Isolated Lower Motor Neuron Facial Nerve Palsy as a Presenting Sign in COVID-19 Associated Orbital Mucormycosis Patients: A Retrospective Observational Study
Purpose: The main purpose of this study is to emphasize that isolated facial nerve involvement can be the first presenting symptom in patients suspected of COVID-associated Mucormycosis (CAM). Methods: This study is a retrospective observational study conducted at a tertiary care referral center which included patients with a history of CAM, who presented with isolated facial nerve palsy as initial presentation between March 2021 to March 2022 along with their follow-up. All the patients were managed with combined modality treatment with antifungal therapy and debridement of the necrotic tissue and fungal debris. Results: There were 184 eyes of 148 patients diagnosed with CAM. All patients developed rhino-orbital mucormycosis (ROM) following the COVID-19 infection and the duration between diagnosis of COVID-19 and ROM was 36±23 days. 42(28%) patients presented with isolated Facial Nerve Palsy (FNP) as the initial presentation. The mean age was 48.5 years (range 38 to 67years) with a male predominance of 29 (69%). All were unilateral cases and were of Lower motor neuron type presentation. All the patients (100%) were treated with systemic Liposomal amphotericin-B and sinus debridement. At a mean follow-up of 13.1 months, 19 (45%) of the patients had improvement in Facial Nerve function and 23 (55%) had static functioning. None of them had worsened. With medical intervention and tarsorrhaphy, the corneal condition was improved in all patients. Conclusion: Isolated FNP is an unusual but important sign in the presentation of mucormycosis which can be misdiagnosed with a cerebrovascular accident leading to delay in the management. This is a large case series with isolated FNP in CAM cases. A high index of suspicion for mucormycosis in diabetic patients presenting with isolated facial palsy can save the life and salvage the eye.
Introduction
Although Mucormycosis is rare it leads to serious angioinvasive infection caused by a group of fungi of the order Mucorales. It mainly affects people with diabetes (60- 81%), those with a history of transplantation, malignancy, raised levels of ferritin, prolonged hospitalization, long term steroid use [1, 2, 3, 4]. Second wave of COVID-19 was associated with the sudden rise in Mucormycosis cases. Worldwide, the prevalence of CAM ranged from 0.005 to 1.7 per million people and India alone was having a prevalence of approximately 80 times greater (0.14 per 1000) than other countries [5]. This may be because India has one of the highest populations of diabetes in the world [6]. CAM patients mainly present with headache, periocular swelling, nasal stuffiness, bleeding from the nose, and rarely with a deviation of mouth or improper closure of the eyelid. Early diagnosis of CAM is difficult and requires a high index of suspicion. The main pathogenic mechanism for Rhino Orbital Mucormycosis (ROM) is inhalation and inoculation of spores of the fungus on the middle or inferior turbinate. Then by angioinvasion or contiguous involvement, it spreads to the sinuses, pterygopalatine fossa, and orbit. If the orbital apex is involved then it leads to the involvement of the II, III, IV, VI, and Vth cranial nerves [7]. Involvement of the Facial Nerve in its Lower Motor Neuron (LMN) segment is rare to see and is also difficult to explain. Facial nerve palsy has been reported among diabetic patients with CAM in 11% to 40% of cases [8, 9].
Material and Methods
A retrospective case review was done for COVID-19 associated mucormycosis at a tertiary care institute in India from March 2021 to March 2022 along with their follow-up. The study was approved by the institute’s ethical committee. All patients who had presented with isolated facial palsy were included in the study. The diagnosis of mucormycosis was confirmed by visualization of aseptate or pauciseptate fungal hyphae, with right-angled branching, on tissue biopsy with direct potassium hydroxide (KOH) mount or culture or histopathological examination. Cases were considered COVID-19 associated if the patient received a positive Reverse Transcription Polymerase Chain Reaction or Antigen test result for SARS-CoV-2 during the 60 days preceding the mucor diagnosis [7]. The clinical and demographical details were noted. Contrast-enhanced computed tomography (CT) or contrast-enhanced magnetic resonance imaging (MRI) of the brain, orbits, and Para nasal sinuses. A thorough clinical history, ocular examination, and examination of cranial nerves were done for each patient. Patients with pre-existing Facial Nerve palsy or facial soft tissue involvement if mimicking Facial Palsy were excluded. Motor and sensory functions of the facial nerve were done to confirm seventh nerve palsy.
