Ultrasound-Guided Rectus Abdominis Sheath Block in Cats Undergoing Ovariectomy: A Prospective, Randomized, Investigator-Blinded, Placebo-Controlled Clinical Trial
Objective: To evaluate the analgesic effects of an ultrasound-guided rectus abdominis sheath block performed with lidocaine and bupivacaine, in cats undergoing midline ovariectomy. Study design: Randomized, prospective, placebo-controlled, investigator-blinded clinical trial. Animals: Forty-one client-owned female cats scheduled for ovariectomy were enrolled in the study and randomly assigned to one of the treatment groups. Methods: Both treatment and control groups received general anesthesia and a bilateral rectus abdominis sheath block (RSB) under ultrasound guidance. The block was performed with 0.05 mL kg-1of 2% lidocaine and 0.15 mL kg-1 of 0.5% bupivacaine mixed together in each rectus abdominis sheath (group A) or the equivalent volume of saline (group B). Intraoperative pain assessment was based on changes in physiological parameters compared to the baseline values and rescue analgesic requirement. Postoperative pain assessment was performed using the 4A-Vet pain scale and the need for rescue analgesics at 1, 2, 4 and 6 hours after extubation. The sedation was evaluated and graded at the same times. The owners were asked to fill a questionnaire at three time points: the night the cat was back home, the next morning and ten days after the surgery. Results: There were two significant differences between group A and B: less isoflurane was needed in group A during the suturing phases (p = 0.04 during peritoneal muscular sutures and 0.02 during skin suture) and cats from group A were less sedated 6 hours after extubation (p = 0.03338). Conclusions and clinical relevance: In summary, our study concludes that ultrasound-guided RSB decreases the amount of isoflurane used during surgical closing time and the sedation score 6 hours after extubation. The block was easily and successfully performed. Further studies are needed to adjust the local anesthetic volume and prove its long-term efficacy in cats.
Introduction
Cats are the most common pets in France with a population of 11.2 million. Moreover, 77.2% of French cats are neutered [1]. Therefore, neutering has become a commonly undertaken elective procedure. However, laparotomy in female cats is a major and painful surgery.
Pain in cats has been identified commonly as less treated than in dogs. For instance, a French survey showed that the use of opioids was significantly lower in cats compared to dogs [2]. Local anesthesia is of prime importance in the multimodal approach to control per-operative pain. Indeed, it is the only way to completely stop the progression of the nociceptive message. Furthermore, local anesthesia allows reducing the utilization of systemic analgesics and general anesthetics, and their side effects [3, 4]. The efficacy of blocks during ovariectomy has been proven. For example, one study in cats undergoing ovariectomy indicated that anesthesia requirements were significant lowered in the group with lidocaine infiltration in the skin, on both ovaries and in the abdominal muscles [5].
The rectus abdominis sheath block (RSB) is a local anesthetic technique that works by “diffusion” of the local anesthetic to adjacent nervous structures into the rectus abdominis muscle sheath. RSB has been used in human anesthesia for years and is especially useful in pediatric anesthesia, to reduce nociceptive influx during abdominal surgery. Its efficacy has been showed in several studies by sparing analgesic uses after abdominal surgery in children and women in acute and chronic pain situations [6, 7, 8, 9, 10]. In addition, the safety of RSB is suggested to be high since the potential complications such as small bowel or major vessel puncture, hematoma or an infection of the injection site rarely occur [10, 11, 12].
In human medicine, the RSB provides dense and predictable analgesia over the middle anterior wall from the xiphoid process to the symphysis pubis. It is therefore used for surgery with midline (or paramedian) abdominal incision. Analgesia however does not extend to the lateral abdomen [13]. The RSB has been described in a cadaveric canine study [14], was deemed easy to perform and to have the potential to provide effective analgesia of the abdominal wall in the ventral midline area. In the feline species, the RSB targets the nerves that have ramifications ending in the rectus abdominis muscle sheath, ie the last intercostal, the costoabdominal, the cranial ioliohypogastric, the caudal iliohypogastric and the ilioinguinal nerves [15].
The ovariectomy is a source of acute peroperative pain [3, 16], is a widely performed surgical procedure in veterinary medicine and commonly used as a surgical standardized model of abdominal pain [5, 17, 18, 19]. The aim of the study was to evaluate the feasibility and the usefulness of the RSB in alleviating nociceptive responses in cats undergoing ovariectomy, performed by midline laparotomy, as well as the sparing effect of isoflurane and the post-operatively pain behavior.
