Novel Technique of 23G Pars Planar Vitrectomy (TPPV) with Alcon Centurion Silver System Gravity -FMS (ACenSS) and ACenSS Vitrectomy Probe (23G) with an External Light Source in Teaching Hospital Rathnapura Sri Lanka
Dual pneumatic 23G vitrectomy cutters of both Alcon Constellation Vision System (AConsVS) and ACenSS have cut rates of 5000 cpm. Aims: To report a novel technique of using ACenSS 23G Vitrectomy cutter for trocar surgery with an external light source in Teaching hospital Rathnapura Sri Lanka from 01/03/2022 to 30/09/2022. Methods: 23G Alcon light probes were used with Retikare (ICON Medicare Tamil Nadu India) external light source for endoillumination. Infusion pressure was set at 65cmH2O (47.81 mmHg) and infusion line connected to eye through a 3 ways tap. ACenSS-GFMS aspiration line connected to aspiration line of vitrectomy probe. Cryopexy used to seal retinal tears as no endolaser facility. Volk surgical corneal lenses with Zeiss Lumera I microscope provided the viewing. ACenSS foot pedal was programmed to 3 modes of vitrectomy with navigation, cutter on/ off function and on/pause of continuous irrigation. A gravity driven another infusion line is used to keep the infusion when endo diathermy is used. Results: When working on maximum cut rate of the ACenSS GFMS (5000 cpm) for long duration machine automatically stops and a restart with reprime needed. Therefore, cut rates were set at a lower rate to work without interruption (core vitrectomy- 2000 cpm, peripheral trim- 3000cpm and for epinucleus removal 4000 cpm). No retinal traction or ridging of retina was observed at peripheral trim. Total of 210 TPPVs were performed with this technique. Conclusions: 23G TPPV with ACenSS using an external light source is a simple, safe and a cost-effective technique with equal outcome to AConsVS.
Introduction
At present Sri Lanka has 15 board certified Vitreo- Retinal surgeons and another 3 general ophthalmologists who can work as Vitreo-Retinal surgeons, summing up to 18 for the whole island. There are 20 Vitrectomy machines for a population of 22.15 million [1, 2]. Out of these 14 machines in the government sector hospitals and 6 in the private sector hospitals or in private ownership. Western province, the administrative centre (Area 3684km2) of Sri Lanka alone has 12 vitrectomy machines (7 in government sector hospitals and 5 in private hospitals) for 6.2 million population (one machine per 0.516 million population in Western province [1]. Therefore, only 8 vitrectomy machines to serve rest of the people in the country (one machine per 2.05 million population). Apart from that Northern, Eastern, Sabaragamuwa and Uva provinces of Sri Lanka do not have a vitrectomy machine at least to give the vitreoretinal service. Vitreoretinal services are considered low priority in peripheral tertiary care multidisciplinary hospitals due to pressing demand for more life or organ saving specialties and to treat common eye conditions like cataract, refractive errors, traumatic eye injuries and paediatric eye problems. Therefore, getting facilities for provision of vitreo-retinal services to preserve vision in eye diseases like proliferative diabetic eye disease, retinal detachments, traumatic eye injuries, recovery of vision in complicated cataract operations and cases of endophthalmitis is a difficult task for the vitreoretinal surgeon working in a peripheral tertiary care hospital of Sri Lanka. On the other hand, with the ongoing economic crisis of the country ministry of health cannot afford costly equipment and consumables for vitreoretinal surgery. Therefore, the authors were compelled to find out an alternative technique with available resources to provide vitreoretinal service in preventing blindness in Sabaragamuwa Province (Population -1.9 million area- 4968km2) [1, 2], the draining area to the teaching hospital Rathnapura. Only available vitrectomy facility in teaching hospital Rathnapura Sri Lanka is the Alcon Centurion Silver System with supply of limited consumables through the hospital. Alcon Centurion Silver system’s (ACenSS) 23G vitrectomy probe is very similar to Alcon Constellation vision system (AConsVS) 23G vitrectomy probe in mechanics (dual pneumatic drive technology where air controls the cutter open and close timing) except the former has a rounded edge than the bevelled edge configuration of latter.