At the primary position, asymmetry of facial expression, absence of nasolabial fold, facial deviation, lagophthalmos, and presence of ectropion, were noted. Different muscle groups supplied by the seventh nerve were examined by asking the patient to forcibly close the eyes for orbicularis by zygomatic branch; wrinkling of the forehead for frontalis action by temporal branch; pouting their cheeks, showing teeth for buccinators and zygomaticus by buccal branches; forcefully depress and draw inferior lip laterally by marginal mandibular and tense the skin of the anterior neck for the cervical branch to the platysma. ICMR and institutional- guided COVID protocol was maintained during the study. Data were analyzed using standard statistical software.
Results
There were 184 eyes of 148 patients diagnosed with CAM. All patients developed ROM following the COVID-19 infection and the duration between diagnosis of COVID-19 and ROM was 36±23 days. 42(28%) of patients presented with isolated FNP as the initial presentation. The mean age was 48.5 years (range 38-67years). There was a male predominance of 29(69%) and females were 13(31%). All were unilateral and were of Lower motor neuron type presentation. 32(76%) of the study population were known diabetics and 10(24%) had developed new onset diabetes. The newly diagnosed diabetic patients had a history of systemic steroid use for more than 2 weeks. All patients had isolated FNP at the initial presentation. Most of the patients had grade 6 of House Brackmann facial nerve palsy 29(69%) (Figure 1) and the rest 13(31%) had grade 5 palsy (Figure 2) [10].

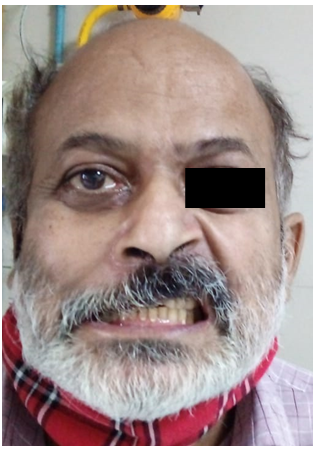
Table 1 summarises the ocular features of FNP. Other cranial nerve examination was within normal limits. Radiological evaluation showed all of the patients (100%) had Nose and Para nasal sinus involvement. All the patients underwent surgical debridement and concomitant medical therapy with Liposomal Amphotericin B. Lateral Tarsorraphy was done in 34(81%) cases. At a mean follow-up of 13.1 months, 19(45%) of the patients had improvement in Facial Nerve function and 23(55%) had static functioning. None of them had worsened. With medical intervention and tarsorrhaphy, the corneal condition was improved in all patients.
| Males 29(69%) | Female 13(31%) | |
|---|---|---|
| Loss of Vision | 14(48%) | 5(38%) |
| Ptosis | 23(79%) | 9(69%) |
| Right Side FNP | 15(52%) | 8(62%) |
| Left Side FNP | 14(48%) | 5(38%) |
| Corneal involvement | 12(41%) | 6(46%) |
| Sub conjunctival haemorrhage | 05(17%) | 03(23%) |
| Central Retinal Artery Occlusion | 14(48%) | 5(38%) |
Table 1: Distribution of signs in Bell’s palsy. Loss of vision was attributed to central retinal artery occlusion in that eye.
Discussion
Mucormycosis is an opportunistic infection that can be fatal, especially in patients with diabetes mellitus and those on long-term systemic steroids. The pathophysiology of mucormycosis involves inhalation of spores followed by germination of these spores forming hyphae that invade the blood vessels, leading to thrombosis and hence causing ischemia [11]. The ischemia leads to the formation of the black necrotic Escher on which the fungus feeds and spreads to the palate, orbit, and brain via arteries and can present with abscess, meningitis, or cavernous sinus thrombosis [1]. The actual cause of facial nerve palsy and its pathology is unknown. Typically these patients present with headache, Swelling, or pain in the face and as the disease progresses they may present with ptosis, loss of vision, proptosis, multiple cranial nerve palsy, or eschar formation [12, 13]. Various explanations have been given by different authors. The pterygopalatine fossa is considered to be a mucor reservoir from which mucor can extend to the orbital apex, retro-orbit, and infratemporal space. It can also spread via the bony erosion of the infratemporal fossa causing damage to the seventh nerve exiting the stylomastoid foramen [12]. Some authors postulate that they can migrate along peripheral nerves due to the proximity of the pterygopalatine fossa to the brain [14]. Another hypothesis is that it can be incidental and nonspecific or can spread via a Eustachian tube [15].