Material and Methods
The study was approved by the institutional ethical committee for veterinary epidemiological and clinical research of Oniris National College of Veterinary Medicine, Food Science and Engineering.
Study population
The study was conducted as a prospective, randomized study. The principal investigator was unaware of the group allocation. A total of 41 client-owned intact female cats admitted to Oniris Veterinary Teaching Hospital for routine ovariectomy were enrolled in the study. All cat owners signed an informed client consent form. Inclusion criteria for entering the trial were cats less than 6 years old with an estimated anesthesia risk ASA 1. Upon admission, a thorough clinical examination was performed. Randomization was done by paper drawing by the anesthetist that performed the block but he did not participate thereafter to patient evaluation.
Anesthesia and Analgesia
An intramuscular (IM) premedication with 20 µg kg-1 of medetomidine (Medetor, Virbac, France) and 0.3 mg kg-1 of morphine IM (Morphine, Laboratoire Aguettant, France) in the same 1 mL syringe mounted on a 25-gauge needle (T0) was administered in the semitendinosus muscle. Cats were kept in a calm environment for 15 minutes before the abdomen was clipped from the last rib to the cranial line of the pubis and 3 cm on left and right side of the umbilicus. After a surgical scrub with chlorhexidine soap and solution, the RSB was performed on the cats positioned in dorsal recumbency with 0.05 mL kg-1 lidocaine 2% (1 mg kg-1, Xylocaine, Astra Zeneca, France) and 0.15 mL kg-1 bupivacaine 0.5% (0.75 mg kg-1, Chlorhydrate de bupivacaine, laboratoire Aguettant, France) per side for the group A or the equivalent volume of saline solution for the group B. The RSB was performed under ultrasound-guidance according to technique description in humans and dogs [13, 14]. A linear array 12.5 MHz ultrasound transducer was placed transversally on the abdomen midway between the last rib and the umbilicus to identify rectus abdominis muscles on both sides of the linea alba. The probe orientation was adjusted to facilitate visualization of a hyperechoic sheath wall [14]. The target points of injection were identifiable as the two bilateral hypoechogenic spaces dorsal the two symmetrical strips of the rectus abdominis muscles and ventral to the hyperechoic deep layer of the sheath. A 23-gauge 15 mm needle mounted on a 1 mL syringe was introduced 0.5 cm proximally to the transverse line crossing the umbilicus, approximatively in the median muscle plane with a 30-degree angle to the skin, directed dorsocranially using an out of plane approach one side after the other. The distribution of the solution was observed during the injections that were all done by the same experienced anesthetist, investigator aware of the treatment allocation but not involved in the animal evaluations. The injection success was objectified with the apparition upon slow injection of an anechoic area in the rectus abdominis sheath dorsally to the muscle and ventrally to the peritoneum (Figure 1). Failure was either a partial IM injection within the belly of the rectus abdominis muscle, or an inappropriate depth of injection reaching the peritoneal cavity.
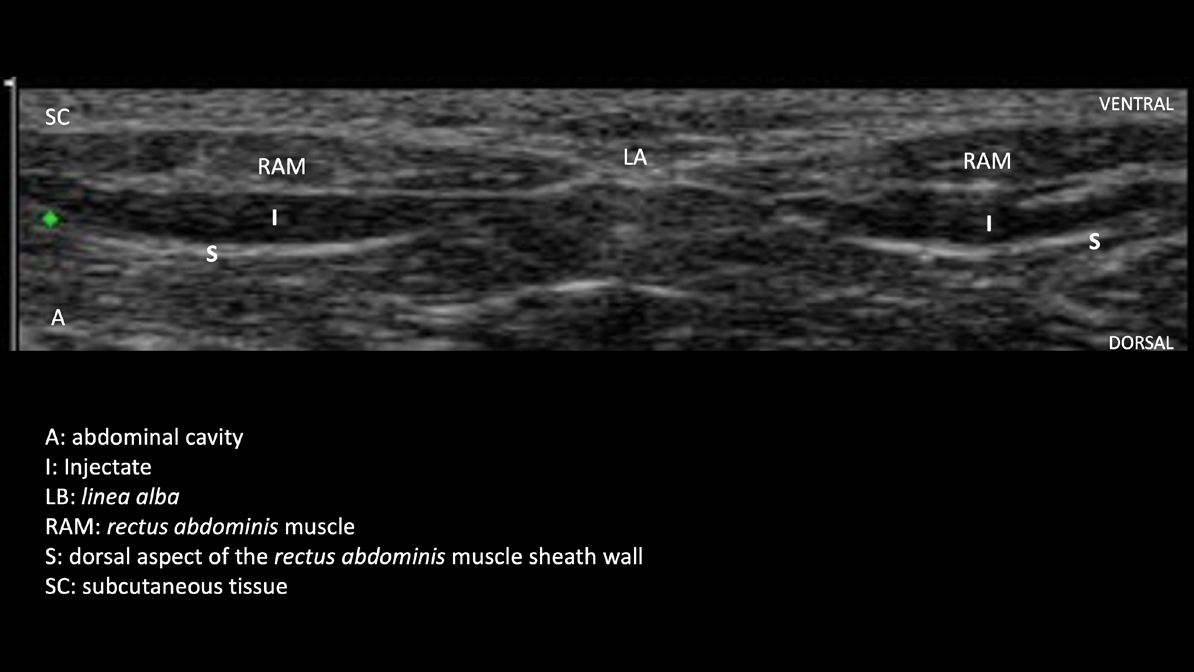
Figure 1: Ultrasound image (transverse section) of the abdominal wall after the successful performance of the RSB: bilateral anechoic areas in the sheath dorsally to the muscle and ventrally to the peritoneum (A: abdominal cavity, I: Injectate, LB: linea alba, RAM: rectus abdominis muscle, S: dorsal aspect of the rectus abdominis muscle sheath wall, SC: subcutaneous tissue).
