Retinopathy of Prematurity: Risk Factors, Recent Trends of Screening and Outcome of Treatment in a Tertiary Care Eye Hospital of Bangladesh
Objectives: To determine the associated risk factors, current methods of screening and treatment outcome of ROP in a tertiarylevel eye hospital in Bangladesh. Methods: A prospective longitudinal study was conducted in the OPD, Pediatric care unit of a tertiary eye hospital, among 167 babies from October 2014 to June 2019. The initial examination was done either at four weeks of birth or 31 weeks post-conceptually, whichever was earlier. After taking consent, a detailed history was taken. Before the fundus examination, mydriasis was achieved, and indirect ophthalmoscopy was done under topical anesthesia. In favorable cases, staging of ROP was done with subsequent follow-up. As per ETROP indication, either laser photocoagulation or anti-vascular endothelial growth factor (anti-VEGF) injection or both were given for treatment. Later these babies were followed up to see the outcome. Results: Out of 167 babies, we had two groups after the 1st screening; 76 babies (45.5%) fell in the ROP group and 91 babies in the No ROP group. On subsequent screening, 28 babies had spontaneously regressed ROP, leaving 48 in the ROP group who required treatment. The male gender was predominant in both groups (52.6% and 56.04%, respectively). Type 1 ROP was the most prevalent. Oxygen therapy (93.4%) of variable duration and neonatal jaundice (52.6%) were the top two risk factors of ROP in this study. Sixty-five babies (38.9%) fell into a group of birth weight 1000-1500 grams, and 81 (48.5%) had a gestational age of 28-32 weeks. As a treatment, the majority with ROP (21 cases) received laser therapy. In the final follow-up, refractive errors are the most common outcome after treatment of ROP. Conclusion: The available care for ROP varies, and visual disability is mainly preventable when detected and treated in time. With limited resources and expertise, the screening and treatment of ROP implemented in Bangladesh showed some satisfactory outcomes; a longer follow-up would give a more detailed evaluation of the impact of this treatment on the visual status.
Introduction
The World Health Organization has identified retinopathy of prematurity (ROP) as an emerging cause of childhood blindness. It has become a significant public health problem due to the increased survival of preterm babies as increasing numbers and facilities of NICUs and Special Newborn Care Units are opening worldwide. Retinopathy of prematurity (ROP) is a Vaso-proliferative disorder of the retina, which principally occurs in premature children during vascular development and maturation. It was first identified by T.L. Terry TL in 1942 in the USA, and he named it retrolental fibroplasia [1]. In many cases, it may undergo spontaneous regression or progress to blindness. If detected early and timely intervention is done, blindness is mainly preventable. Several studies suggested that oxygen therapy is not the only causative factor, but ROP is a multifactorial disorder, having various risk factors, including prematurity, low birth weight, oxygen therapy, sepsis, blood transfusion, respiratory distress syndrome (RDS), failure to thrive, hyperbilirubinemia etc [2, 3, 4, 5, 6]. Increased the incidence of ROP worldwide due to the better survival rate of low birth weight and preterm babies availing modern neonatal facilities and care. As the baby and attendant can never complain about any symptoms until it is too late, it is the health system’s responsibility and professionals’ responsibility to prevent its development (monitored oxygen therapy, sepsis control, minimal transfusion etc.), detection (screening of high-risk babies) and treatment.
Effective screening and treatment programs have been shown to reduce blindness in children from ROP in many high- income countries. Nonetheless, it remains a significant cause of blindness in many low and middle-income countries. Lawn, et al. noted that there are 15 million infants born each year prematurely, with 1.2 million born in high-income countries with access to complete neonatal intensive care, another 8.2 million born in middle-income or low-income countries with access to hospital births but perhaps in hospitals with limited space, staff, and equipment, and 5.6 million born in low-income countries with home birth and care at home and therefore a limited chance of survival [7]. This study aimed to evaluate the associated risk factors predisposing to ROP and the screening procedures in a tertiary eye care center of a developing country. It also attempted to find out the long-term outcome of those treated either with laser photocoagulation with anti-vascular endothelial growth factor injection or both.
