Temporary Application of a Tarsal Arthrodesis Plate as a Postoperative Immobilization Technique in Common Calcaneal Tendon Injury Repair in Dogs: A Pilot Study
Objective: To determine if the temporary application of a pantarsal arthrodesis plate would provide adequate postoperative tarsal immobilization after calcaneal tendon repair and to identify complications compared to an established technique. Study Design: This was a single institution retrospective pilot study. Medical records of dogs from January 2008 through September 2019 that presented for common calcaneal tendon injury and underwent surgical repair were reviewed. Exclusion criteria included cases that had incomplete medical records or had insufficient follow up. 17 calcaneotibial (CT) screw and 10 temporary tarsal arthrodesis plate (TTAP) cases were included in the final analysis. Data collected included signalment, pertinent history, injury type, surgical technique, duration of postoperative immobilization, major postoperative complications that warranted a second procedure, and follow up time. Results: The major complications in the CT screw group were tendon re- injury (n=5), surgical site infection (n=1), and tendon laxity (n=1). The major complication in the plate group was tendon laxity (n=1). The median follow up time after initial surgery was 171 (range 36-1670) and 185 (range 57-567) days for the CT screw and TTAP groups, respectively. Conclusion: The results from this pilot study suggest that a TTAP is an acceptable method for postoperative immobilization after primary calcaneal tendon repair. Further research is warranted to validate this procedure.
Carolyn Chen1, Grayson Cole2* and Wayne Whitney3
Introduction
Injuries to the common calcaneal tendon (CCT) in dogs can be debilitating. Composed of 5 major muscles (gastrocnemius, superficial digital flexor, gracilis, semitendinosus, and biceps femoris), the CCT is under a considerable amount of tension, compounding a naturally long recovery time. While there is no data evaluating the healing process of the CCT specifically, a predicted path of healing akin to those of other canine tendons is extrapolated from the literature. Studies have shown that the canine triceps tendon, at 6 weeks and 1 year post injury, has 56%
and 79% of the original strength respectively recovered [1]. Surgical repair and management of tendon injury aim to oppose the tendon ends and prevent subsequent distraction during the long period of tendon healing [2]. Commonly used postoperative immobilization techniques for primary calcaneal tendon repair include calcaneotibial screw fixation in conjunction with external coaptation [3, 4], external skeletal fixation [5, 6] and external coaptation devices [7]. Several retrospective studies have demonstrated complications associated with each immobilization technique. A retrospective study evaluating largely the use of trans-articular external skeletal fixators (ESF) reported an 18% major complication rate including metatarsal fracture, osteomyelitis secondary to the ESF pins, implant failure that required revision of the fixator, and tendon laxity after the ESF was removed. The same study reported complications for patients that had external coaptation such as bandaged induced dermatitis or wounds and splint breakage (8). Another retrospective study involving 45 dogs with CCT injury investigated postoperative complications associated with the placement of a calcaneotibial (CT) screw. The authors reported a 35% complication rate, including implant failure, or screws that were loose at the time of removal, but had not caused any apparent morbidity [9]. No significant functional difference among immobilization techniques has been demonstrated in the current veterinary literature [8, 10]. Due to the complication rate associated with standard immobilization techniques, there is a clinical need for a technique which affords appropriate stability with minimal patient morbidity.
With this need in mind, the authors started to investigate the use of a temporary tarsal arthrodesis plate (TTAP) as an alternative postoperative immobilization technique. There were several potential advantages that were considered with this method. The plate could offer a more robust fixation than the CT screw, and would not demand as much at-home care as an external fixator. The plate could also decrease the risk of bandage morbidity that is often associated with traditional external coaptation methods. Lastly, the TTAP could ensure that the joint could be fixed at a functional angle, allowing the tendon to heal in the appropriate anatomical position. By avoiding prolonged hyperextension (as the leg is often positioned in after CT screw placement), the concern for superficial digital tendon contracture can also be mitigated. While this complication has not been documented in the current literature, the authors have anecdotally seen this clinically affect patients who had their limbs in hyperextension after primary calcaneal tendon repair. The purpose of this pilot study was to investigate the placement of a TTAP as an alternative technique for postoperative stabilization after primary CCT repair. The authors hypothesized that there was no significant difference in major complications between dogs receiving the CT screw and dogs receiving a TTAP for post-operative immobilization.