Both have the cut rate of 5000 cuts per minute (cpm) [3]. Even though the Alcon Centurion Siler System 23G Vitrectomy probe has used for either anterior vitrectomy and very limited pars planar approach anterior vitrectomy in the literature, author believes that it has not been used before for full scale TPPV for retinal detachment repairs, macula hole repairs, membrane dissection in diabetic vitrectomy, Fragmentation, TPPV for recovery of vision in complicated cataract operation and TPPV in traumatic eye injuries with intraocular foreign bodies in the published literature Sachdev MS, et al. [4, 5, 6, 7]. The aim of this study is to report the novel technique of using Alcon Centurion silver system machine and its 23G vitrectomy probe for full scale 23G trocar surgery in treating complex vitreoretinal disease and to report practical problems encountered and solutions to overcome the problems. Main advantages of Alcon Centurion silver system and its fluid management system (Gravity FMS) over Alcon Constellation vision system are cheaper, cost effective, no central lines or cylinders of compressed air needed for its operation (this is due to in built diaphragm pump vacuum system drives ACenSS 23G vitrectomy cutter blade whereas Venturi aspiration pump system with an external air source drives AConsVS 23G vitrectomy cutter blade) [3, 8], ability to do phacoemulsification and sleeveless phacoemulsification of dropped lens pieces or whole lens in the absence of a fragmatome at the same time and easy handling.
Key Messages
This technique highlights the provision of vitreoretinal service with available resources in the prevention of blindness. Author believes this is the first time in the world that Alcon Centurion Silver System GFMS 23G Vitrectomy cutter is used for full scale trocar surgery with an external light source for endoillumination.
Method
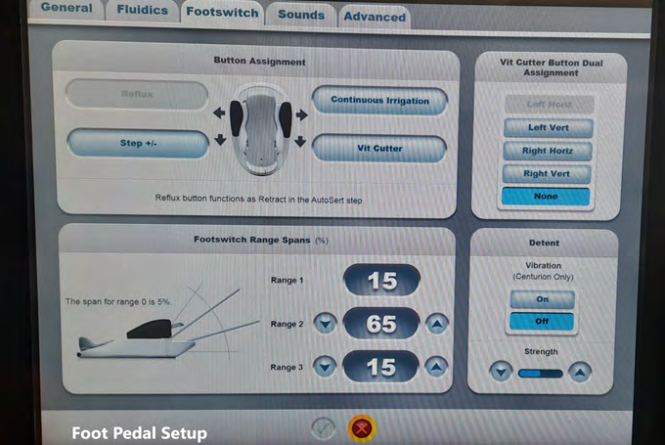
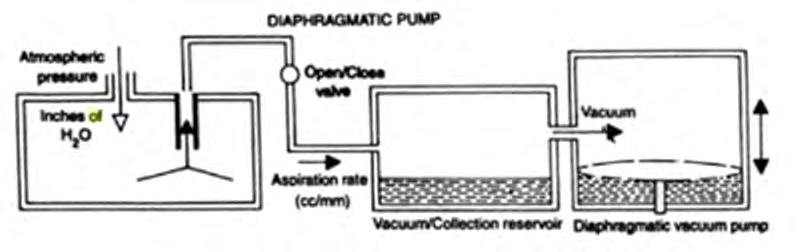
Observational study of using Alcon Centurion Silver system (ACenSS) Gravity Fluid management System (GFMS) 23G vitrectomy probe for full scale pars planar vitrectomy surgery in Teaching Hospital Rathnapura Sri Lanka from 01.03.2022 to 30.09.2022. All the cases underwent 23G pars planar vitrectomy with Alcon Centurion Silver system’s 23G vitrectomy cutter from 01.03.2022 to 30.09.2022 included in this study (6 month period) (Figure 1). Privately owned Retikare vitrectomy machine (ICON Medicare Tamil Nādu India) of a colleague Ophthalmologist of Teaching hospital Rathnapura was used as the external light source for 23G endo-illumination and for air-fluid exchange and 1000cst Silicone oil insertion /removal when needed. 