SARS-Cov-2 Associated Paracentral Acute Middle Maculopathy: A Case Report with a Challenging Diagnosis
We present an intricate case of Paracentral acute middle maculopathy (PAMM) as part of the COVID-19 complex clinic presentation. 53 years old patient, pediatric nurse developed symptoms specific to SARS-Cov-2 infection (dry cough, headaches, myalgia’s and fever) which prompted her to get tested. 11 days into the disease, she experienced right eye mild loss of vision and received a short course of steroids for her concomitant pulmonary disease with no subjective improvement on vision. After 2 weeks of self-isolation, she had an ophthalmology examination and was misdiagnosed with optic neuritis. As her visual acuity was 6/6 she was monitored closely with perimetry and OCT. Patient showed reduction of central scotoma with no further treatment. One year later, an Angio-OCT was performed and upon reviewing the initial images, PAMM diagnosis was made
Introduction
Coronavirus involvement of the eye is one of the chapters that still bring new discoveries as the pandemic continues. From anterior segment manifestations such as conjunctivitis and episcleritis to posterior segment manifestations such as vascular occlusions to neuro-ophthalmic involvement, COVID-19 eye spectrum is unfolding as a complex disease [1].
We present the case of a 53 years old patient, pediatric nurse who developed SARS-CoV-2 in August 2020 and consecutive Paracentral acute middle maculopathy (PAMM). The initial symptoms were similar to any cold: dry cough, headaches, myalgia’s and fatigue, followed by fever one week later. PCR for Sars-CoV-2 infection came back positive and the patient had to self-isolate for 2 weeks as per current legislation. 11 days from the first symptoms, she developed a right eye central scotoma describing a cobweb and photopsias without headache or painful eye movements. As she was self-isolating, she was not able to have an ophthalmology examination. Her monitoring doctor recommended her a short course of methylprednisolone at home for the pulmonary concomitant disease for 8 days: 32mg for 2 days, 16mg for 2 days, 8mg for 2 days and 4mg for 2 days. Patient described that visual symptoms didn’t improve. At beginning of September (2 weeks from the vision loss episode) she had her first ophthalmology examination: best corrected visual acuity (BCVA) right eye 6/6, left eye 6/5, no relative afferent pupillary defect (RAPD), right eye 10/17 Ishihara plates-diffuse changes in 2-9 and 10-17 group, left eye 17/17 Ishihara plates, both eyes normal intraocular pressures 12mmHg, fundus examination: both eyes tilted optic discs and right eye persistence of myelinated nerve fibers, without any other pathological findings. Fundus colour photographs and auto fluorescence were acquired with Optos Daytona (Figure 1a-d). Auto fluorescence was unremarkable.
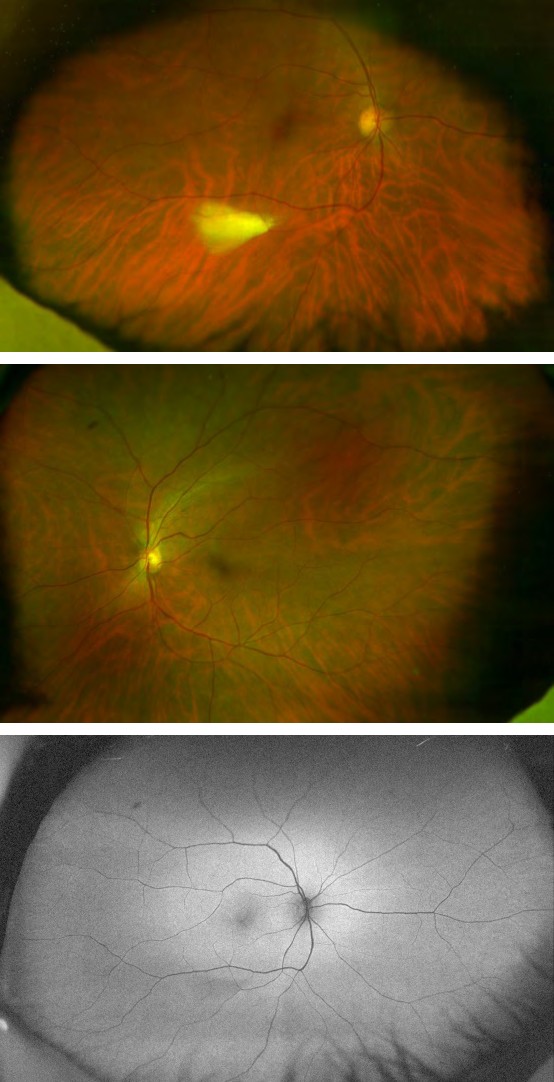
Figure 1a: Right eye colour fundus photography.