Materials and Methods
Study Procedures
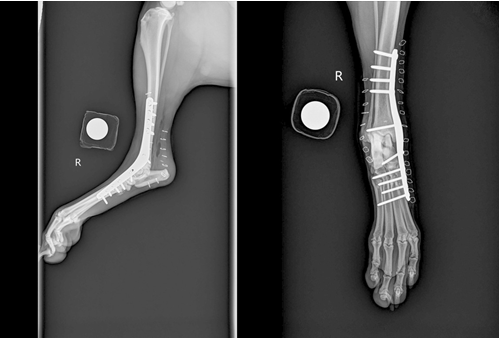
Medical records of dogs from January 2008 through September 2019 that presented for partial or complete common calcaneal tendon rupture were reviewed. Inclusion criteria included cases that had primary surgical repair of the calcaneal tendon with medical records complete through surgical explant. Cases were excluded if they had incomplete medical records or were ongoing (i.e. explant surgery had not occurred yet). Of the 29 dogs that met the inclusion criteria, 17 had a CT screw placed, and 10 had a TTAP placed. Data collected included signalment, pertinent history, injury type, surgical technique, type of implant, duration of postoperative immobilization, duration of follow up, and major postoperative complications. A major postoperative complication was defined as a complication in which a revision surgery was recommended. For all cases, the primary tendon repair was performed at the surgeon discretion. Postoperative immobilization methods were also at the surgeon’s discretion, depending on what technique they believed would best suit the patient. Patients that potentially had excess tension on the repair site or had increased amount of tendon debridement were excluded from receiving a TTAP. The dogs that received a CT screw had the procedure performed as previously described [3, 11]. Explant of the screw was planned to be 6-8 weeks postoperatively. External coaptation with a bandage and plantolateral splint following screw placement was recommended to be maintained until 2 weeks post-explant for a total of 8-10 weeks. For dogs that received a TTAP, a standard medial approach to the tarsus was made to place the implant [12]. The implant was placed on the medial aspect of the tarsus as previously described with some aspects of the procedure modified [2]. Articular cartilage was not debrided, and the medial malleolus was not ostectomised, in order to preserve the medial collateral ligament and the medial aspect of the talocrural joint. The plate was contoured to fit over the malleolus, and secured with a combination of cortical and locking screws according to the surgeon’s discretion. Orthogonal radiographs were taken to ensure appropriate placement of the implant prior to recovery from general anaesthesia. The dogs were placed in external coaptation with a bandage and plantolateral splint for two weeks following the initial surgery; the remainder of the period prior to explant, the dogs did not have any form of external coaptation. It was recommended for the plate to be explanted 8 weeks postoperatively and the patient to be replaced in a bandage and plantolateral splint for an additional 2 weeks post-explant procedure. All dogs were to gradually return to normal activity over 6-8 months after removal of external coaptation 2 weeks post-explant.
Statistical Analysis
Continuous variables were assessed for normality using Shapiro Wilk tests. The median and range were reported for non-normally distributed continuous variables. Commercially available statistical software was used to calculate statistics.
Results
Of the 27 cases, 16 dogs were male, and 11 were female. The mean age in both the TTAP and CT screw groups was 6 years old. Of the 12 purebred breeds represented, the most common breed was the Labrador retriever (n=12). Of the 10 TTAP cases, 3 dogs had a 3.5/2.7mm tarsal arthrodesis plate placed, and 3 dogs had a 3.5/3.0mm tarsal arthrodesis plate placed. 4 cases did not have operative reports or radiographs available to review, and so implant details were not documented. Anaesthesia times were available for review in two cases. One CT screw case had an anaesthesia time of 80 minutes, and one TTAP cases had an anaesthesia time of 90 minutes. The median number of days between placement and removal of the implants were 43 (range 28- 81) and 61 (range 35-170) days for the CT screw and TTAP groups, respectively. The median follow up time after initial surgery was 171 (range 36-1670) and 185 (range 57-567) days for the CT screw and TTAP groups, respectively. 8 major complications were documented in the CT screw group, while 1 major complication was documented in the TTAP group. Complications associated with the CT screw included 5 dogs reinjuring the tendon (avulsion or rupture), 2 dogs developing tendon laxity, and 1 dog developing a surgical site infection after explant. Three screws were found broken at the time of explant, but this had not caused any apparent morbidity and was not documented as a major complication. The complication documented in the TTAP group was tendon laxity in one dog. The dog was not presented for plate removal until 170 days after initial surgery due to a suspect miscommunication. One plate broke and was explanted earlier than planned, but the dog was managed with an orthotic and was documented to have minimal lameness on exam 51 days after plate explant (Table 1 & Table 2).