23G Alcon light probes were used with Retikare external light source (white LED Illumination). 23G Alcon trocars used as entry ports in the pars planar area for pars planar vitrectomy (TPPV). Sensor controlled (both infusion and aspiration pressures are controlled by 2 sensors in the cassette) infusion line (Figure 2) of Alcon Centurion Silver system Gravity Fluid Management System (ACenGFMS) is connected to inferotemporal port through a 23G exhaust probe and a tube line with a 3 way tap to eye (Figure 2). ACenGFMS aspiration line (Figure 2) is connected to vitrectomy probe’s aspiration line. 23G dual pneumatic Alcon Centurion vitrectomy cutter is used for vitrectomy (TPPV). Foot pedal was programmed with cutter on /off position, continue/ pause irrigation and separate vitrectomy modes for core vitrectomy, peripheral vitreous trim, and cortex aspiration with backward/forward navigation (Figure 3). As there is no endolaser facility primary sealing of retinal tears were achieved with cryopexy. Volk direct surgical vitrectomy corneal stick-on lenses were used for posterior segment viewing during TPPV in the absence of a wide-angle viewing system. Zeiss Lumera I microscope was used for all the vitrectomies. As soon as the port confirmation was done with direct visualization through microscope infusion was switched on to continuous mode to maintain the pressure within the eye (Figure 3). When using 23G Endo diathermy facility in the ACenSS machine as soon as the assistant manually changed the settings to diathermy and as a result continuous irrigation turns off and it was overcome by connecting another gravity driven fluid line to the 3 ways tap of the infusion line to keep the pressure in the eye during endo-diathermy. All the surgical consumables were reused several times after thorough cleaning and dry up for 24 hours and plasma sterilization due to the very poor financial situation of the Teaching hospital Rathnapura Sri Lanka with the present economic crisis. All the cases operated followed up day one post-op, one-week post-op, one-month post-op and at 3 months post-op during the last 6 months. In addition, they were seen early or re-operated at any time when the need arose.
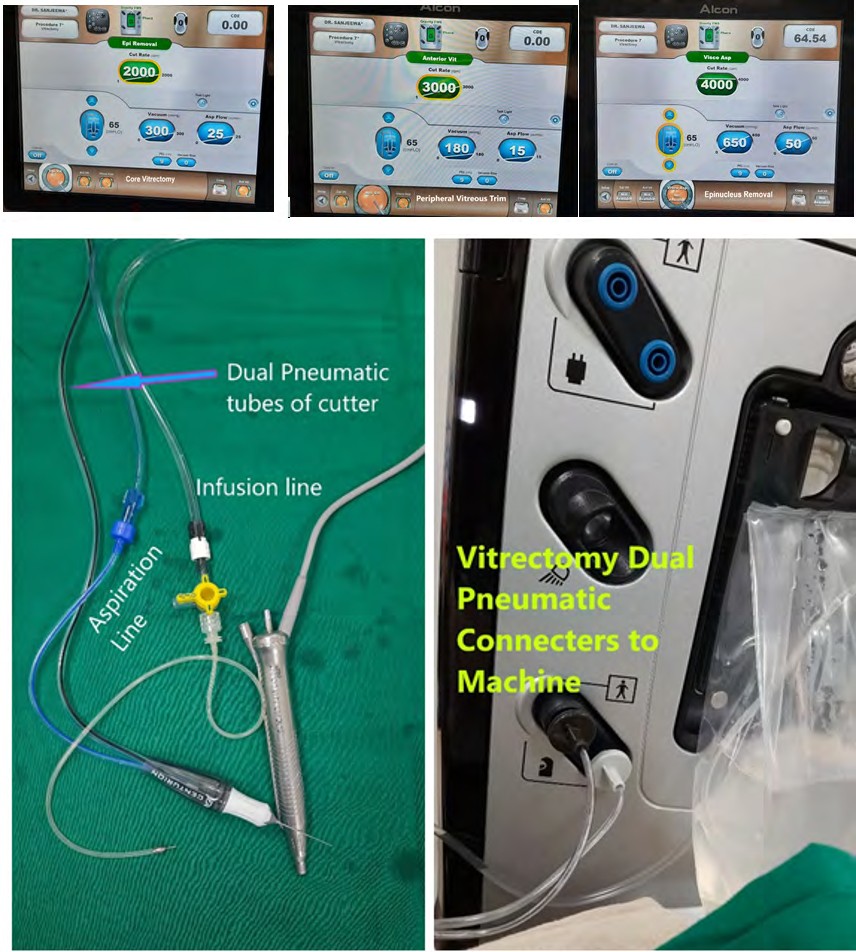
Figure 1A, B, C: Different vitrectomy modes in Alcon Centurion Silver System 23G Vitrectomy machine. A-core vitrectomy, B- Peripheral vitreous trim, C- epinucleus removal.
