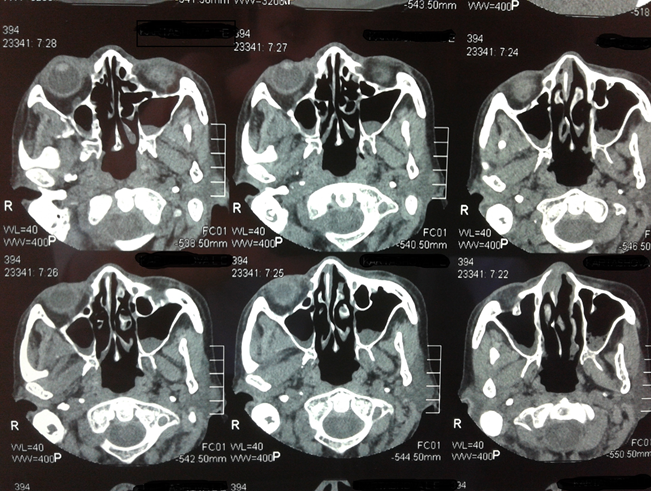
Severe neutropenia persisted. According to the chest CT scan, no focal or infiltrative changes were detected. CT of the paranasal sinuses -swelling of the mucous membrane of the maxillary sinuses, swelling of the soft tissues of the face of the paranasal region (Figure 2).
MRI of the head (14.05.2012): the picture of moderate mixed replacement hydrocephalus; foci in the brain substance; changes in signal intensity and signs of edema of the soft tissues of the face; inflammatory changes in the paranasal sinuses.
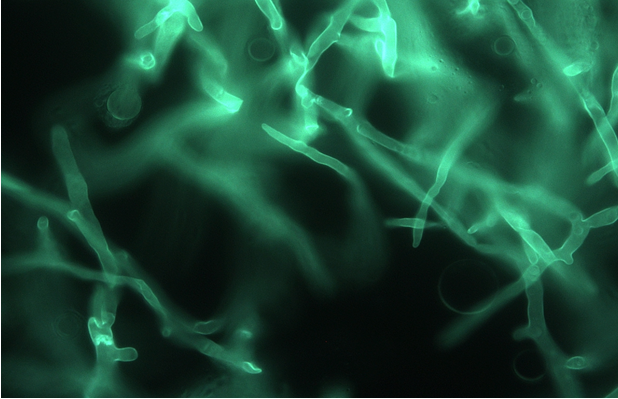
Mycological investigation by microscopy and the biopsy revealed non-septate hyphae branching at right angles in the paranasal sinuses tissue (Figure 3).
The culture was obtained and identified by morphological features as Lichtheimia corymbifera (Figure 4). The isolate was deposited into the Russian Collection of Pathogenic Fungal Cultures (RCPF) at Kashkin Research Institute of Medical Mycology (Collection strain number 1507).
We diagnosed rhinocerebral mucormycosis (the causative agent -Lichtheimia corymbifera) and recommended antifungal therapy (liposomal amphotericin B 5 mg/kg/day or amphotericin lipid complex 5 mg / kg / day), correction of risk factors, surgical removal of necrotic tissues, control studies (cultures of excreta from paranasal sinuses, histological examination of postoperative material, сhest and paranasal sinuses CT scans, MRI of the brain).
Treatment was started with amphotericin B deoxycholate at a dose of 50 mg/day for 2 days, followed by lipid complex amphotericin B at a dose of 3 mg/kg/day. We noted the progression of the underlying disease. Severe thrombocytopenia was the reason for the refusal of radical surgical treatment. The patient died 6 days after the start of antifungal therapy.
Autopsy report: disseminated mucormycosis with lesions of the skin of the face, the soft and hard palate, the sinuses and the ethmoid bone, tissues of the both eyes and the basal parts of brain, both lungs, gastric and intestinal tissues (microscopy on 17.05.12 revealed hyphae of mucoromycetes).
The described case is the first reported proven disseminated mucormycosis caused by Lichtheimia o_r_nata. We conducted a molecular genetic study of mucormycetes cultures stored in the Russian Collection of Pathogenic Fungi. The isolate from this patient was identified as L. ornata by sequencing the ITS region of ribosomal RNA. The analysis showed that L. ornata was grouped with the type strain CBS 291.66 and differed unambiguously from L. corymbifera [6, 8].
The analysis of nucleotide sequences of the ITS region (access number in the Genbank database JX661052, and the LSU locus, JX961703) was obtained in the course of an earlier study. A search by the Blast tool revealed that the sequences assigned to the species L. ornata, L. corymbifera, and L. ramosa have the greatest similarity to the sequences of the RCPF 1507 strain. It was not possible to accurately determine the species by this approach.