Figure 1b: Left eye colour fundus photography.
Figure 1c: Right eye fundus auto fluorescence.
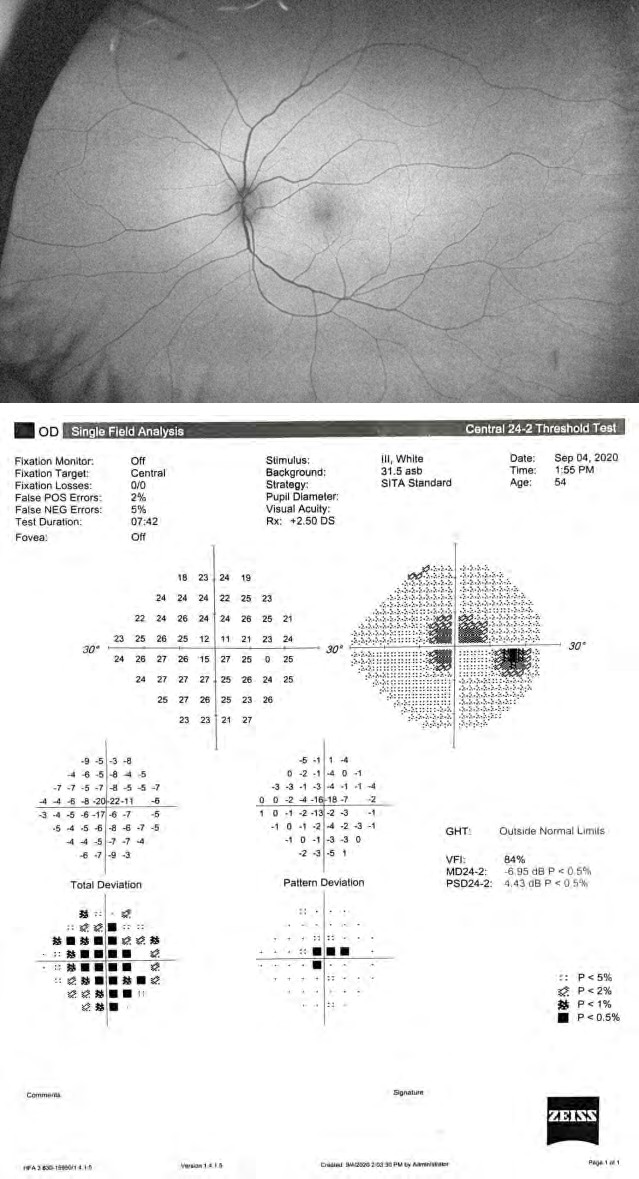
Figure 1d: Left eye fundus auto fluorescence.
Central 24-2 and Full field 120 point perimetry were performed using Zeiss Humphrey Field Analyzer. Right eye perimetry showed enlarged blind spot, central scotoma and peripheral defects (Figure 2a & 2c), left eye no pathological findings. Ganglion Cell Complex (GCC) and retinal nerve fiber layer (RNFL) were analyzed with Zeiss Cirrus 4000. GCC showed initial thinning (Figure 3a), but RNFL was normal (Figure 3c) which should have prompted for further enquiries into the disease, instead a misdiagnosis of optic neuritis was made. Bloods done at one month showed the following changes: erythrocyte sedimentation rate 80 (normal range 0-25mm/hr), C-reactive protein 1.2 (0-1mg/dL), fibrinogen 702 (150-400 mg/dL) and cholesterol 269 (120-200 mg/ dL). MRI performed at one month (also with delay, the health system being congested due to the pandemic) showed no contrast enhancement of the optic nerve. As there were no active lesions on MRI we decided no further treatment and only close monitoring. At 4 months follow-up, the central scotoma and peripheral defects have reduced considerably (Figure 2a-d), BCVA right eye 6/6, left eye 6/5, no RAPD, Ishihara test right eye improved to14/17, GCC and RNFL thinning were observed (Figure 3a-d).
