Role of Fine Needle Aspiration Cytology (FNAC) in the Diagnosis of Adult-Onset Retinoblastoma: A Case Report
We report the role of fine needle aspiration cytology (FNAC) for suspected intraocular tumor in the case of a 25 year old man who presented with the chief complaint of a whitish reflex and painless diminution of vision in the right eye for 3 months. Examination revealed a large intraocular mass with overlying retinal detachment. B-scan ultrasonography revealed an intraocular mass with foci of intralesional calcification. Systemic workup was unremarkable. MRI of the brain and orbit ruled out extra ocular spread. Based on clinical suspicion of either amelanotic melanoma or adult-onset retinoblastoma, fine needle aspiration cytology (FNAC) was done which revealed retinoblastoma. The patient underwent primary enucleation of the right eye and histopathological analysis confirmed the diagnosis of retinoblastoma.
Introduction
Retinoblastoma is the most common primary malignant tumor of childhood with more than 90% of the cases diagnosed under the age of 5 years [1]. Although rare, retinoblastoma can present even in adults with most of the cases reported in the past two decades. Adult-onset retinoblastoma often lacks the classical features such as intralesional calcification present in childhood retinoblastoma, which often leads to misdiagnosis and advanced presentations due to delayed diagnosis [2]. Therefore, high clinical suspicion and use of adjunctive investigations are often required while dealing with any atypical intraocular mass lesion in an adult.
A 25 year old man presented with the chief complaint of a whitish reflex and painless diminution of vision in the right eye for 3 months. There was no history of any other systemic complaints, ocular trauma, and no family history of any ocular or systemic malignancy. On examination, he had a visual acuity of perception of light positive with projection of rays inaccurate in all quadrants in his right eye and 20/20 in his left eye. The intraocular pressure was 32 mm Hg and 14 mm Hg in his right and left eyes, respectively. A relative afferent pupillary defect was noted in his right eye. Slit lamp bio microscopy revealed neovascularization of the iris and a greyish-white vascularized intraocular mass filling the vitreous cavity, reaching just behind the posterior capsule of the clear crystalline lens in his right eye (Figure 1A). A dilated fundus examination of the right eye revealed an intraocular mass filling the vitreous cavity with an overlying retinal detachment. Examination of the left eye was unremarkable. B-scan ultrasonography of the right eye showed a mass arising from the retina with variable internal reflectivity and foci of very high amplitude spikes suggestive of intralesional calcification (Figure 1B).
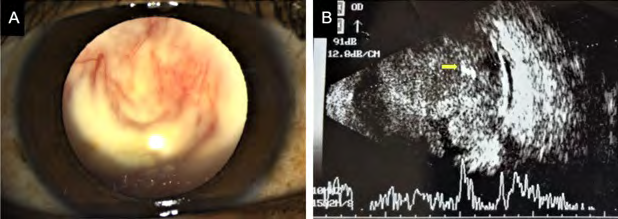
Figure 1: (A) Slit lamp bio microscopy revealed neovascularization of the iris and a greyish-white vascularized intraocular mass filling the vitreous cavity, reaching just behind the posterior capsule of the clear crystalline lens in the right eye. (B) B-scan ultrasonography of the right eye showed a mass arising from the retina with variable internal reflectivity and foci of very high amplitude spikes suggestive of intralesional calcification (marked by arrow).