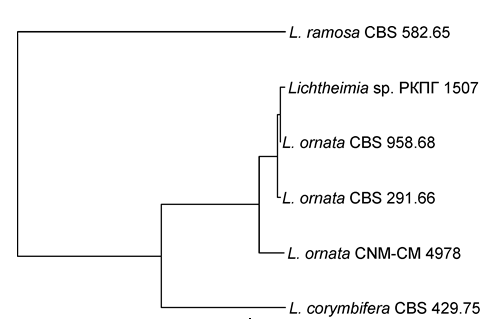
Therefore, we prepared the alignment of the nucleotide sequences of the type and reference strains of the listed species from the taxonomic work of Grit Walther and co- authors [6]. From the final concatenated alignment, an insertion with a length of about 140 bp, belonging to the ITS region of the L. ramosa strain CBS 582.65, was removed. On the tree calculated by the maximum likelihood method in the program PhyML v3.1 [13] of the package SeaView 5.0.4 [14], the sequences of the strain RCPF 1507 were clustered with the sequences of the species L. ornata (Figure 5).
Results
In the period from 2002 to 2020 we observed 64 patients with mucormycosis confirmed by the results of a culture. The median age of the patients was 35 yrs (range 0-74), children -21%, and males 61%. We analyzed the risk factors, clinical manifestations, treatment and survival of patients in groups with different causative agents of mucormycosis (Lichtheimia spp. vs non-Lichtheimia spp.). The causative agents of Lichtheimia mucormycosis were: Lichtheimia corуmbifera (72%), Lichtheimia ramosa (22%), and Lichtheimia ornata (5,5%, n=1). In non-Lichtheimia group: Rhizopus spp. (54%, n=25), Rhizomucor spp. (30%, n=14), and Mucor spр. (15%, n=7).
In the period from 2002 to 2020 we observed 18 patients with Lichtheimia mucormycosis and 46 non-Lichtheimia mucormycosis. In the first group of patients median age was 32 yrs (range 0-74), children -33%, and males 50%. In the second group of patients mean age was 37 yrs (range 5-69), сhildren -15%, and males -66%.
Underlying conditions were hematological malignancies (83% vs 76%), trauma/ burns (11% vs 9%), diabetes mellitus (5,5% vs 4%), and COPD or tuberculosis (0% vs 11%) (Table 1). The most frequently mucormycosis developed in patients with acute leukemia (55.5% vs 42%). Neuroblastoma, Hodgkin’s or non-Hodgkin’s lymphoma, aplastic anemia, Fanconi’s anemia, myelodysplastic syndrome, myeloid sarcoma and multiple myeloma were less frequent as underlying diseases.
| Lichtheimia-mucormycosis n=18 | non-Lichtheimia mucormycosis n=46 | |
|---|---|---|
| Hematological malignancies: | 83% | 76% |
| Acute myeloid leukemia | 39% | 22% |
| Acute lymphoblastic leukemia | 16,5% | 20% |
| Aplastic anemia | 11% | 0 |
| Hodgkin lymphoma | 0 | 9% |
| Non-Hodgkin lymphoma | 5,5% | 9% |
| Chronic lymphocytic leukemia | 5,5% | 4,5% |
| Chronic myeloid leukemia | 5,5% | 2,2% |
| Myelodysplastic syndrome | 0 | 2,2% |
| Neuroblastoma | 0 | 2,2% |
| Fanconi's anemia | 0 | 2,2% |
| Multiple myeloma | 0 | 2,2% |
| Trauma/ burns | 11% | 9% |
| Diabetes Mellitus | 5,5% | 4,5% |
| COPD or Tuberculosis | 0 | 11% |
Table 1: Underlying diseases in patients with mucormycosis.
The study of risk factors showed that mucormycosis mainly developed after 3 vs 5 courses of chemotherapy. Prolonged severe nuetropenia was detected in 72% vs 63% of patients, with a median duration for 47 and 39 days. Lymphocytopenia was determined in 72% vs 60% of patients with a median duration for 48 and 39 days. Only 55% of patients with Lichtheimia-mucormycosis received steroids.