At one year follow-up, an Anglo-OCT was performed with Topcon Triton which showed right eye deep plexus changes (nasal and temporal) (Figure 4a). The acquisition time of this type of OCT machine is longer and obtaining the image was difficult as the patient couldn’t fixate properly. Right eye macula OCT also showed inner nuclear layer (INL) atrophy (Figure 4b), which prompted the case to be reviewed. Hyper- reflectivity of INL was observed on initial right eye Zeiss macula OCT which was overlooked (Figure 3e & 3f). A diagnosis of PAMM was made. Visual Fields were also performed showing further reduction of the remaining central scotoma. Visual acuity remained stable right eye 6/6, left eye 6/5.
Figure 2a: Central 24-2 visual field at 2 weeks.
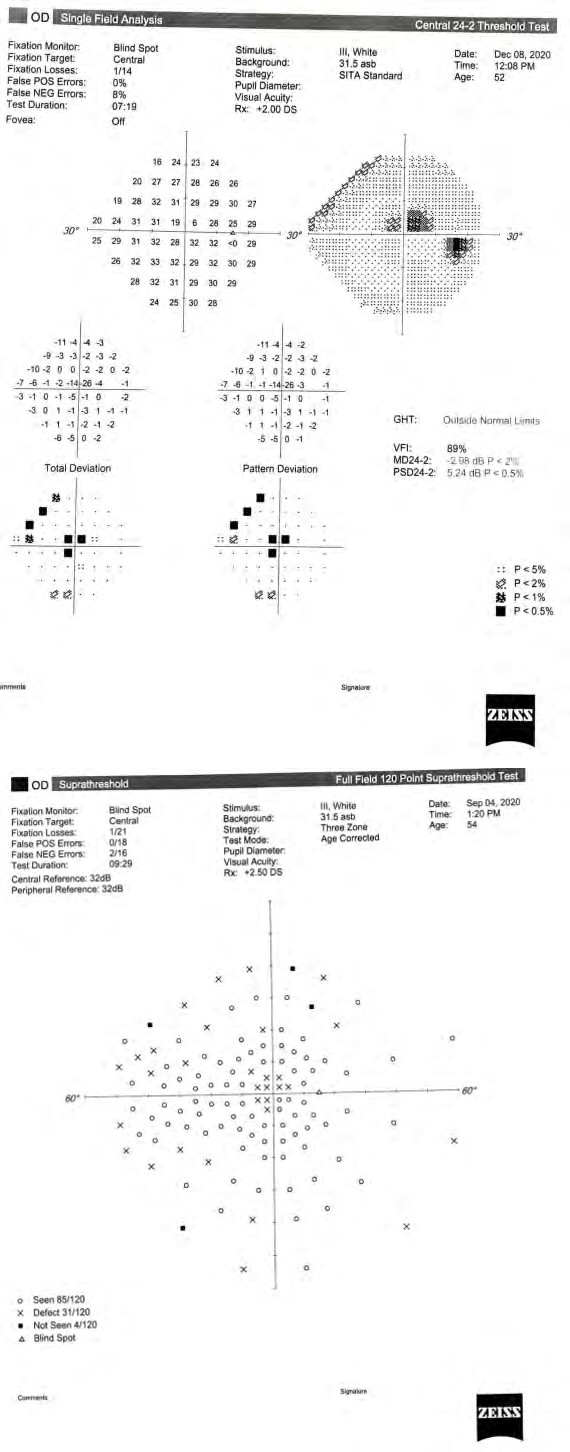
Figure 2b: Central 24-2 visual field at 15 weeks.
