A Case of Adenoid Cystic Carcinoma Mimicking Orbital Pseudotumor
Introduction: Clinical approach to the case of dacryoadenitis. Case Report: A 41-year-old male patient was admitted to our clinic with complaints of decreased vision in the left eye, periorbital and headache for 2 days. On examination, his visual acuity was full on the right and counting fingers at 2 meters on the left. There was a slight swelling and dimness in the margins of the optic disc on the left, other eye examination findings were normal. The patient was treated with intravenous methylprednisolone at a dose of 1gr/day for three days with the prediagnosis of orbital pseudotumor. However, it was observed that the patient's complaints recurred after methylprednisolone was discontinued. In repeated orbital MRI, at the level of the orbital apex on the left, infiltrating the dural structures, indenting the cavernous sinus, affecting the soft tissue structures adjacent to the nasopharyngeal lumen on the left, are seen. The left optic nerve was found to be slightly thicker than normal, especially at the apex level. For histopathological diagnosis, endoscopic biopsy was performed from the tumor and surrounding tissue from the left maxillary sinus. The biopsy result was reported as adenoid cystic carcinoma. Discussion: The diagnosis of orbital pseudotumor is made in accordance with clinical, radiological and pathological data. Orbital pseudotumor is histopathologically characterized by polymorphous inflammatory cell infiltration accompanied by varying degrees of fibrosis. It is difficult to distinguish an orbital pseudotumor from a true neoplasm. Lymphomas constitute 20% of orbital mass lesions. Our case was initially treated with a preliminary diagnosis of orbital pseudotumor localized in the posterior orbit and responded to steroids. However, lack of complete recovery and recurrence after steroid discontinuation brought to mind other underlying pathologies and directed to further examination and biopsy. As a matter of fact, the patient, who was diagnosed with adenoid cystic carcinoma as a result of biopsy, was included in the oncological follow-up and treatment program. It is necessary to be vigilant in terms of malignancy in orbital pseudotumors and not to avoid biopsies in suspected cases.
Introduction
Orbital pseudotumor is a benign idiopathic inflammatory event that can involve any structure in the orbit. It is more common in the population under the age of 50, especially in women. Although it can show bilateral involvement, unilateral involvement is more common. Orbital pseudotumor may be in the form of diffuse inflammatory disease involving all orbital compartments, it may be in the form of myositis, dacroadenitis, perineuritis and periscleritis [1, 2]. In the differential diagnosis of the disease, especially Graves’ ophthalmopathy and orbital lymphoma, and then primary or metastatic tumors, sarcoidosis, Wegener’s granulomatosis, orbital and preseptal cellulitis, vascular pathologies, orbital amyloidosis, foreign body reaction and dermoid cyst should be considered [3, 4]. In this study, the clinical approach to a patient who was treated with the prediagnosis of orbital pseudotumor but recurring complaints and later diagnosed with adenoid cystic carcinoma was examined.
Case Report
A 41-year-old male patient was admitted to our clinic with complaints of decreased vision in the left eye, periorbital and headache for 2 days. He was being followed up with tegretol 800 mg treatment in an external center for about 1 year due to trigeminal neuralgia. On examination, his visual acuity was full on the right and counting fingers at 2 meters on the left. Intraocular pressure was 12 mmHg in the right eye and 14 mmHg in the left eye. Eye movements were free in both eyes. There was a slight swelling and dimness in the margins of the optic disc on the left, other eye examination findings were normal. In the orbital magnetic resonance examination (MRI) of the patient, a heterogeneous contrasting lesion area with unclear borders localized in the orbital apex on the left was observed. The patient was treated with intravenous methylprednisolone at a dose of 1gr/day for three days with the prediagnosis of orbital pseudotumor. After this treatment, the left visual acuity reached 0.2 and the patient’s pain decreased. Oral methylprednisolone, which was started at a dose of 1 mg/kg/day and gradually decreased from the fourth day, was completely discontinued within 1.5 months. However, it was observed that the patient’s complaints recurred after methylprednisolone was discontinued.
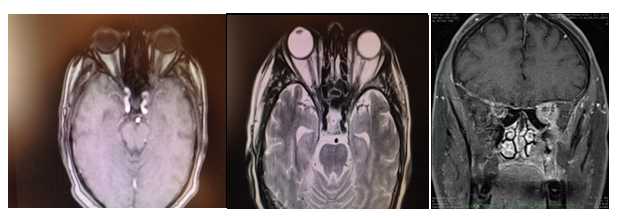
In repeated orbital MRI, at the level of the orbital apex on the left, involving the retroorbital fat tissue and optic nerve sheath, affecting the entire apex, infiltrating the dural structures, indenting the cavernous sinus, extending to the maxillary sinus in the anteroinferior and affecting the soft tissue structures adjacent to the nasopharyngeal lumen on the left, heterogeneously enhanced lesion area with unclear borders, and thickness in the extraocular muscles, prominently in the superior rectus muscle on the left are seen (Figure 1).
