Ocular Trauma - Management: A Case Report
Ocular morbidity resulting from trauma remains most common cause of uniocular and non-congenital visual loss across the world. Penetrating injury threatens the integrity of the globe and constitutes an ocular emergency. We report a case of a 21-year-old male, who presented at our Centre within two hours of Type C, Grade D, and Zone 2 injury with a retained metallic foreign body. Primary repair was done after a prompt and detailed examination to maintain the globe integrity. This was followed by removal of foreign body with lensectomy as a secondary procedure within the week of the injury. We report this case to highlight the surgical dilemmas that may be faced by the surgeon while dealing with an ocular emergency
Introduction
As per literature, ocular trauma is one of the major causes of ocular morbidity and blindness. According to WHO, 55 million eye injuries result in the restriction of daily activities per year [1, 2]. Globally, there are approximately 1.6 million people blind due to ocular trauma; 2.3 million people are bilaterally visually impaired and 1.9 million have unilateral vision loss [3, 4]. Ocular trauma may result in a socioeconomic and psychological impact on patients and their families. Therefore, appropriate, and timely management of ocular trauma is crucial. We hereby, describe a case of a penetrating ocular injury with retained intraocular foreign body (RIOFB) successfully managed with staged surgical approach. Globe integrity was achieved by primary repair of corneoscleral laceration in the first stage followed by removal of RIOFB in the second stage. Visual rehabilitation is planned with intraocular lens implantation as a third and final stage procedure.
A 21-year-old male student presented to our institute with the history of injury to his right eye (OD) with sharp metallic object at his workplace associated with sudden painful diminution of vision, redness, discharge, inability to open the injured eye and intolerance to the ambient light. As stated by the patient, while working with a machine, a piece of iron dislodged and penetrated his right eye at very high velocity. He did not give history of any piece ejecting from the eye or any use of protective eye gear used while working. Specifically asked for, he denied history of assault or alcohol intake and gave no history of loss of consciousness, seizures, or ear nose throat bleed after the injury. His past surgical history is significant for refractive surgery two years ago.
There was no history of any ocular trauma in past or any systemic illness. His personal and family history was not significant. On examination, his uncorrected visual acuity was perception of light with accurate projection of rays in the right eye and 20/20 in left eye (OS). IOP in the left eye was 14 mmHg as measured on non-contact tonometer (NCT). The extra ocular movements in both the eyes were full and free (Figure 1).
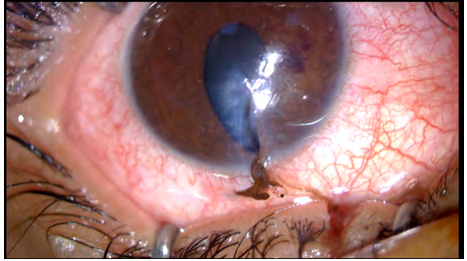
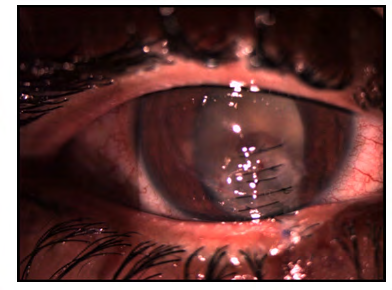
There was a 2 mm full thickness vertical lower lid tear at the junction of medial one-third and lateral two-third with diffuse conjunctival congestion in the right eye. On slit-lamp examination, the right eye showed a full thickness corneoscleral tear inferiorly extending horizontally from 5:00 to 5:30 clock position and vertically extending up to center of the pupil, approximately 6mm in length (Figure 1) with iris incarceration in the wound, flat anterior chamber and grossly hypotonous globe. Posterior segment could not be evaluated due to media haze but red glow was present. Vertical edges of tear did not show any impacted foreign body but there was surrounding stromal edema. Anterior chamber was flat with an organized blood clot measuring 2mmx 3mm present at 3 o clock to 4 o clock position. Pupil of the right eye was keyhole in shape and with sluggish reaction to light. Left eye was normal (Figure 2).
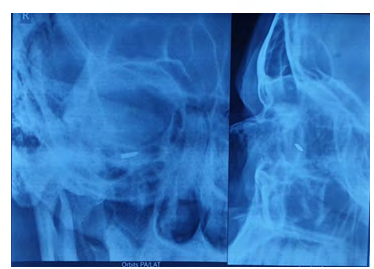
In the left eye, fundus was found to be within normal limits with the cup disk ratio of 0.3:1 and a healthy neuro- retinal rim. Retina was attached and the foveal reflex was present. Provisional diagnosis of right eye was: Open globe injury classified as Type C, Grade D, and Zone 2 according to Ocular trauma score (OTS) Classification consisting of a 6 mm penetrating cornea scleral laceration and 2 mm full thickness lower lid laceration. On radiological investigation, X-ray Orbits (PA and Lateral views) revealed inferior metallic IOFB (Figure 3).