Figure 2c: Full field 120 point at 2 weeks.
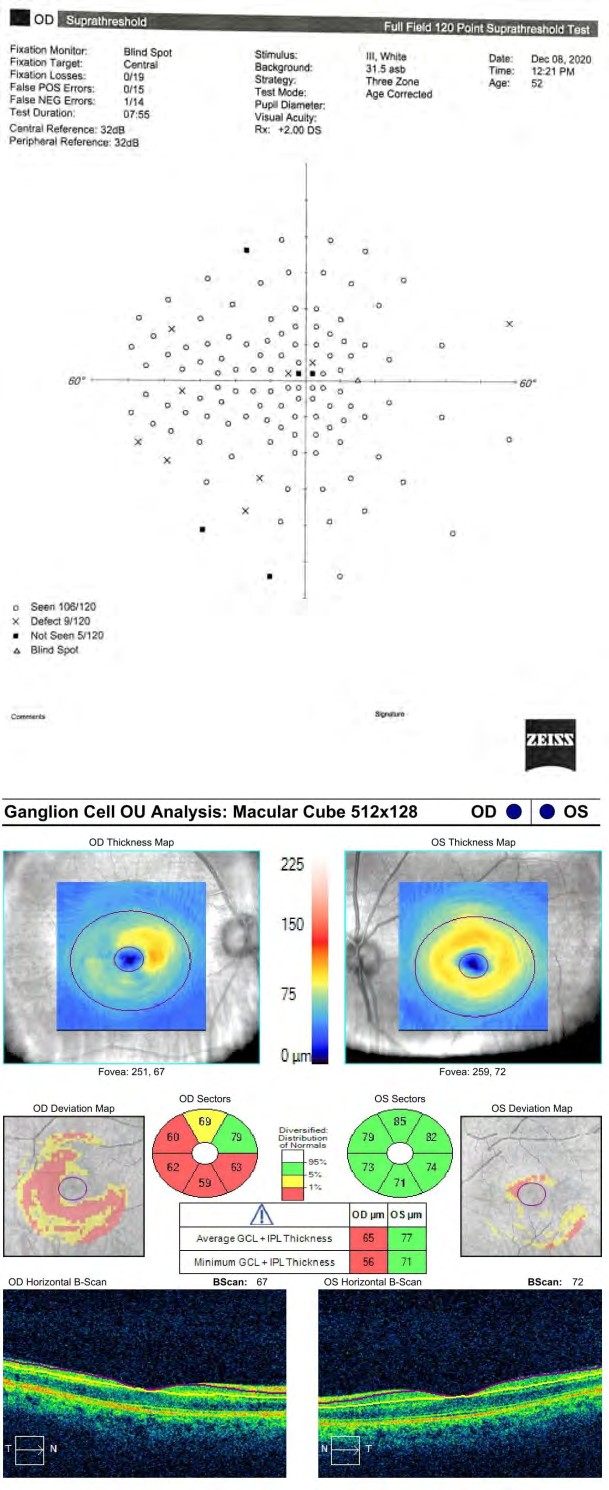
Figure 2d: Full field 120 point at 15 weeks.
Figure 3a: Ganglion Cell Complex (GCC) analysis at 2 weeks.