Materials and Methods
A prospective longitudinal study was conducted from October 2014 to June 2019 among 167 babies referred to the Outpatient department (OPD) of the Pediatric care unit of Bangladesh Eye Hospital for ROP screening from a consultant pediatrician/neonatologist who worked in NICU and managed them previously. The initial screening of the neonate was done either at four weeks of birth or 31 weeks post-conceptually, whichever was earlier. Ethical clearance was obtained from the hospital committee, and informed consent from the parents was also obtained. Birth Weight (BW) and gestational age (GA) at birth were noted from medical history and stratified into different groups to determine the incidence of ROP in different BW and GA. A detailed history, including the history of any neonatal complications, such as apnoea/RDS, oxygen requirement, sepsis, hyperbilirubinemia, twinning/multiple pregnancy, and exchange transfusion/use of any blood products, were recorded from their previous hospital discharge note and were considered to be risk factors for ROP according to previous studies [2, 3, 8, 9]. The screening was done with a binocular indirect ophthalmoscope with a +20D lens under topical anesthesia with the help of a pediatric speculum and scleral indentation. Before the fundus examination, mydriasis was achieved with 0.5% tropic amide and 2.5% phenylephrine eye drops, instilled three times at 10 minutes intervals. In favorable cases, staging of ROP was done according to the international classification [8, 9, 10]. All the infants were screened by the same ophthalmologist.
Infants with normal vascularization up to the periphery were not examined again. Those with ROP were examined every week. Treatment was given according to the Early Treatment of Retinopathy of Prematurity Randomized Trial study [10, 11]. The improved results of visual outcomes with initial treatment are recommended by the Early Treatment of Retinopathy of Prematurity Study (ETROP) as follows (Tables 1 & 2):
| Type 1 | Zone | Plus |
|---|---|---|
| ROP 1 or 2 or 3 | I | + |
| ROP 3 | I | - |
| ROP 2 or 3 | II | + |
Table 1: (Severe pre-threshold ROP): Treatment with laser/ anti-VEGF in an expert center.
| Type 2 | Zone | Plus |
|---|---|---|
| ROP 2 or 3 | I | - |
| ROP 2 or 3 | II | - |
Table 2: (Less severe ROP): Careful observation.
Laser therapy was done using an 810 nm red laser (index SLx) with indirect laser ophthalmoscope as early as possible, at least within seven days of diagnosis of threshold plus disease. This was done under topical anesthesia, using an infant wire speculum and scleral indentation in an OT setting. The avascular retina beyond the ridge was ablated using confluent medium-intensity burns over one session. Topical treatment with tobramycin and dexamethasone was given for five days, and an oral analgesic was given for one day. If regression was found inadequate or skip areas were seen on subsequent examination, laser therapy was repeated after one or two weeks. Injection Avastin (anti- vascular endothelial growth factor) therapy was used as the primary treatment or before using laser treatment. All ROP babies were asked to come for regular follow-ups on the 2nd - 4th day and then on the 7th day to check for any adverse effects and the regression of ROP. Follow-ups were planned and scheduled according to the location and severity of ROP for up to 40 weeks. They were again called for a detailed ophthalmic examination at the age of 1 year and two years. After the collection, all data analysis was done using SPSS version 22 (Figure 1).
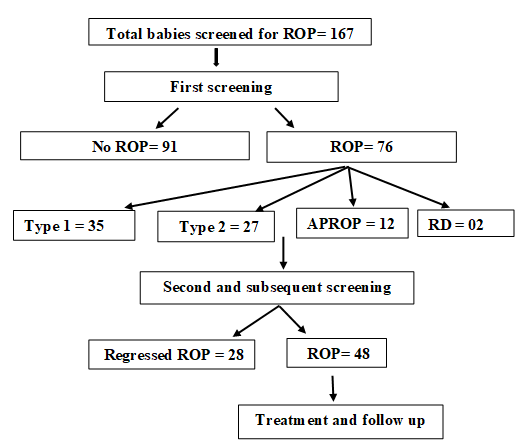
Results
In this study, out of 167 babies, we had two groups, where 76 babies (45.5%) fell in the ROP group and 91 babies in the No ROP group after the 1st screening. On subsequent screening, 28 babies were found to have regressed ROP, leaving 48 in the ROP group who required treatment. The male gender was predominant in both groups (52.6% and 56.04%, respectively). Distribution of the neonatal conditions that contributed as risk factors of ROP for this study population showed (Table 3) that 71 babies (93.4%) in the ROP group needed oxygen therapy for a variable length of the period (range: 11-32 days). Among other risk factors, 41.1% of babies who had different stages of ROP had neonatal sepsis, and 52.6% had neonatal jaundice. 23.7% of babies had been suffering from respiratory distress syndrome/Apnoea that developed ROP. Twinning in 13.2% and transfusion in 3.9% of babies was found in the ROP group. All these factors were statistically significant (χ2 test done, p-value <0.04 or less).