Results
Infusion pressure was set at 65cmH2O (47.81mmHg, Figure 1) [9] and continuous irrigation on pressing to the side of top right-hand toe switch in foot pedal (Figure 3). There was not any collapse of the globe during vitrectomy (both core vitrectomy and peripheral vitreous trim with indentation) with continuous infusion and the stable IOP maintenance was observed throughout.
Vitrectomy Cutter Settings
For core vitrectomy cut rate 2000 cpm, vacuum 300mmHg and aspiration 20cc/min was set (Figure 1A). For peripheral vitreous trim cut rate at 3000mmHg, vacuum at 180 mmHg and aspiration 15cc/min was set (Figure 1B). Third setting was set for epinucleus or cortical matter removal with a cut rate 4000 cpm, vacuum 650mmHg and aspiration 50 cc/min (Figure 1C). Foot pedal toe switches were programmed as in the Figure 3. Even though the machine’s maximum cutter speed is 5000cpm, with long vitrectomies the cutter function was automatically disabled, and the Alcon Centurion FMS needed reprime after a shut down and restart. Therefore, cut rate was optimized to 2000 cpm and 3000cpm to work longer without any interruption. Various procedures (Pars planar vitrectomies) done with this technique from 01.03.2022 to 30.09.2022 is shown below (Table 1). Authors observed no complications during the surgery like choroidal haemorrhages, globe collapse, inadvertent retinal damage, or post-operative retinal detachments in any of these cases. Even during peripheral vitreous trim with indentation no traction or ridging on the retina was observed. There are 3-foot pedal ranges (Figure 3) where cutting and fluidic dynamics are linearly increased to the set maximum which provided very safe parameters working close to the retina. Total of 210 pars planar vitrectomies (23G) has been performed with this technique from 01.03.2022 to 30.09.2022 (6-month period). There are 40 pars planar vitrectomies performed for complex rhegmatogenous retinal detachment repairs where a success rate of 87.5% (35 out of 40 cases) could be achieved (Table 1).
| Surgery | Number and success |
| TPPV for Retinal Detachments (Complex RD) | 40 Success rate 35/40 (87.5%) |
| TPPV for Vitreoretinal interphase disorders Macula holes, Vitreomacular traction, Epiretinal membrane removals | 14 |
| Diabetic Vitrectomy | 27 |
| TPPV for VH removal | 31 |
| TPPV for traumatic eye injuries involving the posterior segment | 3 |
| TPPV and IOL scleral Tuck | 44 |
| TPPV and lens matter removal | 12 |
| TPPV for Endophthalmitis | 3 |
| TPPV for miscellaneous causes | 36 |
| Phacoemulsification and IOL | 283 |
| Total TPPV | 210 |
Table 1: 23G Pars Planar Vitrectomies (TPPV) performed with Alcon Centurion Silver System with an external light source in Teachi
Discussion
Dual pneumatic (bi-directional pulsed air) vitrectomy cutter blade drive mechanism, high cut rate (5000cpm) and 23G instrumentation of both Alcon Centurion Silver System (ACenSS GFMS) and Alcon Constellation Vision System (AConsVS) machines prompted the authors to use former’s vitrectomy cutter for full scale 23G trocar surgery (pars planar vitrectomy) irrespective of the pump systems for fluidic mechanisms [10, 11, 12]. ACenSS GFMS has a dual segment peristaltic aspiration pump system with an inbuilt diaphragm pump for bidirectional pulsed air propelling the cutter blade while AConsVS has a Venturi aspiration pump system where the flow is induced by vacuum generated with an external air source which drives the cutter blade through bidirectional pulsed air [12] (Figures 4 & 5).
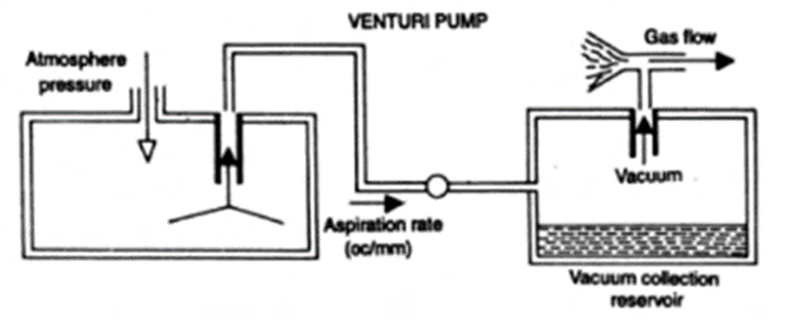
Venturi pump systems were used traditionally in vitrectomy machines due to slow rise times and pulsatile flow in older peristaltic pumps [12]. But however in newest generations of peristaltic pump systems these deficiencies have improved and increasingly used in vitrectomy machines [12] (for example dual segment pump system in ACenSS GFMS compared to Alcon Infinity Vision System single segment pump to mitigate pulsatile flow). In several of newest machines both venturi and peristaltic pump systems have been in cooperated and the surgeon has been given the choice to choose [12]. Therefore, the peristaltic aspiration pump and inbuilt diaphragm pump system in ACenSS GFMS is no inferior to AConsVS Venturi pump and use of former machine for full scale trocar surgery is justifiable both theoretically and technically because it is the only available vitrectomy facility in the centre where the authors work Spandau U, et al. [6, 7, 8, 11, 12, 13, 14, 15].