Following the RSB, a 22-gauge intravenous catheter was inserted in the cephalic vein and anesthesia was induced with propofol 2-4 mg kg-1 IV to effect (Propovet, Axience, France). To facilitate intubation, 0.1 mL lidocaine 2% (Xylocaine, Astra Zeneca, France) was applied on the larynx. A cuffed endotracheal tube with an internal diameter range of 3.0 to 4.0 mm depending on size of cat was used. Anesthesia was maintained with isoflurane (Isoflo, Axience France) vaporized in oxygen administered using a Bain breathing system (flow rate of 200 mL kg-1min-1 with a minimum of 1 Lmin-1). All cats were placed in dorsal recumbency and Lactated Ringer solution (Virbac, France) was administered IV at a rate of 5 mL kg-1 h-1. At T25 (25 minutes after premedication), cats received subcutaneously (SC) 2 mg kg-1 robenacoxib (Onsior, Novartis, France).
Physiological parameters were recorded at several steps during the surgery: before skin incision, during skin incision, during the first ovary handling, during the second ovary handling, during abdominal wall suture and during skin suture. Clinical signs of anesthesia depth, body temperature, pulse rate (pulse oximetry with a tongue probe), non-invasive arterial pressure (Doppler method, Flow detector 811.BL; Parks Medical Electronics, OR, USA), respiratory rate, end- tidal CO2 (EtCO2) and end-tidal isoflurane (Etiso) (side-stream capnography system and gas analyzer) were monitored with a multiparameter monitor (S/5 patient monitor, GE/ Datex Ohmeda, General Electric Healthcare). Anesthesia was monitored by veterinary students supervised by a clinician, both blind to the study randomization. Rescue analgesia consisted of 0.05 mg kg-1 morphine IV boluses, not exceeding a total dose of 0.5 mg kg-1 and was to be administered if a sudden increase greater than 20% was witnessed in the heart or respiratory rate or Doppler blood pressure. The isoflurane concentration could also be adjusted following the response to rescue analgesia and reassessment of anesthesia depth signs.
Anesthesia recovery and follow up
At the end of the surgery, isoflurane administration was discontinued and cats given oxygen at an inspired fraction of 100% during 10 minutes. Medetomidine was reversed with 12.5 µg kg-1 of atipamezole IM (Antisedan, Zoetis, France) once body temperature was above 37°C and if swallowing or head movements had not returned at this time. If the cat was still not awake 15 minutes after the first injection, a second dose was administered. Exubation time was recorded and determined the beginning of the recovery time.
Postoperatively, pain was evaluated 1, 2, 4 and 6 hours after extubation by one same investigator unaware of treatment allocation. Pain score was evaluated with the 4A-Vet pain scale [20] and transformed in pain levels: Level 1 is equivalent to a score from 1 to 5 and level 2 from 6 to 10 [21]. If the pain score was above 6, morphine (0.05 mg kg-1) was injected IV. During those four examinations during recovery, body temperature (rectal thermometer), heart rate (stethoscope), respiratory rate (observation), sedation score (modified Young’s sedation scale, Le Berre 2008.) [22] were monitored. Systematically, 20 µg kg-1 buprenorphine IM (Vetergesic, CEVA and France) were administered 6 hours after extubation before hospital discharge. Oral meloxicam 0.05 mg kg-1 once a day (Metacam, Boehringer France) was given for the subsequent 3 days.