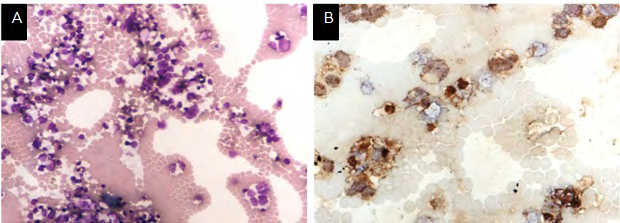
Systemic workup including a complete blood count, liver function tests, renal function tests, ultrasound of the whole abdomen and a chest X-ray was unremarkable. A contrast-enhanced MRI of the brain and orbit showed a heterogeneously enhancing well-defined mass lesion in the right globe with an associated exudative retinal detachment with suspected choroidal and optic nerve infiltration. Visual evoked response, which was done to prognosticate, revealed no significant response in the right eye. Based on the clinical examination and ancillary investigations, a differential diagnosis of amelanotic melanoma and adult-onset retinoblastoma was made. However, neither the age of the patient nor the examination findings or investigations was conclusive for a diagnosis. Therefore, the patient was planned for fine needle aspiration cytology (FNAC) of the intraocular mass to confirm the diagnosis. Under microscopic view, a 24-G needle mounted on a 5 mL syringe was introduced through the pars plane route into the intraocular mass. Carefully controlled aspiration with simultaneous withdrawal of the needle was done and subsequently triple freeze-thaw cryotherapy was applied at the site of scleral entry to decrease the potential risk of tumor seeding. Cytospin® (Shandon, Pittsburgh, PA) smear preparations were made and stained by Papanicolaou (Pap) stain and May Grunwald Giemsa (MGG) stain. These revealed a malignant round cell tumor present singly as well as in small clusters with nuclear moulding which was suggestive of retinoblastoma (Figure 2A). Immuno Histochemical (IHC) staining showed strong cytoplasmic positivity with synaptophysin in the tumor cells (Figure 2B) and no staining with human melanoma black-45 (HMB-45) which was in concordance with our provisional diagnosis of retinoblastoma.
The patient underwent primary enucleation of the right eye and histopathological sections were prepared and stained with Haematoxylin and Eosin stain. These sections confirmed the presence of poorly differentiated retinoblastoma with extensive necrosis in the enucleated eyeball specimen. The tumor was seen to be infiltrating the choroid, iris, ciliary body, inner sclera and entire optic nerve stump including the resected margin of the optic nerve (Figure 3A & 3B). The patient was further referred to medical and radiation oncologist for adjuvant systemic chemotherapy and radiotherapy, respectively.
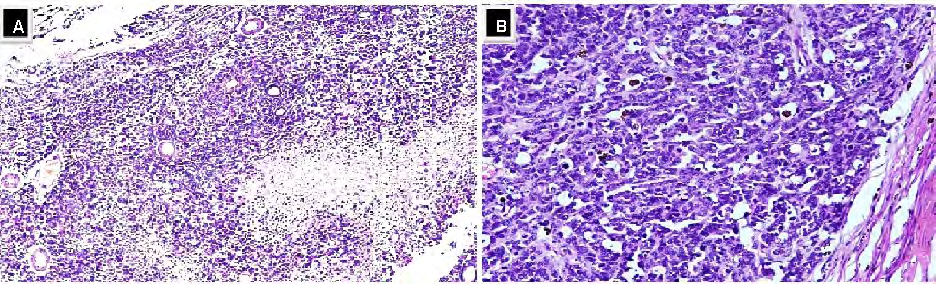
Figure 3: Histopathological sections of the enucleated eyeball stained with Haematoxylin and Eosin; (A) under 10x magnification. (B) Under 20x magnification, showed the presence of poorly differentiated retinoblastoma with extensive necrosis. The tumour was seen to be infiltrating the choroid, iris, ciliary body, inner sclera and entire optic nerve stump including the resected margin of the optic nerve.