However, none of the patients presented to us with ear problems. Isolated involvement of the facial nerve can occur if the nerve sheath of the intracanalicular facial nerve within the temporal bone gets involved [16] or in people with diabetes, localized facial nerve ischemia can happen [17]. Our mean age was 48.5 years with a male predominance of 69%. This was similar to the study done by Rupa Mehta, et al. where the mean age was 48 years with male predominance [18]. This was also similar to the study done by Rajashri Mane, et al. where the mean age was 50.75 years and male predominance [1]. This was different from Das, et al. [7] who had 72% female predominance. This difference may be because of the place and small sample size. Of all patients in our study 32(67%) were pre-diabetic and 10(33%) have developed new-onset diabetes. This was similar to the study done by Mehta and Mane, et al. [1, 18]. New-onset diabetes cases were higher in a study done by Gautam, et al. where 16 out of 30 cases had new-onset diabetes [19]. However, this was different from Das, et al. where 54% were diabetics [7]. The study has done by Reddy, et al. have shown 95% to be newly diagnosed diabetics [20]. This difference may be because they have considered all cases of CAM with and without FNP. All patients in our study had unilateral isolated lower motor neuron FNP. This can be due to angioinvasive and neurotropic nature of the mucormycosis. Our study had 42 patients coming with isolated FNP as primary presentation compared to 4 patients in the study by Das, et al. [7], and 4 patients with FNP and other cranial nerve involvement in a study done by Jaiswal, et al. [21]. Both males and females in our study have shown more right-sided facial palsy. This is similar to the study done by Reddy, et al. [20]. Table 2 compares the different studies on FNP presentation.
| Year | Author, et al. | No. of patients with Facial Palsy | Mean age of presentation (years) | Isolated FNP | Combined with other nerves | Improvement in FNP | Stable FNP | Death |
|---|---|---|---|---|---|---|---|---|
| 2013 | Sachdeva [22] | 6 | 52 | 0 | 100% | 66% | NA | 33.30% |
| 2019 | Mane [1] | 4 | 50 | 50% | 50% | 50% | NA | 50% |
| 2021 | Gautam [19] | 30 | 45 | 27% | 73% | 0 | 100% | 0 |
| 2022 | Reddy [20] | 53 | 47 | 0 | 100% | NA | NA | 0 |
| 2023 | Das [7] | 11 | 50 | 18.20% | 81.80% | 54.50% | 9.10% | 0 |
| 2023 | Current Study | 42 | 48 | 100% | 0 | 45% | 55% | 0 |
Table 2: Different studies on FNP presentation.
Conclusion
Mucormycosis is a lethal angioinvasive opportunistic infection. Timely diagnosis and intervention are most crucial for patients’ survival especially strict control of glucose levels. Rarely, they can manifest as isolated facial palsy as initial presentation masquerading as cerebrovascular accident. Our main aim is to emphasize that isolated facial palsy can be the initial presentation in mucormycosis cases. A high index of suspicion for mucormycosis in diabetic patients presenting with facial palsy can save the life and salvage the eye. Further study is needed to find the cause of isolated facial nerve palsy in mucormycosis cases.
Declaration of Patient Consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial Support and Sponsorship
Nil
References
-
Mane R, Patil B, Mohite A, Mohanty R (2019) Facial Nerve Palsy: An Unusual Presentation in Patients with Rhino Cerebral Mucormycosis. Indian J Otolaryngol Head Neck Surg 71(3): 2110-2113.
-
Singh AK, Singh R, Joshi SR, Misra A (2021) Mucormycosis in COVID-19: A systematic review of cases reported worldwide and in India. Diabetes Metab Syndr 15(4): 102146.
-
Bhansali A, Bhadada S, Sharma A, Suresh V, Gupta A, et al. (2004) Presentation and outcome of rhino-orbital- cerebral mucormycosis in patients with diabetes. Postgrad Med J 80(949): 670-674.