In small gauge vitrectomies infusion pressure is set at 50mmHg (AConsVS) because vitreous flow rates are higher in small gauge instruments at higher pressures [9, 10, 11, 12]. As the ACenVS GFMS infusion pressure calibration is in cmH2O it was set at 65cmH2O to achieve the target pressure close to 50mmHg (47.81mHg). Main points to consider when going ahead with full scale vitreoretinal surgery with this technique (ACenSS) are
- Stable intraocular pressure maintenance (IOP) in the vitreous cavity,
- Vitrectomy cutter setting optimization for fluidics [11, 12].
- Foot pedal setup to the convenience of the surgeon.
- Identification of problems during the procedures and optimization to the best possible outcome.
The ACenSS GFMS with peristaltic aspiration pump system having 2 sensors each for infusion and aspiration (active fluidics) [14] is meant for stable IOP control in the anterior segment surgeries. Nevertheless, author observed the same stable IOP maintenance in the long duration posterior segment surgeries throughout (TPPV). Vitreous cutter configuration of ACenSS (rounded edge at port) vs AConsVS (bevelled edge at port) has no major drawback to the surgeries performed in a low economic setup. Author has used AConsVS earlier for TPPV and no difference was observed in relation to surgical timing and outcome. When doing peripheral vitreous trim, no traction or ridging in the attached or detached retina was observed with the settings (cut rate 3000cpm, vacuum 180mmHg, aspiration 15cc/min, Figure 1) [11]. Induction of posterior vitreous detachment (PVD) with cutter off is equally comfortable as with the AConsVS machine to the author. Compared to the other vitrectomy machines ACenSS GFMS has 2 sensors each for infusion and aspiration is an added advantage for stable IOP maintenance and to work with high cut rates [9]. This is an easy, simple, cost effective and a safe technique even to a general ophthalmologist with some hands on with vitreoretinal surgery in recovering the cataract complications with dropped pieces of lens to the posterior segment provided the surgeon can get the vitreoretinal instruments, consumables, and an external light source for endo-illumination with no any added burden to the health system. In fact, there are 43 ACenSS machines in government hospitals island wide and there is a huge potential for each machine to be converted to a vitrectomy machine and same general ophthalmologist functioning as the Vitreoretinal surgeon to recover his or her cataract surgery related complications in the process of preserving vision. Therefore, huge burden and waiting lists to a vitreoretinal surgeon can be eased.
Compared to standard Alcon Constellation Vision System both have 23G dual pneumatic cutter blades with 5000 cpm, ability of cutter on/off while infusion is intact, linear function of set vitrectomy and fluidic parameters and stable IOP maintenance throughout. In contrast standard AConsVS has bevelled edge cutter configuration compared to rounded edge cutter configuration in ACenSS, cutter drive mechanism by an external air source and venturi pump for long duration pars planar vitrectomy compared to peristaltic system with inbuilt diaphragm pump for cutter drive in ACenSS, and 3 vitrectomy sub modes (namely 3D vitrectomy, proportional vacuum, and momentary vacuum sub modes) in AConsVS compared to single linear mode in ACenSS (Table 2).
