Visual Function after Implantation of Multifocal Lens ACUNEX® VARIOMAX, Positioned in Two Variants, According to the Axis of Angle Kappa
ACUNEX® VARIOMAX, an asymmetric multifocal lens was positioned in the eye in two extreme positions, adequately to the axis of angle kappa. This positioning was to answer the question whether the asymmetry of the lens structure in combination with the asymmetry of the position and the size of the pupil will have an impact on the obtained visual acuity to far and near distances. In the first variant, the part of the lens responsible for vision to far distances was more exposed in the pupil, while in the second - the part responsible for vision to near distances was positioned in this way. Taking into account the size of angle kappa, not exceeding the value of 0.640 mm, moderate, statistically significant correlations were found between the size of the pupil and the visual acuity to near distances in one position and to far distances in the other position. There were no statistically significant differences in the obtained values of visual acuity for both studied groups.
Introduction
ACUNEX® VARIOMAX (Teleon Surgical®) is a one- piece, aspherical intraocular lens with a complex structure. The spherical version available on the market for over 3 years continues the success of the Mplus® intraocular lens manufactured by Oculentis® [1, 2]. Their common feature is the asymmetric structure, which distinguishes these models from other premium class lenses with a concentric structure. Another common feature of the Oculentis® and Teleon® models is an addition to near distances at the level of +3.0 Dsph. What makes them different is the material from which they were made. ACUNEX VarioMax is made of a hydrophobic material which, importantly, is glistening free. The hydrophobic structure additionally reduces the risk of posterior capsular opacification. Another difference is the use of the Extended Depth of Focus (EDOF) technology in the Acunex model, which has a positive effect on improving the quality of vision. With the change of the lens material, its structure has changed from a rectangular platform (Mplus) to a typical structure with two haptics (Figures 1a & 1b).
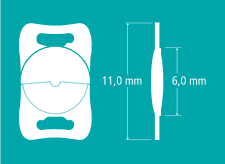
Figure 1a: (left) Mplus® (Oculentis®).
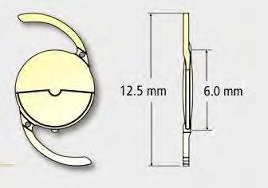
Figure 1b: (left) ACUNEX® VarioMax (Teleon Surgical®). Both lenses have an asymmetrical structure, but differ from each other, i.e. the structure of the main platform.
When thinking about the structure of an asymmetric lens, we often imagine its functioning similar to that of progressive glasses, which is obviously wrong. Regardless of the position of the lens in the eye, the function of vision to far and near distances as well as intermediate distances be preserved [3].
Taking into account the criteria aimed at selecting the appropriate model of the intraocular lens, the examination of the size of angle kappa is already a qualifying standard. Its value affects vision, as does the pupil size in the case of EDOF lenses [4, 5, 6].The greater the angle kappa, the greater the pupil decentration relative to the optical axis.
Below the result of the examination performed using the iTrace analyser shows an example of the eye with a very large angle kappa of 1.41 mm, which indicates a huge decentration of the pupil in relation to the visual axis (Figure 2).
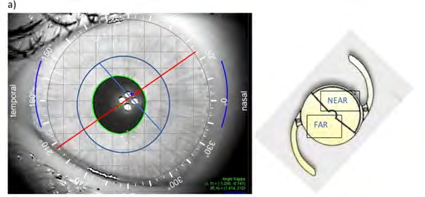
In the above case, if a decision is made to implant a complex intraocular lens, the risk of significant disturbances in visual acuity and the quality of vision should be considered. By positioning the lens with an asymmetric structure according to the axis of angle kappa, where the part responsible for vision to far distances would be positioned “towards the pupil”, there is a probability that the eye will “see” mainly through the part responsible for vision to far distances, which will increase in the case of a narrow pupil (Figure 3a), so vision to near distances may be deteriorated. In the reverse positioning of the lens, i.e. with the part responsible for vision to far distances positioned “away from the pupil”, vision to near distances would be better, which could be further improved by the physiological reflex to reduce the pupil size when focusing the eyesight on nearby objects (Figure 3b).