The owners were asked to fill a questionnaire at three time points: the night the cat was back home, the next morning and ten days after the surgery. Global behavior, play behavior, interest for the surgical wound, appetite, return to normal bowel function and diuresis as well as owner satisfaction concerning pain control of their cat were gathered. Questionnaire was designed by compiling items from 2 sources translated in French: the Cat Assessment Tool for Cardiac Health [23] and the Feline Acute Pain Scale from Colorado State University Veterinary Medical Center. Those data were collected by phone by the same clinical investigator, unaware of the cat allocation to group A or B.
Surgery
The ovariectomy was performed by veterinary students teamed by pair: a student in his last year of study (fifth year) and a fourth-year student. The protocol was standardized: skin 3 to 5 cm incision caudal to the umbilicus; smooth dissection of sub-cutaneous connective tissue; puncture of the linea alba and incision with a groove probe; exploration and prehension of one ovary; ligature of anterior and posterior vascular areas: puncture of the broad ligament, set up of hemostatic clips, set up of ligatures; removal of the ovary; checking of the hemostasis; exploration and prehension of the second ovary; surgical removal just as the first one ; sutures of abdominal muscles and peritoneum with simple stitches in cross ; skin suture with an intradermal pattern.
Statistical analysis
Statistical analyses were performed using statistical software package R® (R Core Team, Austria, 2014). Each variable was initially tested for normality and within-cat correlations. Depending on the results, an ANOVA test for repeated measures or a Kruskall-Wallis test was used for quantitative variables. Qualitative variables were analyzed with Fisher’s exact test. Regarding data measured on the same animals several times, a mixed effects model analysis was performed. A p-value less than or equal to 0.05 was considered to be significant. Parametric data are presented as mean ± SD.
Results
Seventeen cats in the group A and 19 in the group B completed the study. In total, five cats from the initial forty- one included cats (four from group A and one from group B) were excluded as three of them were tattooed after the ovariectomy and the pain caused by the tattoo may have influenced the evaluation of RSB effectiveness. One cat was not brought to its surgical appointment and one cat became excited after medetomidine reversal that precluded clinical assessment during recovery. The groups were comparable with respect to mean age (A: 8 ± 2.5 months, B: 12.5 ± 15 months), weight (A: 2.97 ± 0.65 kg, B: 2.99 ± 0.74 kg), preoperative heart rate (A: 172 ± 20 bpm, B: 179 ± 31 bpm), preoperative respiratory rate (A: 53 ± 19 mpm, B: 51 ± 21 mpm), hematocrit (A: 33 ± 3 %, B: 34 ± 2 %), total blood proteins (A: 62 ± 5 g L-1, B: 65 ± 4 g L-1), duration of both anesthesia (A: 94 ± 18 min, B: 92 ± 16 min) and surgery (A: 58 ± 16 min; B: 69 ± 14 min), as there were no significant statistical difference between the two groups.
Feasibility of RSB
During the whole trial, 83 % of RSB injection were successfully performed, ie the local anesthetics were accurately injected into the rectus abdominis sheath under ultrasonographic guidance. Moreover, after the twenty- fourth injections, all RSB were successful. No intraperitoneal injection was witnessed. The time between the premedication and the anesthesia induction (which included sedation and RSB injections done by the clinician aware of the treatment allocation and IV catheter placement done by students) was on average 44 ± 9 minutes in the group A and 51 ± 17 minutes in the group B.