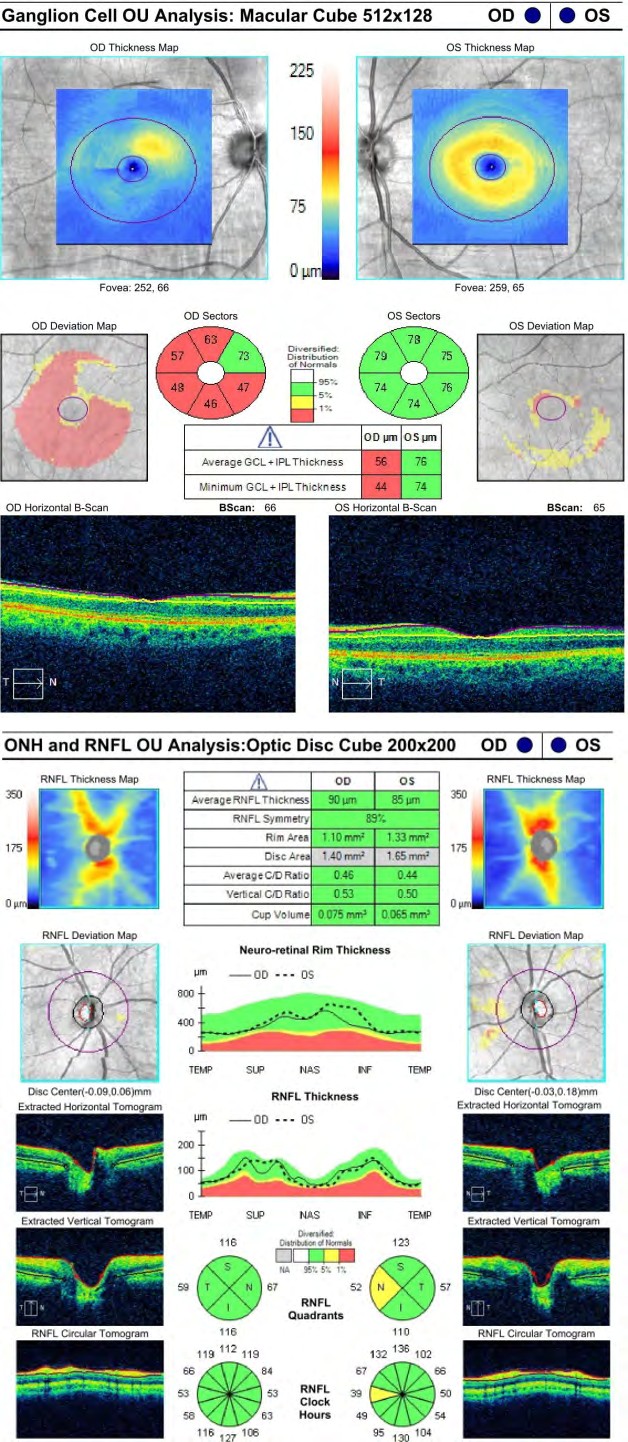
Figure 3b: Ganglion Cell Complex (GCC) analysis at 16 weeks.
Figure 3c: Retinal nerve fiber layer (RNFL) analysis at 2 weeks.
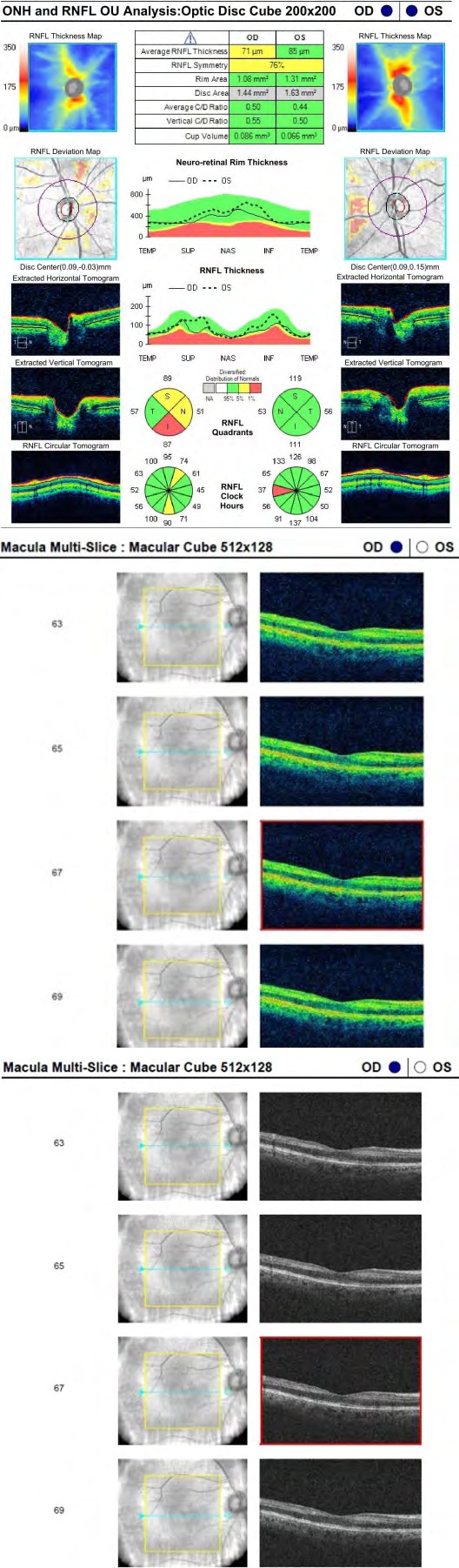
Figure 3d: Retinal nerve fiber layer (RNFL) analysis at 16 weeks.