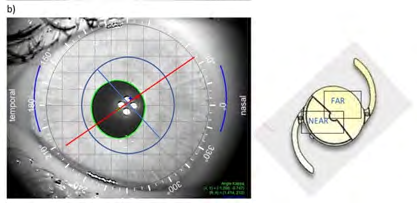
Figure 3a: Lens positioning variant-part responsible for vision to far distances positioned in the lower part
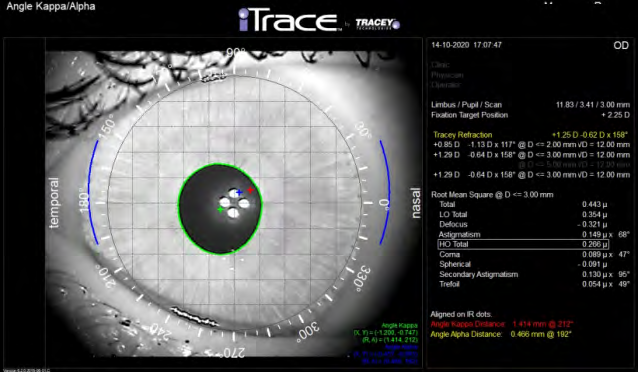
Figure 3b: Lens positioning variant-part responsible for vision to far distances positioned in the upper part. Figure 3: Diagram showing the probable position of the Acunx Vario Max lens relative to the pupil in two options in the image obtained from the iTrace analyser. A high value of angle kappa translates into significant decentration of the pupil centre (green cross in the centre of the pupil) in relation to the visual axis (Red Cross). The red line shows the axis of the intraocular lens (the yellow model next to it) and the blue line in the projection divides the lens into parts responsible for vision to far and near distances.
Considering the qualification criteria, intraocular lenses with a complex structure with the angle kappa values above 0.6mm are practically not implanted. The exception may be lenses with the EDOF structure. In the case of such a large angle kappa as in the above example (value=1.44mm), the implantation of any complex lens could be considered a mistake [7].
Standard implantation of Mplus and Acunex lenses assumes that the part responsible for vision to far distances is in the upper part, and thus its lower part is responsible for vision to near distances (Figure 4).
Considering the already described experience with Mplus lens implantation, in some cases of disturbances in the quality of vision, it was recommended to rotate the lens along the axis to another position, which often resulted in the resolution of unfavorable symptoms [8]. So, to what extent does angle kappa, i.e. its size and the position of the lens in the eye, affect visual acuity and the subjective assessment of the quality of vision? What about pupil size and its effect on vision?
Objective
An assessment of visual acuity to far and near distances as well as the quality of vision in the eyes after implantation of the Acunex Vario Max lens. The lens in the eye was positioned in two variants as presented in the introduction to this article, considering the axis of angle kappa (Figures 3a & 3b). This method of implantation theoretically may have an impact on the obtained values of visual acuity to far and near distances, especially in the case of higher values of angle kappa [9].
Material and Methods
48 patients, 74 eyes were included into the group. After patient’s lens removal, Acunex VARIOMAX, spherical model of intraocular lens was positioned in the eye in two variants, following the angle kappa. The size of angle kappa was assessed preoperatively and postoperatively using the iTrace analyser, a module that also allows for the assessment of the size and position of angle alpha. Visual function achieved pre and postoperatively in the two groups were analysed.
Results
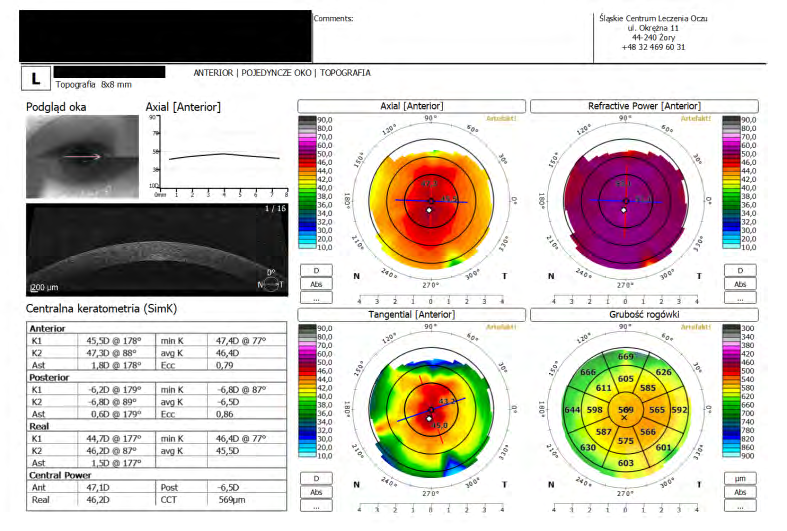
The analysed group included patients in whom, after the removal of the natural lens due to the presence of cataracts or RLE, the artificial lens was implanted directly into the capsule. In each case, a spherical lens was implanted in the eyes, where the value of total corneal astigmatism did not exceed 0.75 Dcyl. In the case of corneal astigmatism, the value of which was higher and amounted between 1.0 to 1.25 Dcyl, an examination was performed with the use of the OCT device, the REVO model (Optopol), aimed at assessing the scope of the actual corneal astigmatism (Figure 5).