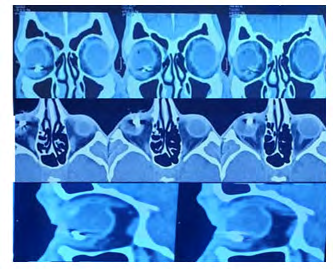
Thin 2 mm cuts in axial and coronal sections in NCCT Orbit also displayed metallic IOFB approximately 7.6 x 4.3 mm (12961-16244 HU) in dimensions in the inferior aspect of right globe in the posterior chamber along with intraocular air foci in vitreous cavity. Based on the above findings, the staged surgical approach was planned. Primary repair of corneoscleral laceration and lid tear of right eye was planned under local anaesthesia with intracameral injection (vancomycin, ceftazidime, voriconazole) under very guarded visual prognosis in view of metallic foreign body in the posterior segment and no visualisation of the fundus (Figure 4).
Conjunctival peritomy was done to determine the posterior limit of the scleral wound and it was sutured using 8-0 vicryl in a zippering fashion. The limbus was opposed by a single nylon suture. Cornea was sutured using 10-0 nylon in keeping with the principles of corneal repair [5]. Conjunctival laceration and lid margin tear were also sutured using 8-0 vicryl. Intracameral antibiotic (2.25mg/0.1 ml ceftazidime and 1mg/0.1ml vancomycin) and voriconazole (100ug/0.1ml) were injected prophylactically. Seidel’s test was done to ascertain the water tight anterior chamber. Initial medical management included bed rest, head end elevation, Injection Tetanus Toxoid IM stat, Tablet Ciprofloxacin 750 mg twice a day for 5 days, Tablet Diclofenac and Serratiopeptidase twice a day for 5 Days, Tablet Prednisolone Acetate 60 mg once a day for 7 days, Tablet Pantoprazole 40 mg once a day for 7 days, Tablet Paracetamol(325mg), Tramadol(37.5mg) SOS (Si Opus Sit, if necessary), Eye drop (E/D) Moxifloxacin
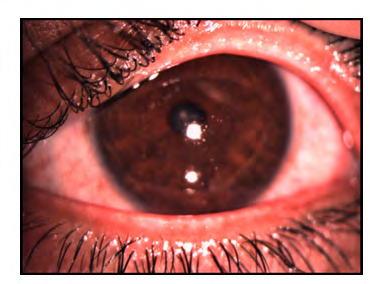
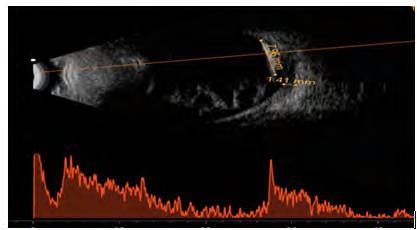
0.5% 6 times a day, E/D Tobramycin 0.3% six times a day, E/D Vancomycin 0.5% six times a day, E/D Natamycin 5% six times a day, E/D Atropine 1% three times a day. On post-operative day 1 (POD-1), the examination of right eye revealed vision to be hand movements close to face, projection of rays (PR) was accurate. Seidel’s test was negative. Intraocular pressure on digital examination was within normal limits. There was mild stromal edema around the wound. Anterior Chamber (AC) was formed. Ultrasound B-scan was done where lens echoes were noted. Vitreous cavity showed few dot and membranous echoes suggestive of vitreous haemorrhage. There were high reflective intensity echoes with 100% spike with back shadowing suggestive of IOFB in the inferior half (Figure 5). On a postoperative day three (POD-3), visual acuity in the right eye improved to finger counting close to face with an IOP of 13mmHg on NCT (Figure 6).
On subsequent follow-up visits, there was an increase in anterior chamber (AC) reaction with lens matter in AC. Serial ocular ultrasound B-scan revealed vitreous hemorrhage and RIOFB with a mild increase in low amplitude spike suggestive of an increase in vitritis with normal retinal, choroidal, and scleral (RCS) thickness. Eight days following primary repair, pars plana lensectomy with pars plana vitrectomy with RIOFB removal was performed. Three pars plana vitrectomy ports were made. Core and peripheral vitrectomy were performed and per fluorocarbon liquid (PFCL) was injected. The metallic FB was present on the inferior retina (Figure 7A,7B).
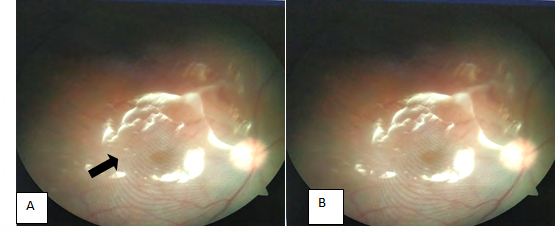
Figure 7A: Intraoperative image of the right eye showing a metallic foreign body on the inferior retinal surface (arrow). 7B: Fundus picture of the right eye on postoperative day one showing silicone oil filled eye with retina attached.