Glucocorticosteroids were significantly more frequently used in patients with non- Lichtheimia mucormycosis 80%* (р=0,049). The average duration of corticosteroid use was 35 vs 31 days. Mucormycosis developed in 38% vs 46% patients after allogeneic HSCT. These and other risk factors are presented in Table 2.
| Lichtheimia-mucormycosis n=18 | non-Lichtheimia mucormycosis n=46 | |
|---|---|---|
| Chemotherapy | 83% | 76% |
| Number of courses of chemotherapy | median -3 | median -5 |
| Severe neutropenia | 72% | 63% |
| Duration of severe neutropenia, days | median -47 | median -39 |
| Lymphocytopenia | 72% | 60% |
| Duration of lymphocytopenia, days | median -48 | median -39 |
| Glucocorticoid therapy | 55%* | 80%* (p=0,049) |
| Duration of glucocorticoid therapy, days | median -35 | median -31 |
| Allogeneic HSCT | 38% | 46% |
| Treatment in the ICU | 50% | 60% |
| Diabetic ketoacidosis | 5,5% | 4,5% |
Table 2: Risk factors and background conditions in patients with mucormycosis.
The study showed that the primary focus of infection most often was located in lungs. Significantly more often in patients with Lichtheimia mucormycosis, rhinocerebral mucormycosis developed and significantly less often lung damage. Lichtheimia mucormycosis was more severe disease in almost half of the patients in the study, we observed widespread mucormycosis with ≥ 2 organs involvement (skin, mucous membranes of the paranasal sinuses, orbital tissues, osteomyelitis of the walls of the paranasal sinuses and orbit, the spread of infection in the central nervous system) (Table 3).
| Lichtheimia mucormycosis n=18 | non-Lichtheimia mucormycosis n=46 | |
|---|---|---|
| Lungs | 55%* | 80%*, (p=0,043) |
| Skin and soft tissues | 50%* | 9%*, (p=0,0001) |
| Bones | 38%* | 6,5%*, (p=0,001) |
| Paranasal sinuses | 33% | 15% |
| Central nervous system | 27% | 13% |
| Gastrointestinal tract | 22% | 6,5% |
| ≥2 organs involvement | 66%* | 22%*, (p=0,0004) |
Table 3: Clinical forms of mucormycosis depending on the pathogen.
The main clinical symptoms of mucormycosis were fever (above 38.50С), cough, bleeding and local pain. Fever above 38,50С was observed in 83% vs 86 % of patients. The cough was noted in 80% vs 80% of patients, who had primary lung involvement. The haemoptysis 30% vs 28% and local pain 61% vs 44%. All patients with primary lesion of paranasal sinuses had local pain in and 66% vs 70% of them had signs of bleeding. Patients with gastrointestinal mucormycosis had sings of “acute abdomen” with gradually increasing intensity of pain.
CT scans of lungs were performed in all patients. All patients with pulmonary mucormycosis had focal infiltrative changes on CT. 40% vs 48% of patients had bilateral lesions. In
addition, 44% of the patients with Lichtheimia mucormycosis had hydrothorax, and only 30% with non -Lichtheimia pulmonary mucormycosis. Specific symptoms of mycotic lung involvement as “reversed halo sign” were observed 44% vs 28% of the patients. CT scans of paranasal sinuses were performed in 66% vs 55% of patients. Symptoms of sinusitis were determined in 33% vs 15% of the patients.
In order to identify the pathogen bronchial lavage fluid, pleural fluid, cerebrospinal fluid and sinus aspirate and biopsies were examined. Non-septate mycelium branching at right angles was identified with direct microscopy and/or on histology in 100% of patients. Histological examination was done in 72% and 46% of patients (p=0,05).
Antifungal therapy of mucormycosis received 88% vs 80% of patients. Mucormycosis was treated with amphotericin B lipid complex (66% vs 41%), posaconazole (50% vs 69%), amphotericin B (38% vs 42%), echinocandins (50% vs 24%, p=0,05), voriconazole (0 vs 3%), and liposomal amphotericin B (8% vs 4%). The medians days of treatment were 30 vs 70 accordingly (Table 4).
| Lichtheimia-mucormycosis n=18 | non- Lichtheimia mucormycosis n=46 | |
|---|---|---|
| Amphotericin B lipid complex | 66% | 41% |
| Posaconazole | 50% | 69% |
| Amphotericin B | 38% | 42% |
| Echinocandins | 50% | 24%, p=0,028 |
| Voriconazole | 0 | 3% |
| Liposomal amphotericin B | 8% | 4% |
| Combined therapy | 61% | 31%, p=0,01 |
| Surgery | 72% | 35%, p=0,047 |
Table 4: Treatment of mucormycosis depending on the pathogen.
Combined therapy was given to 61%* vs 31%* of patients. Combinations of echinocandins, voriconazole, with a lipid amphotericin B, amphotericin B or posaconazole were used predominantly.