| Variables | Studied babies with ROP at 1st screening. (N=76) | Studied babies without ROP at 1st screening. (N=91) | P value (χ2 test done |
|---|---|---|---|
| Gender: Male | 40 (52.6%) | 51 (56.04%) | 0.048 |
| Female | 36 (47.4%) | 40 (43.96%) | |
| Neonatal complications | |||
| RDS/apnoea | 18 (23.7%) | 14 (15.4%) | 0 |
| Sepsis | 32 (42.1%) | 20 (22%) | 0 |
| Hyperbilirubinemia | 40 (52.6%) | 28 (30.8%) | 0 |
| O therapy 2 | 71 (93.4%) | 66 (72.5%) | 0 |
| BT/ET | 03 (3.9%) | 0 | 0 |
| Twinning | 10 (13.2%) | 7 (7.69%) | 0.001 |
Table 3: Baseline characteristics of study population (n=167). RDS= respiratory distress syndrome; BT=Blood transfusion; ET=Excha
Among the 167 babies, 65 (38.9%) fell into the birth weight group of 1000-1500 grams (Table 4), and 81 (48.5%) had a gestational age of 28-32 weeks (Table 5). The mean birth weight was 1260 gm, and the median was 1620.23 gm (ranging from 800 gm to 2700 gm). The mean gestational age was 32.63 weeks, and the median was 33.92 weeks (ranging from 26 to 40 weeks). As expected from previous studies, low birth weight and prematurity had a significant relationship with ROP in this study (p-value <0.05).
| Weight Group (grams) | Stages of ROP at 1st screening | |||||
|---|---|---|---|---|---|---|
| Type 1 | Type 2 | APROP | RD | No ROP | Grand Total | |
| <1000 | 4 | 1 | 2 | 1 | 6 | 14 |
| 1000-1500 | 17 | 16 | 6 | 1 | 25 | 65 |
| >1501-2000 | 9 | 8 | 2 | 0 | 38 | 57 |
| 2001-2500 | 5 | 2 | 1 | 0 | 14 | 22 |
| >2500 | 0 | 0 | 1 | 0 | 8 | 9 |
| Total | 35 | 27 | 12 | 2 | 91 | 167 |
Table 4: Distribution of studied babies by birth weight (n=167). *p- value .034; RD= Retinal detachment.
| Gestational age groups (weeks) | Stages of ROP at 1st screening | |||||
|---|---|---|---|---|---|---|
| Type 1 | Type 2 | APROP | RD | No ROP | Grand Total | |
| <28 | 5 | 5 | 1 | 1 | 6 | 18 |
| 28-32 | 24 | 11 | 8 | 0 | 38 | 81 |
| 33-36 | 6 | 11 | 3 | 1 | 44 | 65 |
| 37-40 | 0 | 0 | 0 | 0 | 3 | 3 |
| Total | 35 | 27 | 12 | 2 | 91 | 167 |
Table 5: Distribution of studied babies by gestational age (n=167). *p-value 0.18.
subsequent screening, it was revealed that among 76 ROP screen-positive babies at 1st visit, 28 had spontaneous regression and ultimately needed no treatment.
Regarding treatment, a total of 21 cases (19 ROP babies had been given laser in both eyes. in one case, the laser was given in the R/E, and another case, it was applied in the L/E. Of 48 ROP infants, 05 needed injection Anti-VEGF (Inj.
Avastin given in both eyes of 03 and eye of 02 cases). A total of 03 cases needed surgical intervention, and the rest of the 19 infants had the injection and laser therapy (Table 6).
| Treatment | Right eye | Left eye | Both eyes | Total |
|---|---|---|---|---|
| Diode laser | 1 | 1 | 19 | 21 |
| VEGF inhibitor injection | 1 | 1 | 3 | 5 |
| VEGF inhibitor injection plus Laser | 0 | 0 | 19 | 19 |
| Surgery | 0 | 0 | 3 | 3 |
| Total | 2 | 2 | 44 | 48 |
Table 6: Distribution of the ROP babies according to a type of treatment (n=48).