| Patient | Age (years) | Sex | Breed | Pertinent history and PE | Lateral ization | Injury details | Tendon Repair | Implant details | Major Complication | Duration implant intact (days) | Follow up after initial surgery (days) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 8 | MI | Labrador | 10 days weight bearing lameness (WBL); PE revealed swollen and painful CCT insertion | Right | NA | 16G wire, tendon reconstruction | Fixin V3010 3.5 plate | No; broken plate | 35 | 86 |
| 2 | 9 | FS | Labrador | Acute onset WBL. PE revealed soft tissue swelling in region of CCT insertion | Left | NA | 1 PDS - locking loop with pre- drilled bone tunnel | VOI 3.5/2.7 plate, #5 3.5 screw and #2 2.7 screws | No | 39 | 82 |
| 3 | 6 | FS | Labrador | Acute onset lameness. PE revealed soft tissue swelling 2 inches proximal to CCT insertion | Left | SDF intact | 1 PDS - locking loop with 1.5mm bone tunnel | Fixin V3010 3.5 plate | No | 63 | 567 |
| 4 | 3 | FS | Terrier X | Acute onset lameness. PE revealed CCT laxity and soft tissue swelling at the CCT insertion. | Right | NA | 1 PDS - locking loop with pre- drilled bone tunnel | Fixin V3010 3.5 plate | No | 107 | 182 |
| 5 | 9 | MC | Labrador | Acute onset WBL duration 1 week. PE revealed soft tissue swelling at the CCT insertion, slight CCT laxity, and pain on palpation. | Right | SDF intact | 1 PDS - locking loop with pre- drilled bone tunnel using 0.045 K wire | VOI 3.5/2.7 plate, #5 3.5mm screws and #4 2.7mm screws | Yes; tendon laxity | 170 | 256 |
| 6 | 7 | MN | Labrador | Acute onset non-weight bearing lameness (NWBL). PE revealed soft tissue swelling at the distal CCT | Left | SDF intact | NA | NA | No | 64 | 84 |
| 7 | 10 | MN | Spaniel | Acute onset lameness. | Right | NA | NA | NA | No | 62 | 323 |
| 8 | 1 | MN | Labrador X | Acute onset lameness after being stepped on by a horse 14 days prior to presentation. | Right | Complete rupture | 1 PDS - locking loop suture with pre-drilled bone tunnel using 0.062 K wire | VOI 3.5/2.7 plate | No | 57 | 188 |
| 9 | 4 | FI | Labrador | Not available | Left | NA | NA | NA | No | 60 | 463 |
| 10 | 3 | MN | Labrador X | Acute onset lameness after laceration on kennel cage the day before presentation. | Right | Complete rupture | NA | NA | No | 49 | 57 |
| PATIENT # | Age (years) | Sex | Breed | Pertinent History and PE | Laterali zation | Injury Details | Tendon Repair | Implant Details | Major Complication | Duration implant intact (days) | Initial surgery (days) |
| 1 | 10 | FS | Labrador | Acute onset lameness. PE revealed weight bearing lameness (WBL) of affected hindlimb, with tarsal and digital hyperflexion; soft tissue swelling at CCT insertion. | Left | SDF intact | 1 PDS - 3 loop pulley and krackow suture patterns | 3.5mm CT screw | Yes; tendon laxity | 43 | 181 |
| 2 | 10 | FS | Vizsla | PE revealed WBL, digital hyperflexion, and soft tissue swelling at CCT insertion. | Right | SDF intact | NA | 3.5mm CT screw | No; screw broke | 64 | 89 |
| 3 | 9 | MN | English Pointer | Acute onset lameness. PE revealed non-WBL and soft tissue swelling over CCT insertion. | Left | NA | NA | 3.5mm CT screw | Yes; tendon re-avulsion | 42 | 200 |
| 4 | 1 | MN | Mixed Breed Dog | PE revealed tarsal hyperflexion and a laceration over the distal aspect of the CCT, visible tendon ends | Left | Complete tear | NA | 3.5mm CT screw | Yes; tendon infection | 42 | 260 |