Anesthetic variables
The average dose of propofol for both groups was 3.1 mg kg-1 (A: 3.0 ± 1.1; B: 3.2 ± 0.7 mg kg-1). The two groups were not different with regards to heart rate, blood pressure, respiratory rate and body temperature, SpO2 and EtCO2. Results are presented in Table 1. A trend of having higher Etiso in the placebo group was identifiable as soon as the first ovary manipulation and isoflurane concentrations were statistically different during the last two times of surgery (1.29 ± 0.17% in group A and 1.22 ± 0.19% in group B, ie - 9.7 % during abdominal wall sutures, p-value=0.04; 1.22 ± 0.19% in group A and 1.4 ± 0.24% in group B, ie - 12.7 % during skin suture, p-value=0.02). A post-hoc power study revealed a power of 83% for the significant difference in the Etiso between group A and B. An average of less than one bolus of morphine was used for each cat in both groups during the surgery with no statistical difference between groups (A: 0.6 ± 0.5 bolus, B: 0.3 ± 0.6 bolus). Three cats per group received 12.5 µg kg-1 atipamezole with no significant statistical difference between group A and group B.
| Variable | Before skin incision | During skin incision | Manipulation of the first ovary | Manipulation of the second ovary | Suture of abdominal wall | Skin suture |
|---|---|---|---|---|---|---|
| Temperature Group A (°C) | 37.3±0.6 | 37.1±0.7 | 36.7±0.8 | 36.4±0.7 | 36.3±0.8 | 36.3±0.8 |
| Temperature Group B (°C) | 37.2±0.4 | 36.8±0.5 | 36.4±0.5 | 36.2±0.7 | 36.2±0.6 | 36.4±0.6 |
| Heart rate (bpm) Group A | 113±14 | 118±14 | 150±19 | 162±24 | 147±17 | 130±19 |
| Heart rate (bpm) Group B | 110±14 | 112±15 | 150±20 | 152±18 | 143±19 | 135±19 |
| Respiratory rate (mpm) Group A | 28±9 | 23±7 | 25±7 | 23±10 | 20±10 | 18±6 |
| Respiratory rate (mpm) Group B | 26±10 | 21±9 | 24±11 | 23±10 | 22±11 | 20±10 |
| Arterial blood pressure (mmHg) Group A | 90±16 | 84±15 | 111±22 | 122±21 | 98±20 | 89±10 |
| Arterial blood pressure (mmHg) Group B | 91±13 | 88±17 | 103±13 | 117±21 | 93±20 | 87±12 |
| SpO (%) 2 | 97±2 | 97±2 | 96.4±2 | 96±3 | 96±2 | 96±2 |
| Group A | ||||||
| SpO (%) 2 | 97±1 | 96±2 | 97±2 | 96±3 | 97±3 | 97±2 |
| Group B | ||||||
| EtCO (mmHg) 2 | 32±8 | 33±8 | 34±8 | 35±8 | 36±9 | 36±9 |
| Group A | ||||||
| EtCO (mmHg) 2 | 31±9 | 33±10 | 33±10 | 30±10 | 32±10 | 34±12 |
| Group B | ||||||
| Etiso(%) | 1.22±0.10 | 1.26±0,14 | 1.27±0.19 | 1.32±0.17 | 1.29±0.17a | 1.22±0.19a |
| Group A | ||||||
| Etiso (%) | 1.16±0.21 | 1.21±0.21 | 1.38±0.22 | 1.4±0.20 | 1.43±0.22b | 1.4±0.24b |
| Group B |
Table 1: Intraoperative variables expressed as mean ± SD in Group A and group B (placebo) at the different surgical times. Bpm: B
Postoperative evaluations
Three cats in each group were at the pain level 2 one hour after extubation and received a rescue morphine dose. Four of those six cats were back to level 1 one hour later. The remaining two animals in group A and one in group B that were still on level 2 two hours after extubation received a second IV rescue dose of morphine. No cats were in level 2 four and six hours after extubation. There was no significant statistical difference between the two groups in terms of pain score or rescue analgesia. Cats with a 4A-Vet pain score above 6 looked significantly more sedated than cats with a pain score under 5 one hour and two hours after extubation (p-value = 0,046 and 0,0009). Cats from Group A were significantly less sedated than cats from Group B six hours after extubation (p-value = 0.03338). All owners answered the questionnaires at the three time points. Owners responded that their cat was comfortable and calm in 71% (A) and 58% (B) 2 hours following home return, 76% (A) and 68% (B) the following morning, 94% (A, 16 cats out of 17) and 100% (B) 10 days after the surgery. Seven cats (2 in group A and 5 in group B) presented a deterioration of their behavior (less interaction, avoiding touch, tiredness) the day following home return. Playful behavior was reported in 41% (A) and 68% (B) of the cases upon home return, 71% (A) and 58% (B) the following morning and 100% at 10 days. However, no difference in the behavior occurrences was found statistically significant between the groups. Finally, nearly 90% of the cats in both groups ate voluntarily upon home return.