Figure 3e: Right eye colour Zeiss Cirrus macula OCT at 2 weeks.
Figure 3f: Right eye gray scale Zeiss Cirrus macula OCT at 2 weeks.
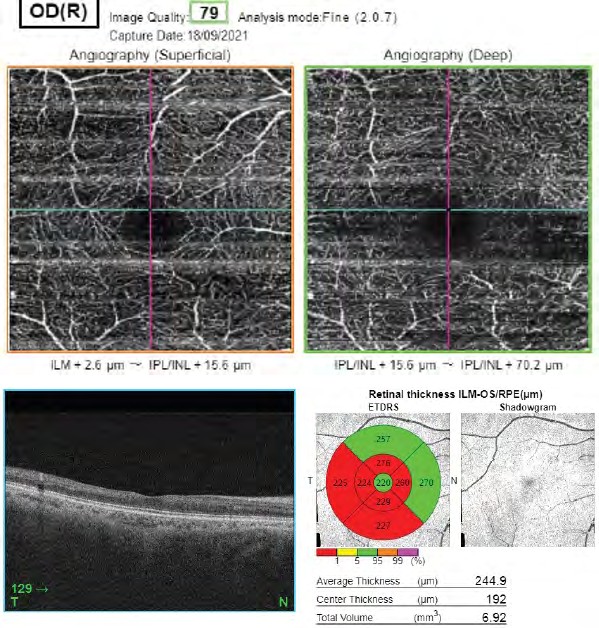
Figure 4a: Right eye superficial and deep plexus Topcon Triton Angio-OCT at one year.
Figure 4b: Right eye Topcon Triton macula OCT at one year.
Discussion
The particularity of this case resides in the fact that the Paracentral acute middle maculopathy (PAMM) diagnosis was made with a delay of one year. The similar presentation between optic neuritis and PAMM made this mistake to be done easily. First exclamation mark should have been given by the other published COVID optic neuritis cases characterized by incapacitating visual acuities ranging from 20/200 to hand movements, RAPD, painful eye movements and MRI showing optic nerve lesions with contrast enhancement [2, 3, 4, 5]. The second exclamation mark should have been given by GCC thinning before RNFL involvement which highlighted an anterograde optic nerve disease mechanism, a sign of macular disease with consecutive optic nerve partial atrophy. Also the 2 weeks self-isolation pandemic rules imposed by our country didn’t help either as the hyper-reflective OCT changes were attenuated and easily overlooked. The details would have been better appreciated on the gray scale instead of the colour spectrum, a detail which was disregarded (Figure 3e versus Figure 3f). The perimetry contributed to further confusion, as central scotoma and enlarged blind spot are typical findings for many cases of optic neuritis.