In five cases where the value of total corneal astigmatism ranged from 1.25 to 1.75 Dcyl, during the procedure, additional corneal relaxing incisions were performed to reduce astigmatism. The patients were divided into two groups. The division criterion was the position of the lens in relation to the axis of angle kappa.
Group 1: The part responsible for vision to far distances was positioned “towards the pupil”, most often in the lower part of the eye (Figure 3a). It can be assumed that in this position, visual acuity to far distances may be better than in the position of the lens in position 3b. Group 2: The part responsible for vision to near distances was positioned “towards the pupil”, most often in the lower part of the eye (Figure 3b). It can be assumed that visual acuity to near distances may be better in favour of reduced visual acuity to far distances, especially in the case of a narrow pupil.
An example of postoperative positioning of the lens in relation to the axis of angle kappa is shown in (Figure 6).
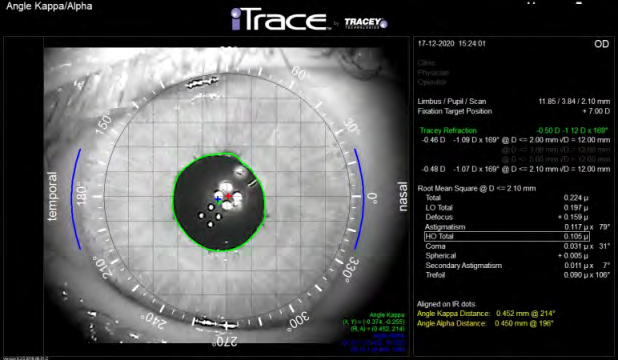
Figure 6: A result of examination using the iTrace analyser, Angle Kappa/Alpha module. Condition after implantation of the lens, positioned in accordance with the axis of angle kappa (±214°), the part responsible for vision to far distances positioned “towards the pupil”, i.e. in group 1. Reflections of light from the lens are visible in the pupil projection. The four clear points are the focus of the image on the part responsible for vision to far distances. The four blurry points are the part responsible for vision to near distances.
A comparative assessment of visual acuity to far and near distances was performed in both groups. The relationship between visual acuity and the size of angle kappa was also analysed. When developing statistical research, the correlation coefficient was examined, and then it was checked whether this coefficient was statistically significant.
Statistical data, including the patient’s age, the number of eyes treated, preoperative values of angles kappa and alpha, the number of cataract surgery and RLE procedures performed are presented in Table 1.
| Values (range) | |
|---|---|
| Age (years) | 63 (28 -83) |
| Number of patients/eyes | 48/74 |
| Preoperative myopia (eyes) | 29 |
| Preoperative hyperopia (eyes) | 34 |
| Cataracts (eyes) | 45 |
| RLE (eyes) | 29 |
| Kappa angle (mm) | 0.358 (0.124-0.644) |
| Alpha angle (mm) | 0.422 (0.072-0.736) |
Table 2: Statistical data of the values obtained from examining group, including age, the number of eyes treated, preoperative va
Visual Acuity
The mean values obtained in both groups, to far (logMar) and near (Snellen) distances, tested before the procedure and two months after the procedure, are presented in Table 2.
| Visual Acuity to Far/Near Distances | Before Surgery | After Surgery |
|---|---|---|
| To far (logMar) | ||
| Group 1 | 0.28 | 0.11 |
| Group 2 | 0.28 | 0.13 |
| To near (Snellen) | ||
| Group 1 | 0.57 | 0.53 |
| Group 2 | 0.52 | 0.53 |
Table 1: Includes values of visual acuity obtained in the two groups, before and after surgery. A comparative analysis of the obt
Table 2: Includes values of visual acuity obtained in the two groups, before and after surgery. A comparative analysis of the obtained values did not show any statistically significant differences in visual acuity to far and near distances, with one exception. In the patients from group 2, a statistically significant positive correlation was found between the pre- and postoperative visual acuity values.