Surgical treatment (sinusotomy, lobectomy, resection of ribs, bowel resection, surgical debridement of skin and soft tissues) was performed in 72% vs 35%* (p=0,007) of patients.
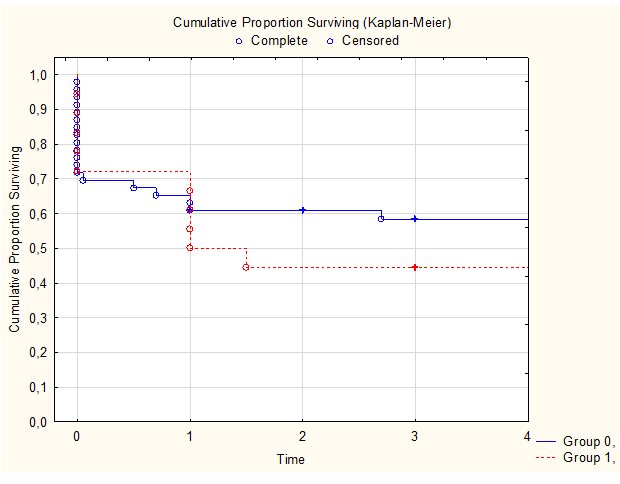
The main criterion for assessing the effectiveness of antifungal therapy was the overall survival rate of patients with mucormycosis. The 12-weeks overall survival rate of patients treated with antifungal therapy after 3 months were 44% vs 59% (Figure 6). The medians survival in both groups were 1,5 vs 3 months.
Discussion
The prevalence of Lichtheimia spp. among the causative agents of mucormycosis varies significantly between geographical regions. In recent European studies, Lichtheimia spp. (L. corymbifera -84%) was the cause of 17.5-42% of cases of mucormycosis [8, 9, 10, 11, 12]. However, since L. ramosa and L. corymbifera have long been used as synonyms, and L. ornata has only recently been identified as a separate species, a correct assessment of the occurrence of this species is difficult [9].
The literature analysis also shows that hematological malignancies (up to 80%), especially acute myeloid leukemia, are the most frequent background diseases in patients with mucormycosis caused by Lichtheimia spp. [8, 9, 10, 11, 12]. The main risk factors for the development of mucormycosis are long-term severe neutropenia, immunosuppressive and high-dose cytostatic therapy, as well as long-term use of glucocorticosteroids. In our case patient mucormycosis developed against the background of chronic lymphocytic leukemia, during the period of severe neutropenia. We obtained similar data: in 83% of patients Lichtheimia mucormycosis developed against the background of hematological diseases. More than half of these patients had acute leukemia (55.5%).
A recent meta-analysis of published cases of mucormycosis showed that Lichtheimia spp. are most often the cause of skin and deep tissue lesions, while it should be taken into account that most of the cases considered were described in Africa [8, 12]. In Europe, the main clinical variant caused by Lichtheimia spp. mucormycosis was pulmonal [4, 8, 11].
An analysis of our registry showed that Lichtheimia almost equally often affects the lungs and the skin with soft tissues. In two-thirds of patients with Lichtheimia spp. mucormycosis infection affects 2 or more organs and rapidly spreads to the surrounding tissues.
According to international recommendations, the main antifungal drugs for the treatment of mucormycosis are liposomal amphotericin B, amphotericin B lipid complex, isavuconazole and posaconazole [7].
An analysis of publications has shown that in the treatment of Lichtheimia-_related spp. mucormycosis the use of lipid forms of amphotericin B is also more common (65- 80%) [4, 11, 12]. Pan J, et al. [8] analyzing the use of antifungal drugs in patients with _Lichtheimia spp. noted that combined antifungal therapy was used in 20% of patients. Surgical methods were used in 43-63% [8, 11]. Our patient was treated with amphotericin B deoxycholate 2 days, followed by amphotericin B lipid complex at a dose of 3 mg/kg/day. We used surgical rehabilitation in 72% of patients with Lichtheimia mucormycosis.
Survival rate of patients with Lichtheimia mucormycosis remains low. According to the results of the analysis of our register, the 12 weeks overall survival rate of patients with Lichtheimia mucormycosis was 44%. The first case of rhinocerebral mucormycosis caused by Lichtheimia ornata, described by Pan J, et al. [8] in 2020, was also fatal. Guinea J, et al. [11] reported surviving of 50% of patients.
The presented clinical case, results of the register analysis as well as the analysis of our register and published materials, demonstrates that Lichtheimia ornata causes severe mucormycosis, often with dissemination, and high mortality.