- Alcon Centurion Silver System (ACenSS) for 23G Pars Planar
- Vitrectomy
- Alcon Constellation Vision System (AConsVS) for 23G pars Planar Vitrectomy
- Advantages
- 23G Dual Pneumatic cutter
- 23G Dual Pneumatic cutter
- Stable IOP maintenance
- Stable IOP maintenance
- 23G Endo diathermy facility
- 23G Endo diathermy facility
- Cut rate 5000 cpm
- Cut rate 5000 cpm
- Ability to increase cut rate to 20,000cpm with dual cutting blade in hyper vit modes
- Ability of cutter on/off while intact infusion
- Ability of cutter on/off while intact infusion
- Simple and less surgical timing for machine preparation and priming in each case
- Complex and takes more timing for machine preparation and priming
- Less cost and least burden to system
- Expensive instrumentation and consumables
- Disadvantages
- Rounded edge configuration of cutter
- Bevelled edge configuration of cutter (Advantageous in diabetic dissections to get the line of cleavage)
- Blade drive mechanismIn built Diaphragm pump (machine’s vitrectomy facility stops in long duration vitrectomies and need a restart)
- Venturi aspiration pump powered by an external air source or a compressor (amenable for longer vitrectomy)
- No light source for endoillumination
- In built endoillumination source present
Table 2: Comparison of Alcon Centurion Silver System’s 23G vitrectomy facility (ACenSS) to standard vitrectomy machine (Alcon
Even though the standard machine having above advanced features authors were very comfortable with ACenSS vitrectomy facility with equal safety and outcome in the cases performed during the period of the study. On the other hand, ACenSS vitrectomy facility is very simple and easy handling and less time consuming compared to standard machine.
Conclusion
In developing countries with very low priority for vitreoretinal services and no funding for vitreoretinal service, this technique with available resources would prevent blindness from blinding vitreoretinal disease. On the other hand, 23G TPPV with Alcon Centurion Silver System is a simple, safe, cheap and a cost-effective technique compared to 23G TPPV with Alcon Constellation Vision System machine in a low budget set up with equal outcome and safety.
References
-
The World Bank Group (2022) Population Total -Sri Lank.
-
Department of Census and Statistics Sri Lanka (2021) Statistical Pocket Book.
-
Packo KH (2010) True IOP Control and Infusion Cannula Fluidics with the Constellation® Vision System. Retinal Physician 1: 1-2.
-
Sachdev MS, Gupta A, Gupta H, Sachdev GS, Malik R, et al. (2022) Limited pars-plana vitrectomy for optimizing surgical outcome in subluxated cataracts undergoing femtosecond laser-assisted cataract surgery. Indian J Ophthalmol 70(2): 658–661.
-
Spandau U (2020) Introduction and Possible Indications for Trocar Surgery of Posterior Segment. In: Trocar Surgery for Cataract Surgeons, Springer International Publishing, Cham, pp: 99-103.
-
Spandau U (2020) Setup and Basics about Trocar Surgery. In: Spandau U (Ed.), Trocar Surgery for Cataract Surgeons. Springer, Cham, pp: 19-24.
-
Spandau U, Scharioth GB (2022) Anterior Vitrectomy and Other Surgeries with Trocars from Pars Plana. In: Spandau U, et al. (Eds.), Complications During and After Cataract Surgery. Springer, Cham, pp: 87-107.
-
Villanueva GS, Canton AVM (2012) Experience with modern vitrectomy machines. Retina Today pp: 45-46.
-
Nagpal M, Goswami S (2015) Micro-incision Vitrectomy Surgery- Past, Present and Future. European Ophthalmic Review 9(1): 64-68.
-
Oravecz R, Schrage N, Dutescu RM (2021) Comparison of modern high-speed vitrectomy systems and the advantages of using dual-bladed probes. International Journal of Retina and Vitreous 7(1): 8.
-
Rossi T, Querzoli G, Angelini G, Malvasi C, Iossa M, et al. (2014) Fluid dynamics of vitrectomy probes. Retina 34(3): 558-567.
-
Steel DHW, S Charles (2011) Vitrectomy Fluidics. Ophthalmologica 226(1): S27-S35.
-
Charles S (2014) Fluidics and Cutter Dynamics. In: Oh H, et al. (Eds.), Micro Incision Vitrectomy surgery: Emerging techniques and technology. Karger, Basel, pp: 145.
-
Li H, Chen W, Gao Y, Tianju Ma, Luo Y, et al. (2022) Active-fluidics versus gravity-fluidics system in phacoemulsification for age-related cataract (AGSPC): study protocol for a prospective, randomised, double- blind, controlled clinical trial. BMJ Open 12(1): e059062.
-
Williamson TH (2013) Vitreoretinal Surgery. 2nd (Edn.), Springer, Berlin, Heidelberg, pp: 429.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report