Visual Acuity vs. Kappa Angle
Two statistically significant correlations were observed in the study group. I. Correlation between pupil size and visual acuity to near distances. The parameters obtained after the procedure were used for comparison. This correlation, moderately negative, was found in patients in group 1. Increasing the pupil size after the procedure had a moderate effect on the decrease in postoperative visual acuity to near distances, which is synonymous with an improvement in vision. With a significance level of 0.05, there are grounds to reject the hypothesis that the correlation coefficient between the variables is statistically insignificant. II. Correlation found in group 2 between postoperative visual acuity to far distances and the size of angle kappa obtained before the procedure. The correlation is moderately negative as well. This means that higher values of kappa angle had a slight effect on the decrease in the logMar value of vision to far distances after the procedure, and thus the improvement of vision to far distances after the procedure. With a significance level of 0.05, there are grounds to reject the hypothesis that the correlation coefficient between the variables is statistically insignificant.
Subjective Assessment of Vision
A month after the procedure, the patients from both groups was asked a question about their quality of vision. Young people aged 40-50 reported the presence of disturbances in the quality of vision in scotopic conditions in the form of blurring of the image at light sources more often than older people, but the predominance of these symptoms was not found in any of the groups. What is characteristic is the “deficiency” in the field of visual acuity to near distances reported by people who had myopia before the procedure, and the defect was greater than 3 dioptres. However, it is a characteristic symptom that is found in all people with moderate and severe myopia, regardless of the type and structure of the premium class lens. From the experience of the author of this article, people aged 40+ more often pay attention to any imperfections in the field of vision than older people and this is not related to the size of the preoperative defect or the structure of the lens, but most likely to the high quality of contrast vision. However, there were cases when it was decided to change the position of the lens in relation to its initial position.
Example 1: Male, 49 years old. Diagnosis. Low degree of preoperative hyperopia, presbyopia of both eyes. The patient decided to undergo the procedure because he wanted to get rid of glasses used for vision to near distances (CLE procedure). BCVA with correction to far distances: right eye (RE) with correction (cc) + 1.5Dsph=log -0.1fere, left eye (LE) cc +2.0 Dsph=log 0.0. BCVA to near distances, both eyes=D-0.5 (Snellen). Angle kappa, examined preoperatively, was 0.531 mm, the pupil size, under photopic conditions, was 3.2-3.5 mm. According to the author’s own principle, the procedure was performed first on the non-dominant eye, in this case the left eye. The Acunex VarioMax lens was positioned as shown in Figure 3b. The lens was thus positioned more towards the part responsible for vision to near distances. After the procedure, the patient obtained satisfactory vision to near distances=D-0.5, however he stated that vision to far distances (logMar=0.1) is blurred and too weak. Due to the above, the position of the lens was changed by 180 degrees, which resulted in a significant subjective and a slight objective improvement in vision to far distances (log0.0fere). Unfortunately, the patient reported that his visual acuity to near distances deteriorated, reaching a value of D-0.75 (Snellen).
Discussion
When analysing the obtained results, it must be stated that the positioning of the asymmetric lens, along the axis of angle kappa, in its extreme positions may have a slight but significant effect on postoperative visual acuity. Both the size of the angle and of the pupil are components that can contribute to changes in visual acuity. In the case of positioning an asymmetric lens in the variant as shown in (Figure 3a), the part responsible for vision to far distances is more “exposed” in the pupil, so in eyes with a large angle and, additionally, a narrow pupil, with good vision to far distances, we can expect worse values of vision to near distances. An examination performed in this group showed that vision to near distances improved in the case of patients with a wider pupil, which seems logical. The wider the pupil, the more light is likely to pass through the part of the lens responsible for vision to near distances. When the lens is positioned in the other extreme position, the part responsible for vision to near distances is more exposed in the pupil. In the case of a larger angle kappa, better values of vision to far distances were obtained (lower logMar values). It is difficult to explain this mild, however statistically significant, correlation.
Taking into account the above results, we must agree with the lens Manufacturer that the standard position of the lens with an asymmetric structure is optimal in most cases, i.e. the upper part is dedicated to far distances and the lower part to near distances. In these positions, there is no set preference for either distance (Figure 4).