It was lifted from the retina using an 18-gauge intraocular rare earth magnet and was delivered in the AC. A 2.2 mm clear corneal incision was made and the metallic FB was removed using serrated forceps. A retinal break was noted infero-nasally with a nasal retinal detachment. Following the fluid-air exchange, subretinal fluid was drained. Laser was done 360 degrees, around the retinal break, and the primary impact site. Silicone oil was injected for endotamponade. All three port sites were sutured using 7-0 vicryl and intravitreal antibiotic (2.25mg/0.1 ml ceftazidime+ 1mg/0.1ml vancomycin) and voriconazole (100ug/0.1ml) was injected. On postoperative day one (POD 1) (Figure 7B), the BCVA in the right eye was hand movements close to face with IOP of 17 mmHg on NCT. The patient was aphakic with attached retina. On one month follow-up visit, Best Corrected Visual Acuity (BCVA) in the right eye was 6/18 on Snellen visual acuity chart and IOP of 16mmHg on NCT. The retina is attached with mild temporal optic disc pallor. The patient will be planned for right eye scleral fixated IOL surgery.
Discussion
It has been estimated that 90% of all ocular injuries are preventable. In a study conducted at Banaras Hindu University, majority (82.1%) of their cases, traumatic agent was solid in nature and the most common mode of injury was a projectile object (35.8%). About 45% of injury victims had isolated ocular trauma and rest 55% had polytrauma. Majority (98.4%) of participants were not using any protective device at the time of injury. Almost 91.5% of victims had unilateral eye involvement [6]. Although the techniques and principles of primary repair are clearly established across literature, the timing of cataract removal is often a major dilemma faced by surgeons. Cataract is estimated to occur in up to 65% of eye trauma cases and is a major cause of acute and longstanding visual loss worldwide [7]. Disruption of the lens capsule due to trauma results in cataract formation which may be anterior or posterior subcapsular cataract or a rosette cataract. The standard recommendation in a penetrating globe injury is primary globe closure, followed by a secondary cataract removal and intraocular lens implantation [8]. It is imperative to maintain the structural integrity of the globe. There are some advantages offered by this method. Firstly, if the location of cataract is peripheral, it may be visually insignificant and can be corrected later. Secondly, the cataract removal can be technically more difficult in the primary procedure due to poor visualization from resulting media opacities in the cornea, anterior segment, and posterior segment. Primary removal of cataract may be advocated if there is extensive damage to lens capsule with the presence of cortical matter in AC which may exaggerate the inflammatory reaction in the eye and aid early visualization of the posterior segment. It is especially advocated in cases of pediatric trauma where there is a risk of development of amblyopia.
The other dilemma may be in the management of retained intraocular foreign body. RIOFB is defined as intraocularly retained, unintentional projectiles and require urgent diagnosis and treatment to prevent blindness or globe loss [9]. IOFB accounts for 16-40% of ocular injuries [10]. Most of the ocular trauma with RIOFB is work-related and is common among young males. Hammering is the most common mode of ocular injury [11] and metallic foreign bodies are the most common type of FB [12]. The ocular damage caused by FB is related to the mode of injury, nature of the IOFB, and associated complications such as vitreous loss and retinal damage [13]. Therefore, a thorough evaluation for RIOF is essential in case of an ocular injury. Not all FB can be detected on ocular slit lamp bio microscopic examination and indirect ophthalmoscopy. Ocular ultrasound B-scan gives real-time imaging and has specificity and sensitivity of 98.87% and 91.5% respectively in ocular trauma [14]. The detection rate of metallic FB on X-ray orbit (AP and lateral view) is 90%, 70% for glass FB, and 0-15% for others. NCCT orbit is highly sensitive with a detection rate of approximately 100% for a metallic foreign body of >0.5mm [14]. The nature of FB can also be determined using the Hounsfield unit (HU). MRI is useful in identifying glass and wooden foreign bodies and should be done once the presence of metallic FB has been ruled out.
Strategic management of RIOFB is essential. Once life- threatening conditions are ruled out following trauma, immediate primary repair of the ocular perforation is indicated to salvage the eye and reduce the risk of infection. As the risk of post-traumatic endophthalmitis is high with RIOFB (relative risk of 6.9-16.5) [15], topical and systemic antibiotics are started immediately. Intravitreal/ intracameral broad-spectrum antibiotics must be injected prophylactically after the primary repair [16]. The timing for removal of RIOFB depends on the general medical status of the patient, composition of FB, and availability of trained personnel and operating instrument. Immediate removal of RIOFB is indicated if there are signs of endophthalmitis. Otherwise, one can wait for corneal edema to get resolved, inflammation to reduce and ocular tissue to gain strength.