Discussion
Adult-onset retinoblastoma is an extremely rare tumor, with only 45 other cases reported in the literature till date [2]. Almost all cases were sporadic, unilateral and aged between 20-74 years with diminution of vision being the predominant complaint and often associated with a visible white, vascularized retinal mass [2]. Possible differential diagnosis of an amelanotic intraocular mass lesion in an adult includes amelanotic melanoma, lymphoma, metastatic carcinoma, astrocytoma, leukemia, panophthalmitis, endophthalmitis, inflammatory diseases of the retina, retinoblastoma and retinocytoma [2]. In addition to being rare, adult retinoblastomas might not present with clinical features typically seen in childhood retinoblastoma such as a leukocoria or a squint [2]. Although our case did show intralesional calcification on ultrasound B-scan, reports have shown that adult retinoblastomas often lack these characteristic calcification changes [2, 3]. These features often lead to a diagnostic dilemma and may warrant adjunctive investigations such as cytopathology in addition to clinical examination and imaging. The use of FNAC for the diagnosis of a variety of suspected intraocular tumors including cases of retinoblastoma has been demonstrated to be a safe and reliable diagnostic method in cases where non-invasive diagnostic modalities have failed to establish a diagnosis [4, 5]. However, it is not routinely done for cases of retinoblastoma as the majority of the diagnosis of childhood retinoblastoma can be made with clinical examination and imaging. Also, there is a theoretical risk of tumor seeding of the needle-track and possible extra ocular dissemination of the tumor cells [6]. Aspiration cytology or vitrectomy samples were successful in revealing features suggestive of retinoblastoma in majority of the reported cases of adult-onset retinoblastoma [2]. Immunohistochemistry (IHC) staining performed on FNAC specimens can help in confirmation of the diagnosis. Retinoblastoma tumors are often strongly positive for neuron specific enolase (NSE) and synaptophysin [2, 7] as seen in our case too. Also, lack of staining with HMB-45 and keratin almost rules out malignant melanoma and metastatic carcinoma [2]. Any patient with decreased vision or squint should undergo detailed dilated fundus examination. Any suspicious lesion, such as retinocytoma, which is a spontaneous arrest variant of retinoblastoma seen in older children, with an incidence of 1.8% to 10% among retinoblastoma patients [8] should keep the ophthalmologist alert for close follow with swept-source optical coherence tomography (SSOCT) or optical coherence tomography angiography (OCT-A) for tumor recurrence [9].
Conclusion
FNAC can provide a supportive role in the diagnosis of rarely occurring adult-onset retinoblastoma cases. It is especially helpful in ruling out benign conditions from malignant lesions and can aid in preoperative counseling for patients who are unwilling for enucleation without a definitive diagnosis.
Financial Support and Sponsorship
Nil
Conflicts of Interest
There are no conflicts of interest.
References
-
Bishop JO, Madson EC (1975) Retinoblastoma: Review of the current status. Surv Ophthalmol 19(6): 342-366.
-
Sengupta S, Pan U, Khetan V (2016) Adult onset retinoblastoma. Indian J Ophthalmol 64(7): 485-491.
-
Mukhija R, Lomi N, Kumar S, Sen S (2019) Retinoblastoma in an adult: A diagnostic dilemma. BMJ Case Rep 12(10): e230537.
-
Shields JA, Shields CL, Ehya H, Eagle RC, Potter PD (1993) Fine-needle aspiration biopsy of suspected intraocular tumors. The 1992 Urwick Lecture. Ophthalmology 100(11): 1677-1684.
-
Augsburger JJ, Shields JA, Folberg R, Lang W, O’Hara BJ, et al. (1985) Fine needle aspiration biopsy in the diagnosis of intraocular cancer. Cytologic-histologic correlations. Ophthalmology 92(1): 39-49.
-
Karcioglu ZA, Gordon RA, Karcioglu GL (1985) Tumor seeding in ocular fine needle aspiration biopsy. Ophthalmology 92(12): 1763-1767.
-
Orellana ME, Brimo F, Auger M, Galic J, Deschenes J, et al. (2010) Cytopathological diagnosis of adult retinoblastoma in a vitrectomy specimen. Diagn Cytopathol 38(1): 59-64.
-
Singh AD, Santos CM, Shields CL, Shields JA, Eagle RC (2000) Observations on 17 patients with retinocytoma. Arch Ophthalmol 118(2): 199-205.
-
Pujari A, Azad SV, Meel R, Lomi N (2018) Bilateral retinocytoma: multimodal imaging assessment. BMJ Case Rep 11(1): e225908.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report