Discussion
This study investigates the effectiveness of the RSB as part of a multimodal perioperative pain management in cats undergoing ovariectomy by midline laparotomy. First, the RSB was successfully performed within a relatively short period of time. Although the exact duration needed to perform the block was not measured, the time that elapsed from the IM premedication to the anesthesia induction was mainly due to waiting time for the sedation to take place (10-15 min), the animal transfer to the ultrasound room and back to the induction station and the IV catheter placement by veterinary students. The 17% of injection failure were due to a partial injection in the rectus abdominis muscle. This inaccuracy was corrected by the anesthetist who succeeded in all injections after 24 implementations (12 cats). The study confirmed that ultrasonography was helpful for block performance, as well as its accuracy and safety: reduction of the probability to inject anesthetics in an improper space, reduction of the time required to perform the block and of the onset time [10, 11, 24]. To compare, in human medicine, one study highlighted that 89% of injections were successfully done with ultrasonography, only 45% without of which 21% were improperly injected into the peritoneal cavity [24].
The choice of the combination of lidocaine and bupivacaine was based on their pharmacodynamics: the lidocaine ensures a quick and brief effect, relayed by the bupivacaine which has a long-lasting effect but a longer onset time. This combination has been recommended in previous studies in veterinary medicine [4]. The choice of the local anesthetic volume was based on data from the human medicine literature [8, 13, 25] and was less than the volumes tested in dog cadavers (St James et al., 2020)[14]. A larger volume may have provided a more pronounced and prolonged analgesia that could have been seen during surgery and in recovery.
The difference between the two groups is relatively tenuous with regard to all parameters monitored during and after anesthesia (significant lower Etiso during suture and lower sedation score 6 hours after extubation). As pain treated by the RSB is exclusively somatic (abdominal wall), pain due to ovary stimulation, which constitutes the most painful step of the procedure, is not prevented by the RSB [4, 5, 19]. During the surgical wound suture, the Etiso was significantly reduced in the group A compared to the group B (-9.7% during muscular suture and -12.7% during skin suture). This reduction could be linked to a substantial comfort brought by the RSB.
The analgesia provided by the protocol was multimodal and considered profound, with the combination of an α-2 agonist agent, an opioid, a non-steroidal anti-inflammatory drug and the local block or placebo. Therefore, the intensity of analgesia may have precluded from singling out the effect of the block. Fitzpatrick suggests that when the pain is reduced to a very low level, it is not possible to bring a biological difference between two groups [19]. Cardiovascular and respiratory stability during the surgical procedure showed the efficacy of the analgesic protocol. Intraoperative heart rate stayed below 150 bpm, average arterial blood pressure below 120 mmHg and respiratory rate below 22 mpm. There was a tendency of an increase in the cardiovascular and respiratory variables during the surgery, which could be related to the surgical stimulation between baseline data taken before the surgery start and after during the application of the surgical stimulation. On average, less than one intravenous morphine bolus was administered in both groups. During the postoperative period, morphine was used in only 16.7 % of cats one hour after extubation and 8.3 % of cats two hours after extubation. For obvious ethical reasons, a group without systemic analgesia was not recruited.
Other local anesthesia techniques during ovariectomy have shown similar effects on the anesthetic requirements. For example, a study using only an opioid as premedication (Savvas et al. 2008)[4] was able to show a positive effect of a preoperative infiltration of bupivacaine in dogs undergoing midline laparotomy. The study showed a significant reduction of the postoperative pain scores and rescue analgesia needs. As for the study led by Zilberstein, the lidocaine was used for an infiltration of the surgical wound, on the ovaries and on the muscle of the abdomen and allowed to reduce the need for injectable anesthetics during the surgery.
The RSB needs more time to be performed and more training from the anesthetist compared to a subcutaneous infiltration, ovaries and abdominal muscles used in other studies [4, 5]. Upon having the ultrasound machine available in the induction room to streamline the procedure, the block is easy to perform: simple anatomical landmark easily identified on ultrasound, rapid probe positioning on the abdominal wall with bilateral injections done with the same probe placement, only 2 injections. Although the use of RSB and transversus abdominis plane (TAP) block provides complementary analgesia, the RSB technique accessibility with a reduced number of injections has been opposed to the more difficult and multi-injections TAP block [12, 13, 14]. Moreover, the RSB has a very low probability of systemic effects due to low risk of intravenous injection, reduced local anesthetics volume and limited systemic absorption.