The final follow-up (Table 7) demonstrated the outcome of treated ROP babies. Refractive errors occurred in 21 children (Myopia in 16 and Hypermetropia in 05 babies), and 03 cases remained Emmetropic at their last visit within this study period. CSM (Central, Steady and Maintained fixation) was found in 12 (25%), Squint/ misalignment in 03 (6.25%), Cataract, Astigmatism and Nystagmus in 02 (4.17%) cases each and blindness was found in 01 (2.08%). Two (02) cases were reported to be lost from follow-up in the middle of this study after two visits, and a laser vitrectomy was done.
| Eye condition at final F/Up | Laser therapy and Avastin injection | |
|---|---|---|
| Number | Percentage (%) | |
| Refractive error | ||
| Myopia | 16 | 33.33% |
| Hypermetropia | 5 | 10.42% |
| Emmetropia | 3 | 6.25% |
| Astigmatism | 2 | 4.17% |
| Squint/misalignment | 3 | 6.25% |
| CSM (Central, Steady and Maintained fixation) | 12 | 25% |
| Nystagmus | 2 | 4.17% |
| Blindness | 1 | 2.08% |
| Cataract | 2 | 4.17% |
| Lost from follow-up | 2 | 4.17% |
Table 7: Outcome of ROP babies after treatment at final follow-up (n=48).
Discussion
This study was conducted in a tertiary-level hospital among 167 babies referred for ROP screening. Since ROP is essentially asymptomatic in the early stages, standards of practice now demand carefully timed retinal examination of at-risk infants by an experienced ophthalmologist. There are varying screening criteria and methods. This study demonstrated the screening methods of ROP in a tertiary eye hospital in Bangladesh were comparable with international screening guideline [3]. Prematurity and LBW are two independent risk factors in developing ROP in neonates. Many studies have proven the relationship between low meagre birth weight and the occurrence of ROP [4, 12, 13, 14, 15]. Usually, babies with 1250 grams or less and born before 31 weeks gestation are at the highest risk, as was also seen in our study. Though gender did not significantly influence the incidence, a slight male predominance was seen in the present study. Many risk factors have been reported to predispose to the development of ROP: oxygen therapy, anaemia, blood product/exchange transfusion, septicemia, apnea, and hyperbilirubinemia are important risk factors [14, 15, 16]. In our study, oxygen administration, neonatal jaundice, sepsis, apnea/RDS and transfusion- were all significant risk factors. Aggarwal, et al. [14] also found apnea, clinical sepsis, and male sex to be significant risk factors. Vinekar, et al. [15] also found that septicemia was a significant risk factor.
Laser photocoagulation has gained widespread acceptance, largely replaced cryotherapy, and is currently the standard of care for treating ROP. Ng EY, et al. [17] and Connolly, et al. [18] have reported that long-term structural and functional outcome using a laser was superior to cryotherapy, and favorable results were obtained in nearly 83% of eyes treated with laser. We found that most ROP cases were treated using a laser in our study. Few
case reports and a large trial (Bevacizumab reducing the angiogenic threat of Retinopathy of Prematurity: BEAT- ROP Trial) have demonstrated the benefits of anti-vascular endothelial growth factor (inj. Avastin) therapy when used as the primary treatment or before using laser treatment as per need in the regression of stage 3/zone I ROP with no adverse events [19, 20, 21]. The BEAT-ROP trial was the most extensive study examining anti-VEGF therapy to date. This study enrolled 150 infants with Zone I or Zone II posterior stage 3 ROP and randomly assigned each to receive bilateral intravitreal bevacizumab or laser photocoagulation, with a primary outcome measure being the need for retreatment before 54 weeks GA. The recurrence rate in Zone I disease was significantly higher with laser therapy (42%) than with intravitreal bevacizumab (6% recurrence rate). The present study also showed a promising result with the use of intravitreal injection of anti-vascular endothelial growth factor in 19 cases in a combination of laser therapy. Our limitation was not being able to compare the outcome measure of laser and Avastin separately in this setting.
Regarding the outcome after treatment of ROP, the most significant (21 cases among 48) ocular problem observed was refractive errors, among the others like a squint, nystagmus etc. Without timely and proper correction, these errors may lead to the development of a lazy eye that ultimately will cause low vision if not identified in time, hindering the overall purpose of ROP screening and treatment. So, longer follow-up and proper correction of these errors are critical. Another significant outcome of treated ROP could be cataracts (though only 4.17% were found in our study); iatrogenic cataract development after laser or intravitreal injection could be detected in long-term follow-up when cataract extraction can restore vision.
Conclusion
In developing countries such as Bangladesh, our babies suffer more because of suboptimal neonatal care, lack of awareness and not-in-place/ improper screening and treatment programs. Suppose the awareness can be improved for referral for ROP screening in recognized equipped centers, and after diagnosing the actual picture, treatment with laser or injection anti-VEGF in time can be given by experts. In that case, it will reduce the burden of blindness, as we have shown in our results. A longer follow- up will give a more detailed evaluation of the impact of ROP treatment on the visual status of children.