The values of angle kappa in the study group ranged from 0.124 to 0.644. This maximum value significantly exceeded the safe value of 0.500-0.550, which is considered insurmountable if you wish to avoid postoperative loss of visual acuity and quality of vision. Knowing the preoperative values of angle kappa, pupil size and the position of the asymmetric lens in the eye, we can imagine which of these elements and how may affect postoperative vision. In the presence of cataracts, it should be remembered that postoperatively, the pupil size may decrease. In the study group, changes in the pupil size were insignificant (Table 3).
| Pupil Size [mm] | Before Surgery | After Surgery | Difference |
|---|---|---|---|
| min | 2.1 | 2 | 0.1 |
| max | 6.5 | 6.3 | 0.2 |
| mean | 4.3 | 3.8 | 0.5 |
Table 3: Values of the pupil size in the study group, assessed before and two months after the procedure.
Taking into account the postoperative expectations of patients, who are hyperopic before the procedure (preserving or improving vision to far distances and “regaining” vision to near distances) and myopic (preserving vision to near distances and “regaining” vision to far distances), in case of patient dissatisfaction as to the quality of postoperative vision, knowing the above dependencies between the structure of the eye and the structure of the lens, there is a chance that changing the position of the lens in the eye can improve both visual acuity and quality of vision. For example, in the case of a patient with high preoperative myopia and high angle kappa, if vision to near distances is very unsatisfactory and the lens has been set in the standard (upper part-far distances, lower part-near distances) position in the eye, its position in the eye can be changed, as shown in Figure 3b which should improve vision to near distances. Conversely, in the case of a preoperatively hyperopic patient, if his/her vision to far distances is not satisfactory and the lens was inserted in the standard position, it can be positioned as shown in Figure 3a, which may improve vision to far distances. In both cases, however, one should remember about the pupil size and the influence of angle alpha on vision.
Conclusions
Postoperative positioning of the asymmetric Acunex VarioMax multifocal spherical lens may have an impact on the obtained values of visual acuity to far and near distances if the lens is positioned in the eye along the axis of angle kappa. In this position, additionally in the case of large values of angle kappa, visual acuity may slightly change. It should be borne in mind when the standard positioning of this lens, i.e. in the upper part (far distances) - lower part (near distances), recommended by the Manufacturer, does not meet the patient’s expectations. Taking into account the asymmetry in the structure of this lens model, additional asymmetry in the position of the pupil, i.e. the size of angle kappa, may be a factor adversely affecting visual acuity and quality of vision.
References
-
Cywinski A, Penter S, Bednarski L, Ferda-Lewinska D, Gacek M (2019) Mplus/Mplus Toric (Oculentis) Bifocal Successor of Monofocal Lens in Private Medical Centre. Six Years of Experience. Archives of Ophthalmology and Optometry 2(1): 8-15.
-
Venter JA, Pelouskova M, Collins BM, Schallhorn SC, Hannan SJ (2013) Visual outcomes and patient satisfaction in 9366 eyes using a refractive segmented multifocal intraocular lens. J Cataract Refract Surg 39(10): 1477-1484.
-
Song IS, Yoon SY, Kim JY, Kim MJ, Tchah H (2016) Influence of Near-Segment Positioning in a Rotationally Asymmetric Multifocal Intraocular Lens. J Refract Surg 32(4): 238-243.
-
Fu Y, Kou J, Chen D, Wang D, Zhao Y, et al. (2019) Influence of angle kappa and angle alpha on visual quality after implantation of multifocal intraocular lenses. J Cataract Refract Surg 45(9): 1258-1264.
-
A Cywinski (2021) The Influence of Angles Kappa and Alpha and Pupil Size on Vision after Implantation of Soleko Evolve and Lucidis Lenses with a “Pure” EDOF Structure. Journal of Ophthalmology and Advance Research 2(2): 1-12.
-
Spadea L, Giannico MI, Formisano M, Alisi L (2021) Visual Performances of a New Extended Depth-of-Focus Intraocular Lens with a Refractive Design: A Prospective Study After Bilateral Implantation. Ther Clin Risk Manag 17: 727-738.
-
Moshirfar M, Hoggan RN, Muthappan V (2013) Angle Kappa and its importance in refractive surgery. Oman journal of ophthalmology 6(3): 151-158.
-
Pazo EE, Richoz O, McNeely R, Millar ZA, Moore TC, et al. (2016) Optimized Visual Outcome After Asymmetrical Multifocal IOL Rotation. J Refract Surg 32(7): 494-496.
-
Qin M, Ji M, Zhou T, Yaun Y, Luo J, et al. (2022) Influence of angle alpha on visual quality after implantation of extended depth of focus intraocular lenses. BMC Ophthalmol 22(1): 82.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report