The choice of cats undergoing ovariectomy with a midline laparotomy may not discriminate test and control groups sufficiently. Assessing pain in cats is a real challenge [3, 26, 27]. A French survey indicated that over half of responding veterinarians considered that their analgesic use was adequate in canine patients; this figure was significantly lower in cats [2]. Remaining effects of sedation in recovery may render difficult pain assessment in cats. This is the reason why medetomidine reversal with a low dose of atipamezole was included in the protocol in order to mitigate the variability of recovery among the cats. However, medetomidine reversal also decreases the analgesic coverage. The reversal was therefore only done if cats were not showing rapid signs of awakening. Only a few cats received it. It constitutes a study limit due to lack of standardization and it may have interfered with pain evaluation after recovery. One could also argue that painful cat can show signs of sedation and that reversal may have contributed to differentiate sedation due to the anesthesia protocol or pain in the early recovery period [17]. Interestingly, cats looked less sedated at the 6-hour recovery time in the RSB group compared to the placebo which could be interpreted as less pain in the local anesthetic group.
Questionnaires filled by owners were an original feature of the study. The reduction of the perioperative pain during surgery was expectedly challenging to highlight because the RSB does not target the visceral pain, which is the main source of pain during the procedure. As no power study was done prior using the questionnaire, it is possible that group size was a limit to achieve statistical differences. The questions may have not been discriminant enough to identify signs of pain by owners. A control group of cats brought to the hospital but not receiving anesthesia or undergoing a surgical procedure would have been interesting to follow to see how this event changes behavior upon return to home. More work is needed to refine the questionnaire and extract relevant information.
Conclusion
This study showed that performing a RSB under ultrasonographic guidance in cats is relatively easy. The block allows sparing some anesthetic agents during the surgical closing time. Moreover, cats with RSB were evaluated less sedated and more comfortable during the postoperative period. However, the choice of healthy cats undergoing ovariectomy may not be the most discriminant surgical model to highlight the efficacy of RSB. First, the cat is a challenging species for pain evaluation. Then, the ovariectomy creates an acute surgical pain whereas RSB has been shown to be particularly efficient to treat chronic pain in human. The original feature of this study was the cat behavior evaluation by the owner once the cat was backing home.
Conflict of Interest Statement
None of the authors have any financial or personal relationships that could inappropriately influence or bias the content of this article.
Acknowledgements and Funding
The authors thank Oniris Veterinary Teaching hospital for supporting this study.
References
-
FACCO/TNS Soffres (2012) La population animale- Enquête.
-
Hugonnard M, Leblond A, Keroack S, Cadoré JL, Troncy E (2004) Attitudes and concerns of French veterinarians towards pain and analgesia in dogs and cats. Vet Anesth Analg 31(3): 154-163.
-
Mathews K, Kronen PW, Lascelles D, Nolan A, Robertson S, et al. (2014) WSAVA Guidelines for recognition, assessment and treatment of pain. J Small Anim Pract 55(6): E10-68.
-
Savvas I, Papazoglou L, Kazakos G, Anagnostou T, Tsioli V, et al. (2008) Incisional block with bupivacaine for analgesia after celiotomy in dogs. J Am Anim Hosp Assoc 44(2): 60-66.
-
Zilberstein L, Moens Y, Leterrier E (2008) The effect of local anaesthesia on anaesthetic requirements for feline ovariectomy. Vet J 178(2): 212-216.
-
Fu H, Fu Y, Xu X, Gao Y (2020) Ultrasound-Guided Rectus Sheath Block Combined with Butorphanol for Single- Incision Laparoscopic Cholecystectomy: What is the Optimal Dose of Ropivacaine? J Pain Res 13: 2609-2615.
-
Hamill JK, Liley A, Hill AG (2015) Rectus sheath block for laparoscopic appendicectomy: a randomized clinical trial. ANZ J Surg 85(12): 951-956.
-
Crosbie E, Massiah N, Achiampong Y, Dolling S, Slade R (2012) The surgical rectus sheath block for post- operative analgesia: a modern approach to an established technique. European Journal of Obstetrics & Gynecology and Reproductive Biology 160(2): 196-200.
-
Dingeman R, Barus L, Chung H, Clendenin D, Lee C, et al. (2013) Ultrasonography-guided bilateral rectus sheath block vs local anesthetic infiltration after pediatric umbilical hernia repair: a prospective randomized clinical trial. J Am Med Assoc Surg 148(8): 707-713.
-
Willschke H, Bosenberg A, Marhofer P, Johnston S, Kettner S, et al. (2006) Ultrasonography-guided rectus sheath block in paediatric anesthesia - a new approach to an old technique. Br J Anaesth 97(2): 244–249.
