Unique Optical Coherence Tomography Imaging in Spontaneous Closure of Full Thickness Macular Hole Post Laser Photocoagulation
Purpose: To study events in spontaneous full thickness macular hole (FTMH) closure following laser photocoagulation (LP). Methods: Retrospective case study of a patient of spontaneous FTMH closure documented by SD-OCT following laser. Results: A 51-year-old lady presented with FTMH and a subclinical retinal detachment (RD) in her right eye. LP for subclinical RD was done and surgery for FTMH was advised. On day of surgery, repeat SD-OCT showed spontaneous closure of FTMH with an outer retinal defect, following which surgery was abandoned. Conclusion: Spontaneous PVD induction relieves antero-posterior traction and Inner limiting membrane (ILM) micro breaks relieves tangential traction, which can result in spontaneous closure of FTMH.
Introduction
Formation of an idiopathic macular hole has been attributed to mechanical forces exerting tangential traction at the vitreomacular interface as well as antero-posterior vitreoretinal traction of the posterior hyaloid on the parafovea [1, 2]. The spontaneous closure of an idiopathic macular hole has been attributed to bridging retinal tissue, vitreofoveal separation, and a small diameter size of the hole [3]. In this report, we demonstrate a unique event of spontaneous closure of full thickness macular hole immediately following laser photocoagulation of the peripheral retina. To the best of our knowledge, this is the first such report of laser photocoagulation causing closure of macular hole (Figures a,b).
A 51-year-old lady presented to our hospital with decreased vision in right eye (RE) of 2 months duration. She had unremarkable systemic or past history. Her best corrected distance visual acuity was 6/18 in RE and 6/36 in left eye (LE). Anterior segment examination revealed bilateral cataract (more in LE). Funduscopy revealed an altered foveal reflex with a small area of subclinical retinal detachment and a lattice in superotemporal periphery of RE. SD-OCT done from elsewhere 15 days back, confirmed stage 3 full thickness macular hole (FTMH) with attached posterior hyloid, according to Gass‘s classification [1] and the international vitreomacular traction study group classification [2] (Figures c,d). She was planned for macular hole surgery. Meanwhile, barrage laser photocoagulation was given for the subclinical retinal detachment with 577 nm yellow laser. As a protocol we repeated OCT on the day of surgery, which revealed complete closure of FTMH with presence of outer retinal defect (ORD) in fovea (Figure e) and inner retinal layer shows multiple micro breaks in ILM (Figure e) with presence of complete posterior vitreous detachment confirmed as weiss ring on fundus imaging (Figure a). 9 months later, followup showed improvement in right eye to 6/9 N6 and OCT revealed complete closure of macular hole with resolution of ORD (Figure f) and regeneration of outer retinal photoreceptors (Figure f).
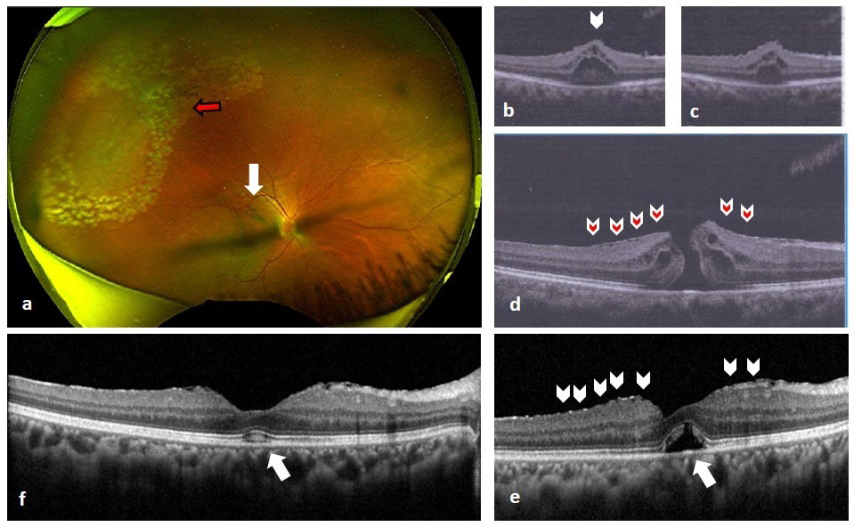
Figure 1: a) Wide field colour fundus photo of right eye showing lasered lattice degeneration in superior temporal quadrant (red arrow) with presence of Weiss ring (white arrow). b,c) OCT showing retinal elevation of posterior vitreous attachment. d) OCT showing FTMH with continuous ILM (red arrow heads). e) SD-OCT on day of surgery showing closure of FTMH with multiple micro-breaks in ILM (white arrow-heads) and presence of outer retinal defect (white arrow). f) SD-OCT showing FTMH closure with complete resolution of ORD and regeneration of outer retinal photoreceptor in fovea (white arrow).