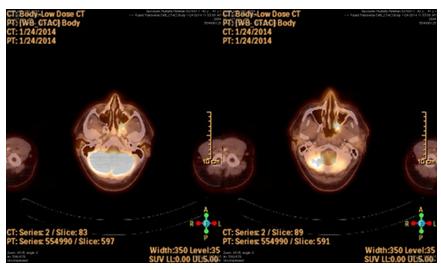
The left optic nerve was found to be slightly thicker than normal, especially at the apex level. In brain computed tomography (CT) angiography, an increase in soft tissue density with irregular borders in the left pterygopalatine fossa, extending to the temporal fossa superiorly and not giving a clear contour feature; irregularities in the left medial pterygoid plate, left maxillary sinus inferomedial wall and left sphenoid bone were observed in its neighborhood. In the positron emission tomographic (PET) examination, an irregularly circumscribed hypermetabolic lesion was observed in the left pterygopalatine fossa with an expanded appearance to the nasal cavity, causing destruction in the left pterygoid bone medial lamina, maxillary sinus inferomedial wall and maxillary bone (Figure 2). For histopathological diagnosis, endoscopic biopsy was performed from the tumor and surrounding tissue from the left maxillary sinus. The biopsy result was reported as adenoid cystic carcinoma. The patient is started to the chemotherapy program.
Discussion
The diagnosis of orbital pseudotumor is made in accordance with clinical, radiological and pathological data. The presence of an underlying malignancy should be excluded in cases that recur and do not receive adequate treatment. Biopsy in orbital pseudotumor cases is controversial. Orbital pseudotumor is histopathologically characterized by polymorphous inflammatory cell infiltration accompanied by varying degrees of fibrosis. Leone, et al. [5] suggested that biopsy in cases with orbital pseudotumor delays the response to treatment and aggravates the clinical situation, and recommended biopsy only to cases that did not respond to steroids or had recurrence or suspected diagnosis. Similarly, there are other studies reporting that biopsy causes worsening in the clinical picture [6, 7]. Contrary to this view, there are also studies indicating that a systemic disease or lymphoid tumors can be ignored if the diagnosis is made without histopathological examination [8]. It is difficult to distinguish an orbital pseudotumor from a true neoplasm [9]. Lymphomas constitute 20% of orbital mass lesions. Clinically, lymphomatous lesions are usually in the form of palpable masses, while orbital pseudotumor cases are often in the form of eyelid edema, optic atrophy, and conjunctival congestion [10].
Our case was initially treated with a preliminary diagnosis of orbital pseudotumor localized in the posterior orbit and responded to steroids. However, lack of complete recovery and recurrence after steroid discontinuation brought to mind other underlying pathologies and directed to further examination and biopsy. As a matter of fact, the patient, who was diagnosed with adenoid cystic carcinoma as a result of biopsy, was included in the oncological follow- up and treatment program. It is necessary to be vigilant in terms of malignancy in orbital pseudotumors and not to avoid biopsies in suspected cases. Endoscopic biopsy may be necessary, especially in posteriorly localized cases. Declaration of Interest: I have no declaration of interest.
References
-
Stevens JL, Rychwalski PJ, Baker RS, Kielar RS (1998) Pseudotumor of the orbit in earlychildhood. J AAPOS 2(2): 120-123.
-
Mahr MA, Salomao DR, Garrity JA (2004) Inflammatory Orbital Pseudotumor with extension beyond the orbit. Am J Ophthalmol 138(3): 396-400.
-
Yesildag A, Adanir E, Koroglu M, Baykal B, Kerman G, et al. (2004) Orbital psodotumor ve hipofiz makroadenom birlikteligi: MRG bulgulari. SDU Tip Fak Derg 11(2): 18- 20.
-
Ayberkin E, Ince E, Tekin D, Fitoz S, Suskan E (2007) Tekrarlayan Orbital Myozitli Bir Olgu. Ankara Universitesi Tip Fakultesi Mecmuasi 60(3): 116-119.
-
Leone CR, Lloyd WC (1985) Treatment protocol for orbital inflammatory disease. Ophthalmology 92(10): 1325-1331.
-
Henderson JW (1994) Orbital Tumors. 3rd (Edn.), RavenPress, New York, USA, pp: 392-400.
-
Jacobiec FA, Font RL (1985) Non-infectious orbital inflammations. In: Ophthalmic Pathology: An Atlas and Textbook. WB Saunders Comp, Spencer WH, Philedelphia, pp: 2777-2795.
-
Char HD, Miller T (1993) Fine-needle aspiration biopsy and response to therapy. Ophthalmology 100(11): 1702- 1710.
-
Kawakami K, Ito R, Tono Y, Yazaki A, Murata T, et al. (2012) Orbital inflammatory lesion as an initial manifestation of systemic nasal type NK/T-celllymphoma. J Clin Exp Hematop 52(2): 137-139.
-
Yan J, Wu Z, Li Y (2004) The differentiation of idiopathic inflammatory pseudotumor from lymphoid tumors of orbit: analysis of 319 cases. Orbit 23(4): 245-254.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report