The presumed mechanism of Paracentral acute maculopathy is vascular, a localized retinal capillary ischemia in the intermediate or deep plexus and may occur isolated or associated with other vascular occlusions. Vascular damage can appear either because of the hypercoagulable state or due to a vasculitis process caused by direct viral infection of the endothelial cells. The inner nuclear layer is affected and hyper-reflective parafoveal bands can be seen on OCT in the acute phase and thinning of the involved retinal layers in the chronic phase. OCT angiography shows decreased vascular density in the deep capillary plexus. Majority PAMM cases show typical minimal ocular signs – paracentral or central scotoma and can be accompanied by good visual acuity. SARS-CoV-2 associated PAMM seems to appear in younger patients than diabetes or hypertension associated PAMM, BCVA is 20/20 in most cases, majority of patients describe a central scotoma and one in three patients has coagulation and inflammatory changes [6, 7, 8, 9, 10]. These findings compare well with our case report and should have pointed sooner towards the right diagnosis. Our case report differs from other published cases as the path to the diagnosis was not clear from the start as details were overlooked. We highlight the similarities between optic neuritis and PAMM and how we could have prevented misdiagnosing the patient and we emphasize on team work as being essential as the patient underwent investigations at several clinics. This can be difficult especially during Covid pandemic when access to certain tests and procedures was more difficult to obtain or was delayed considerably.
Acknowledgements
We thank Mr. Cudrnak Tomas, retina consultant, Plymouth NHS Trust, UK for the case review and retinal input. We also thank Arcadia Private Hospital for the Cirrus OCT measurements and Sanoptic Private Clinic – Dr. Galan and Dr. Mares for the Optos Daytona fundus photos. Last, but not least, we thank Dr Anton for the MRI and Dr. Obada for the Angio-OCT measurements. We highly value the team work which made possible this article.
Declaration of Patient Consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient has given their consent for their images and other clinical information to be reported in the journal.
Financial Support and Sponsorship
Nil.
Conflict of Interest
There are no conflicts of interest.
References
-
Sen M, Honavar SG, Sharma N, Sachdev MS (2021) Covid-19 and Eye: A review of Ophthalmic Manifestations of Covid-19. Indian J Ophthalmol 69(3): 488-509.
-
Sawalha K, Adeodokun S, Kamoga GR (2020) COVID-19- Induced Acute Bilateral Optic Neuritis. J Investig Med High Impact Case Rep 8: 2324709620976018.
-
Zhou S, Jones-Lopez EC, Soneji DJ, Azevedo CJ, Patel VR (2020) Myelin Oligodendrocyte Glycoprotein Antibody- Associated Optic Neuritis and Myelitis in COVID-19. J Neuroophthalmol 40(3): 398-402.
-
Palao M, Fernandez-Diaz E, Gracia-Gil J, Romero-Sanchez CM, Diaz-Maroto I, et al. (2020) Multiple sclerosis following SARS-CoV-2 infection. Mult Scler Relat Disord 45: 102377.
-
Pascual BB, Gegundez JA, Valle DD, Villalobos PA, Carreno E, et al. (2020) Panuveitis and Optic Neuritis as a Possible Initial Presentation of the Novel Coronavirus Disease 2019 (COVID-19). Ocul Immunol Inflamm 28(6): 922-925.
-
Virgo J, Mohamed M (2020) Paracentral Acute Middle Maculopathy and acute neuroretinopathy following Sars-Cov-2 infection. Eye (Lond) 34: 2352-2353.
-
Egea JMO, Medrano JR, Moreno JMR (2021) Retinal Imaging Study Diagnoses in Covid-19: A Case Report. J Med Case Rep 15: 15.
-
Ozsaygili C, Bayram N, Ozdemir H (2021) Cilioretinal artery occlusion with paracentral acute middle maculopathy associated with COVID-19. Indian J Ophthalmol 69(7): 1956-1959.
-
Esfahani HR, Pour EK, Fadakar K, Ebrahimiadib N, Ghassemi F, et al. (2021) Multimodal imaging for paracentral acute maculopathy; The diagnostic role of en face OCT. Int J Retina Vitreous 7(1): 13.
-
Dansingani KK, Inoue M, Engelbert M, Freund KB (2015) Optical coherence tomographic angiography shows reduced deep capillary flow in paracentral acute middle maculopathy. Eye (Lond) 29(12): 1620-1624.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report