Discussion
Chew, et al. [3] reported that 8.6 % of the cases of idiopathic macular holes can undergo spontaneous closure [3]. Macular hole with the diameter of less than 400 μm, especially less than 250 μm, may have higher chances of spontaneous closure. These spontaneously closed macular holes have some distinctive OCT characteristics, such as the release of VMT, sharp edges of hole, formation of bridge- like structure, epiretinal membrane and cystic structure [4]. Posterior vitreous detachment (PVD) induction followed by retinal laser photocoagulation is a well know phenomenon [5, 6]. In the pathogenesis of ERM, the concept of PVD causing breaks in ILM has been proposed through which glial proliferation takes place and ERM ensues [7]. Presumptively, in our case the sudden PVD induction released antero- posterior traction and caused the multiple micro breaks in ILM eventually also releasing the tangential traction (Figure e), resulting in spontaneous full thickness macular hole (FTMH) closure. In this case there was bridging of inner neuroretinal tissue, which may be the initial step in macular hole repair. There was also presence of an outer foveolar defect (OFD), or outer retinal defect (ORD) in this case following the closure of the hole (Figure e), which can be transiently identified in the first postoperative stage of a FTMH [8]. Outer foveolar defect (OFD) are described to be associated with smaller preoperative MH, and once detected, it disappear at the earliest, in 1 month, and the main time of defect disappearance is of 183 days following surgery [9]. Recently, the development of these lesions has been interpreted as a normal state of recovery after MH repair, more favorable surgical outcome and less-advanced preoperative MH stage [10]. This unusual spontaneous closure of the full thickness macular hole immediately following the laser photocoagulation of the peripheral retina, associated with spontaneous PVD induction and appearance micro breaks in ILM is one rare occurrence and to the best of our knowledge has not been reported before.
References
-
Gass JD (1995) Reappraisal of biomicroscopic classification of stages of development of a macular hole. Am J Ophthalmol 119(6): 752-759.
-
Duker JS, Kaiser PK, Binder S, Smet MDD, Gaudric A, et al. (2013) The International Vitreomacular Traction Study Group classification of vitreomacular adhesion, traction, and macular hole. Ophthalmology 120(12): 2611-2619.
-
Chew EY, Sperduto RD, Hiller R, Nowroozi L, Seigel D, et al. (1999) Clinical course of macular holes: The Eye Disease Case-Control Study Arch Ophthalmol 117(2): 242-246
-
Ishida M, Takeuchi S, Okisaka S (2004) Optical coherence tomography images of idiopathic macular holes with spontaneous closure. Retina 24(4): 625-628.
-
Sebag J, Buzney SM, Belyea DA, Kado M, McMeel JW, et al. (1990) Posterior vitreous detachment following panretinal laser photocoagulation. Graefe’s Arch Clin Exp Ophthalmol 228(1): 5-8.
-
Sebag J, Cuu JN (2017) The effects of vitreous on proliferative diabetic retinopathy and the response to pan retinal photocoagulation. Graefes Arch Clin Exp Ophthalmol 255(2): 421-422.
-
Gross JG (2019) ERM Pathogenesis: Three Theories Suggest Defects of Vitreous and ILM. Retina specialist.
-
Kang SW, Lim JW, Chung SE, Yi CH (2010) Outer foveolar defect after surgery for idiopathic macular hole. American Journal of Ophthalmology 150(4): 551-557.
-
Bottoni F, Angelis SD, Luccarelli S, Cigada M, Staurenghi G (2011) The dynamic healing process of idiopathic macular holes after surgical repair: a spectral-domain optical coherence tomography study. Investigative Opthalmology & Visual Science 52(7): 4439-4446.
-
Powers MA, Shields RA, Moshfeghi AA, Moshfeghi DM (2018) Outer retinal defects represent a normal recovery pathway following internal limiting membrane peeling in macular hole surgery. Ophthalmic Surg Lasers Imaging Retina 49(9): e1–e8.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report