There are various strategies for the removal of RIOFB based on the location, nature, and size of FB. For FB located in the AC, it can be removed using serrated forceps or an ocular magnet. Small FB (1mm) in the posterior chamber can be removed using an internal magnet or vitrectomy cutter. Foreign bodies of 1-3mm size can be removed using intraocular forceps, internal magnets, or basket forceps. A larger FB of 3-5mm can be removed using diamond- coated forceps, and an internal magnet after enlarging the sclerotomy wound [8] foreign body of more than 5mm size is removed from making a limbal incision or scleral tunnel. IOFB should be freed from the vitreous before its removal. Laser around intraretinal foreign body should be done before its removal. Peripheral retina is inspected for any retinal break after removal of RIOFB.
Conclusion
All ocular traumas are ophthalmic emergencies which must be evaluated and treated promptly. The presence of any RIOFB should be evaluated in order to decide the further course of treatment. Strategic and timely intervention is essential to salvage the eye and vision and to prevent the development of post-traumatic endophthalmitis.
Acknowledgement
We would like to thank our cornea and retina teams for prompt but detailed examination and apt management of the patient. We would like to especially acknowledge Dr. Tulika Chauhan for her expertise in primary laceration repair. We would also like to extend our thanks to Dr. Obuli Ramachandran and Dr. Gauri Khare for their proficient management of RIOFB. This research would not have been complete without the help and guidance from Dr. Sagarika Patyal. We would like to thank the nursing staff, OT technicians and the entire team at Centre for Sight for their cooperation.
References
-
Acar U, Tok OY, Acar DE, Burcu A, Ornek F (2011) A new ocular trauma score in pediatric penetrating eye injuries. Eye (Lond) 25(3): 370-374.
-
Natarajan S (2013) Ocular trauma, an evolving sub specialty. Indian J Ophthalmol 61(10): 539-540.
-
Negrel AD, Thylefors B (1998) The global impact of eye injuries. Ophthalmic Epidemiol 5(3): 143-169.
-
Pizzarello LD (1998) Ocular trauma: Time for action. Ophthalmic Epidemiol 5(3): 115-116.
-
AAO BSCS 2021- 2022 Basic techniques of ophthalmic surgery, 586-589.
-
Maurya RP, Srivastav T, Singh VP, Mishra CP, Mujaini AA (2019) The epidemiology of ocular trauma in Northern India: A teaching hospital study. Oman J Ophthalmol 12(2): 78-83.
-
Jacobs EJ, Tannen BL (2016) Traumatic Cataract: A Review. J Ocular Biol 4(1): 4
-
AAO BSCS 2021- 2022 Basic techniques of ophthalmic surgery, 592-593.
-
Jung HC, Lee SY, Yoon CK, Park UC, Heo JW, et al. (2021) Intraocular Foreign Body: Diagnostic Protocols and Treatment Strategies in Ocular Trauma Patients. J Clin Med 10(9): 1861.
-
Pieramici DJ, MacCumber MW, Humayun MU, Marsh MJ, Juan ED (1996) Open-globe injury: Update on types of injuries and visual results. Ophthalmology 103(11): 1798-1803
-
Liu CC, Tong JM, Li PS, Li KK (2017) Epidemiology and clinical outcome of intraocular foreign bodies in Hong Kong: a 13-year review. Int Ophthalmol 37(1): 55-61.
-
Greven CM, Engelbrecht NE, Slusher MM, Nagy SS (2000) Intraocular foreign bodies: management, prognostic factors, and visual outcomes. Ophthalmology 107(3): 608-612.
-
Anguita R, Moya R, Saez V, Bhardwaj G, Salinas A, et al. (2021) Clinical presentations and surgical outcomes of intraocular foreign body presenting to an ocular trauma unit. Graefes Arch Clin Exp Ophthalmol 259(1): 263-268.
-
Shazlee MK, Ali M, Ahmed MS, Hussain A, Hameed K, et al. (2016) Diagnostic Accuracy of Ultrasound B scan using 10 MHz linear probe in ocular trauma; results from a high burden country. Pak J Med Sci 32(2): 385-388.
-
Kumar Atul, Ravani Raghav (2018) Post-traumatic Endophthalmitis. In: Retina: medical and surgical management textbook 1st (Edn.), Jaypee Brothers Medical Publishers, New Delhi, India, pp: 734.
-
Thevi T, Abas AL (2017) Role of intravitreal/intracameral antibiotics to prevent traumatic endophthalmitis-Meta- analysis. Indian J Ophthalmol 65(10): 920-925.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report