-
Cohen SG, Greenberg MS (1980) Rhinomaxillary mucormycosis in a kidney transplant patient. Oral Surg Oral Med Oral Pathol 50(1): 33-38.
-
Kanika, Sharma N, Yadav A, Kumar P (2023) Effectiveness of facial palsy protocol among patient with mucormycosis following COVID-19: A case study. Heliyon 9(2): e13209.
-
Shekar V, Sikander J, Rangdhol V, Naidu M (2015) Facial nerve paralysis: A case report of rare complication in uncontrolled diabetic patient with mucormycosis. J Nat Sci Biol Med 6(1): 226-228.
-
Das SK, Barman D, Samaddar S, Chatterjee P, Mondal AR, et al. (2023) New Onset Facial Nerve Palsy : A Part of Post COVID Mucormycosis Disease Spectrum- A Descriptive Observational Study. Journal of the Indian Medical Association 121(1): 28-32.
-
Bakshi SS (2016) An unusual cause for facial nerve palsy: mucormycosis. International Journal of Diabetes in Developing Countries 4(36): 385-388.
-
Dubey S, Mukherjee D, Sarkar P, Mukhopadhyay P, Barman D, et al. (2021) COVID-19 associated rhino-orbital- cerebral mucormycosis: An observational study from Eastern India, with special emphasis on neurological spectrum. Diabetes Metab Syndr 15(5): 102267.
-
House JW, Brackmann DE (1985) Facial nerve grading system. Otolaryngol Head Neck Surg 93(2): 146-147.
-
Hosseini SMS, Borghei P (2005) Rhinocerebral mucormycosis: pathways of spread. Eur Arch Otorhinolaryngol 262(11): 932-938.
-
Song YM, Shin SY (2008) Bilateral Ophthalmic Artery Occlusion in Rhino-Orbito-Cerebral Mucormycosis. Korean J Ophthalmol 22(1): 66-69.
-
Singh NP, Garg S, Kumar S, Gulati S (2006) Multiple cranial nerve palsies associated with type 2 diabetes mellitus. Singapore Med J 47(8): 712-715.
-
Spellberg B, Edwards J, Ibrahim A (2005) Novel perspectives on mucormycosis: pathophysiology, presentation, and management. Clin Microbiol Rev 18(3): 556-569.
-
Munir N, Jones NS (2007) Rhinocerebral mucormycosis with orbital and intracranial extension: a case report and review of optimum management. J Laryngol Otol 121(2): 192-195.
-
Bhattacharyya AK, Deshpande AR, Nayak SR, Kirtane MV, Ingle MV (2012) Rhinocerebral Mucormycosis: an Unusual Presentation. American Journal of Medicine and Medical Sciences 2(1): 16-19.
-
Mutsukura K, Tsuboi Y, Imamura A, Fujiki F, Yamada T (2004) Garcin syndrome in a patient with rhinocerebral mucormycosis. No To Shinkei 56(3): 231-235.
-
Mehta R, Nagarkar NM, Ksbs KS, Sree Sudha Ty, Arora RD, et al. (2021) Facial Nerve Palsy in COVID-19-Associated Mucormycosis Patients: A Case Series. Cureus 13(11): e19208.
-
Gautam M, Soni M, Bhaisare V, Rawat P, Walia S, et al. (2022) Complete and incomplete lower motor neuron facial palsy in post-COVID-19 mucormycosis. Indian J Ophthalmol 70(4): 1365-1370.
-
Reddy YM, Goddanti N, Kumar K, Suresh A, Muderla R, et al. (2022) Facial Nerve Palsy as a Common Presentation during the Epidemic of Coronavirus Disease Associated Rhinocerebral Mucormycosis. Indian J Otolaryngol Head Neck Surg 74(2): 3313-3320.
-
Jaiswal AS, Sikka K, Bhalla AS, Manchanda S, Goel G, et al. (2022) Facial neuritis in coronavirus disease 2019 associated mucormycosis: study on clinico-radiological correlates. J Laryngol Otol 136(4): 349-353.
-
Sachdeva K (2013) Rhino-oculo Cerebral Mucormycosis with Multiple Cranial Nerve Palsy in Diabetic Patient: Review of Six Cases. Indian J Otolaryngol Head Neck Surg 65(4): 375-379.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report