-
Kim WJ, Mun JY, Kim HJ, Yoon SH, Han SR, et al. (2021) Surgical rectus sheath block combined with multimodal pain management reduces postoperative pain and analgesic requirement after single-incision laparoscopic appendectomy: a retrospective study. Int J Colorectal Dis 36(1): 75-82.
-
Kimura F, Oishi M, Yakoshi C, Ogasawara C, Ishihara H, et al. (2013) Rectus sheath block and transversus abdominis plane block for a patient with Lambert- Eaton myasthenic syndrome undergoing low anterior resection. Masui 62(8): 989-991.
-
Webster K (2014) Ultrasound guided rectus sheath block – analgesia for abdominal surgery. Update in Anesthesia. pp: 6.
-
St James M, Ferreira TH, Schroeder CA, Hershberger- Braker KL, Schroeder KM (2020) Ultrasound-guided rectus sheath block: an anatomic study in dog cadavers. Vet Anaesth Analg 47(1): 95-102.
-
Done SH, Goody P, Evans S, Stickland N (2009) Color atlas of veterinary anatomy Vol 3 The dog and cat. (2nd edition) Mosby, St Louis Mi USA, pp: 527.
-
Muir W, Hubbell J, Bednarski R, Lerche P (2014) Handbook of Veterinary Anesthesia. 5th(Edn.) Elsevier Mosby, St Louis Mi USA, pp: 600.
-
Brondani J, Luna S, Padovani C (2011) Refinement and validation of a multidimensional composite scale for use in assessing acute postoperative pain in cats. Am J Vet Res 72(2): 174-183.
-
Carpenter R, Wilson D, Evans A (2004) Evaluation of intraperitoneal and incisional lidocaine or bupivacaine for analgesia following ovariohysterectomy in the dog. Vet. Anaesth Analg 31(1): 46-52.
-
Fitzpatrick C, Weir H, Monnet E (2010) Effects of infiltration of the incision site with bupivacaine on postoperative pain and incisional healing in dogs undergoing ovariohysterectomy. J Am Vet Med 237 (4): 395-401.
-
Freeman LM, Rush JE, Oyama MA, MacDonald KA, Cunningham SM, et al. (2012) Development and evaluation of a questionnaire for assessment of health- related quality of life in cats with cardiac disease. J Am Vet Med Assoc 240(10): 1188-1193.
-
Association Vétérinaire pour l’Anesthésie et l’Analgésie Animales (2014) 4A-Vet pain scale for cats.
-
Verwaerde P, Estrade C (2005) Vade-mecum d’anesthésie des carnivores domestiques. 1st(Edn.), Editions Med’Com., Paris France. pp : 255.
-
Le Berre K (2008) Comparaison de trois protocoles de contention chimique dans l’espèce féline. Thèse de doctorat vétérinaire, Ecole nationale Vétérinaire de Toulouse, Université Paul Sabatier de Toulouse pp: 52.
-
Ludot H (2012) Blocs de la paroi abdominale : apports de l’échographie. Annales françaises d’anesthésie et de réanimation 31(1): e21-e24.
-
Gurnaney H, Maxwell L, Kraemer F, Goebel T, Nance M, et al. (2011) Prospective randomized observer-blinded study comparing the analgesic efficacy of ultrasound- guided rectus sheath block and local anesthetic infiltration for umbilical hernia repair. Brit J Anaesth 107(5): 790-795.
-
Merola I, Mills DS (2016) Behavioural signs of pain in cats: an expert consensus. PLoS One 11(2): 1-15.
-
Steagall PV, Monteiro BP (2019) Acute pain in cats: Recent advances in clinical assessment. J Feline Med Surg 21(1): 25-34.
- The Digital Stethoscope: Harnessing AI in Veterinary Medicine Without Losing Our Healing Touch
- Meningoencephalomyelitis of Unknown Etiology: Short-Term Effect of Two Treatment Protocols on Cerebrospinal Fluid
- Safety and Efficacy of the HomeoPet Cough in Domestic Pets –A Clinical and Correction Analysis Based Upon User Response Survey
- Non Human Animals Responses to Social Loss
- Owner Reported Clinical Outcomes of a Homeopathic Proprietary Preparation for the Treatment of Upper Respiratory and Nasal Disorders in Companion Animals
- Effects and Diagnostic Approach of Ultrasound in Veterinary Practice: A Systematic Review