Conclusions
- Main underlying conditions for Lichtheimia mucormycosis were hematological malignancies (83%)
- Main risk factor was prolonged (median – 47 days) severe neutropenia (72%), steroids were used relatively rarely (55%).
- Lichtheimia mucormycosis was severe disease with ≥ 2 organs involvement in 66% patients
- Сombination therapy (lipid amphotericin B with echinocandins) and surgical treatment were often used for the treatment of Lichtheimia mucormycosis.
- 12 weeks overall survival rate of patients with Lichtheimia mucormycosis was 44%.
Conflicts of Interest
The authors declare no conflict of interest.
References
-
Klimko N, Kozlova Y, Khostelidi S, Shadrivova O, Borzova Y, et al. (2015) The burden of serious fungal diseases in Russia. Mycoses 58(S5): 58-62.
-
Skiada A, Lass-Floerl C, Klimko N, Ibrahim A, Roilides E, et al. (2018) Challenges in the diagnosis and treatment of mucormycosis. Med Mycol 56(S1): 93-101.
-
Donnelly JP, Chen SC, Kauffman CA, Steinbach WJ (2020) Revision and Update of the Consensus Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis 71(6): 1367-1376.
-
Lanternier F, Dannaoui E, Morizot G, Elie C, Garcia- Hermoso D, et al. (2012) Global Analysis of Mucormycosis in France: The RetroZygo Study (2005–2007). Clin Infect Dis 54(S1): S35-S43.
-
De Hoog GS, Guarro J, Gene J, Figueras MJ (2016) Atlas of Clinical Fungi. 2nd (Edn.). CABI 8: 1126.
-
Walther G, Wagner L, Kurzai O (2019) Updates on the Taxonomy of Mucorales with an Emphasis on Clinically Important Taxa. J Fungi 5(4): 106.
-
Cornely OA, Alastruey-Izquierdo A, Arenz D, Chen SCA, Dannaoui E, et al. (2019) Global guideline for the diagnosis and management of mucormycosis: An initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect Dis 19(12): e405-e421.
-
Pan J, Tsui C, Li M, Xiao K, De Hong GS, et al. (2020) First Case of Rhinocerebral Mucormycosis Caused by Lichtheimia ornata, with a Review of Lichtheimia Infections. Mycopathologia 185(3): 555-567.
-
Schwartze VU, Ilse DJ (2014) Jacobsen Mucormycoses caused by Lichtheimia species. Mycoses 57(S3): 73-78.
-
Zoi Dorothea Pana, Danila Seidel, Anna Skiada, Andreas HG, Georgios Petrikkos, et al. (2016) Invasive mucormycosis in children: an epidemiologic study in European and non-European countries based on two registries. BMC Infect Dis 16(1): 667.
-
Jesús Guinea, Pilar Escribano, Antonio Vena, Patricia Muñoz, Del Martínez-Jiménez MC, et al. (2017) Increasing incidence of mucormycosis in a large Spanish hospital from 2007 to 2015: Epidemiology and microbiological characterization of the isolates. PLoS One 12(6): e0179136.
-
Jeong W, Keighley C, Wolfe R, Lee WL, Slavin MA, et al. (2019) The epidemiology and clinical manifestations of mucormycosis: a systematic review and meta-analysis of case reports. Clin Microbiol Infect 25(1): 26-34.
-
Guindon S, Dufayard JF, Lefort V, Anisimova M, Hordijk W, et al. (2010) New Algorithms and Methods to Estimate Maximum-Likelihood Phylogenies: Assessing the Performance of PhyML 3.0. Systematic Biology 59(3): 307-321.
-
Gouy M, Guindon S, Gascuel O (2010) SeaView version 4 : a multiplatform graphical user interface for sequence alignment and phylogenetic tree building. Molecular Biology and Evolution 27(2): 221-224.
- Diversity of Candida sp and Antifungal Susceptibility Patterns in Digestive Candidiasis among People Living with HIV in CHU of Libreville, Gabon
- Vulvovaginal candidiasis: Retrospective study (2019- 2021) at the Centre Hospitalier National de Pikine, Suburban Dakar, Senegal
- Identification of Environmental Fungal Species in Clinical Services of University Hospital of Angre, Abidjan (Cote d’Ivoire)
- New Location of some Gasteroid Basidiomycetes in Western Kazakhstan
- Evaluation of Various Extracellular Enzymes of Ectomycorrhizal Mushrooms
- Morphology and Phylogeny of Lactarius Wallichianae sp. nov and Xerula magnispora sp. nov. from India