References
-
Terry TL (1942) Extreme prematurity and fibroblastic overgrowth of persistent vascular sheath behind each crystalline lens. Preliminary report. American J Ophthalmol 25(2): 203-204.
-
Akter S, Parvin R, Yasmeen BHN, Anwar KS, Hossain MM (2014) Association of infection, blood transfusion and other clinical factors with retinopathy of prematurity (ROP). Northern International Medical College Journal 5(2): 325-328.
-
Hardy RJ, Palmer EA, Dobson V, Summers CG, Phelps DL, et al. (2003) Risk analysis of prethreshold retinopathy of prematurity. Arch Ophthalmol 121(12): 1697-1701.
-
Blencowe J, Lawn JE, Vazquez T, Fielder A, Gilbert C (2013) Preterm associated visual impairment and estimates of retinopathy of prematurity at regional and global level for 2010. Pediatr Res 74 Suppl 1(1): 35-49.
-
Rekha S, Battu RR (1996) Retinopathy of prematurity: incidence and risk factors. Indian Pediatr; 33(12): 999- 1003.
-
Shohat M, Resiner SH, Krikler R, Nissenkorn I, Yassur Y (1983) Retinopathy of prematurity: incidence and risk factors. Pediatr 72(2): 159-163.
-
Lawn JE, Davidge R, Paul VK, Xylander SV, Joseph DGJ, et al. (2013) Born Too Soon: Care for the preterm baby. Reprod Health 10(1): S5.
-
Schaffer DB, Palmer EA, Plotsky DF, Metz HS, Flynn JT, et al. (1993) Prognostic factors in the natural course of retinopathy of prematurity. The Cryotherapy for Retinopathy of Prematurity Cooperative Group. Ophthalmology 100(2): 230-237.
-
Fierson WM (2018) American Academy of Pediatrics Section on Ophthalmology. Screening Examination of Premature Infants for Retinopathy of Prematurity. Pediatrics 142(6): e20183061.
-
An international classification of retinopathy of prematurity. II. The classification of retinal detachment. The International Committee for the Classification of the Late Stages of Retinopathy of Prematurity(1987). Arch Ophthalmol 105(7): 906-912.
-
William VG, Early Treatment for Retinopathy of Prematurity Cooperative Group (2004) “Final results of the Early Treatment for Retinopathy of Prematurity (ETROP) randomized trial.” Transactions of the American Ophthalmol Society 102: 233-248.
-
Wilkinson AR, Haines L, Head K, Fielder AR (2008) UK retinopathy of prematurity guideline. Early Hum Dev 84(2): 71-74.
-
Palmer EA, Flynn JT, Hardy RJ, Phelps DL, Phillips CL, et al. (1991) Incidence and early course of retinopathy of prematurity. Ophthalmology 98(11): 1628-1640.
-
Aggarwal R, Deorari AK, Azad RV, Kumar H, Talwar D, et al. (2002) Changing profile of retinopathy of prematurity. Trop Pediatr 48(4): 239-242.
-
Vinekar A, Dogra MR, Sangtam T, Narang A, Gupta A (2007) Retinopathy of prematurity in Asian Indian babies weighing greater than 1250 grams at birth: ten years data from a tertiary care center in a developing country. Indian J Ophthalmol 55(5): 331-336.
-
Dutta S, Narang A, Dogra MR, Gupta A, Narang S (2004) Risk factors of threshold retinopathy of prematurity. Indian Pediatr 41(7): 665-671.
-
Fierson WM (2013) Screening examination of premature infants for retinopathy of prematurity. Pediatrics 131: 189-195.
-
Ng EY, Connolly BP, McNamara JA, Regillo CD, Vander JF, et al. (2002) A comparison of laser photocoagulation with cryotherapy for threshold retinopathy of prematurity at 10 years. Part 1-Visual function and structural outcome. Ophthalmology 109(5): 928-934.
-
Connolly BP, Ng EY, McNamara JA, Regillo CD, Vander JF, et al. (2002) A comparison of laser photocoagulation with cryotherapy for threshold retinopathy at 10 years. Part 2- Refractive outcome. Ophthalmology 109(5): 936- 941.
-
Mantagos IS, Vanderveen DK, Smith LE (2009) Emerging treatments for retinopathy of prematurity. Seminars in ophthalmology 24(2): 82-86.
-
Hittner HAM, Kennedy KA, Chuang AZ, Group BRC (2011) Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med 364(7): 603- 615.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report