| 5 | 9 | MI | Golden Retriever | Acute onset lameness duration of 3 weeks. | Left | NA | NA | 3.5mm CT screw and PRP injection | Yes; tendon re-avulsion | 48 | 768 |
| 6 | 5 | FS | Chinese Shar Pei | Acute onset lameness. PE revealed soft tissue swelling over R CCT. | Right | NA | NA | 3.5mm CT screw | No | 81 | 91 |
| 7 | 7 | FS | Labrador | NA | Left | NA | NA | 3.5mm CT screw, ESF placement, and ACP injection | No | 77 | 171 |
| 8 | 5 | FS | Chihuahua | NA | Left | NA | NA | NA | No | 28 | 36 |
| 9 | 0.75 | FS | Labrador | Acute onset lameness after laceration over R CCT. PE revealed tarsal hyperflexion and laceration with full trasection of CCT. | Right | NA | NA | 3.5mm CT screw | No | 40 | 1670 |
| 10 | 1 | MN | Great Dane | PE revealed WBL with soft tissue swelling over the CCT. | Right | NA | NA | CT screw | No | 42 | 42 |
| 11 | 6 | MN | German Shorthaired Pointer | Acute onset WBL. PE revealed pain and soft tissue swelling at CCT insertion with hyperflexion of digits. | Left | NA | NA | 3.5mm CT screw | Yes; tendon re-avulsion | 42 | 820 |
| 12 | 6 | MN | German Shorthaired Pointer | Acute onset NWBL. Pe revealed pain and soft tissue swelling at CCT insertion. | Right | NA | NA | 3.5mm CT screw | Yes; tendon re-avulsion | 47 | 152 |
| 13 | 14 | MI | German Shorthaired Pointer | NA | Left | NA | NA | 3.5mm CT screw | No | 43 | 43 |
| 14 | 8 | MN | Mixed Breed Dog | NA | Right | NA | NA | 3.5mm CT screw | No | 66 | 362 |
| 15 | 1 | MN | Labrador | Acute onset lameness. PE revealed WBL with a laceration over the level of the distal CCT. | Left | NA | NA | 3.5mm CT screw | No | 41 | 42 |
| 16 | 1 | FS | Mixed Breed Dog | Acute onset lameness, suspect trauma. PE revealed WBL and tarsal hyperflexion. | Left | NA | NA | 3.5mm CT screw | No | 53 | 124 |
| 17 | 6 | MI | Dalmation | Acute onset lameness after history of trauma. PE revealed WBL with soft tissue swelling over the CCT. | Left | NA | NA | 3.5mm CT screw | Yes; tendon re-avulsion | 78 | 870 |
Table 1: Summary of presentation, implant details, and follow up for patients who received a TTAP as postoperative immobilization
Discussion
To the authors’ knowledge, this is the first description of the temporary application of a medial tarsal arthrodesis plate as a method to immobilize the tarsus after primary calcaneal tendon repair. The results from this pilot study suggest that this method is an acceptable alternative to the currently described techniques. A potential disadvantage of the TTAP procedure is the overall increased perioperative morbidity associated with longer surgery. It may take relatively longer for the clinician to place the implant as compared to a CT screw, and the patient needs to undergo a second general anaesthesia event at time of explant, as opposed to an explant of a CT screw under sedation alone. However, given that the use of an external skeletal fixator (another well described technique) also demands longer anaesthesia time, the disadvantages associated with general anaesthesia are only pronounced when compared to the use of a CT screw. Due to the institution suffering loses of medical records from a natural disaster, surgery and anaesthesia times were largely unavailable for review. Documentation and comparison of anaesthesia times of future TTAP cases is recommended to be able to compare with the currently established techniques. Another plausible drawback of the TTAP procedure is the associated cost. While the cost of the TTAP surgical procedure may be increased compare to the CT screw procedure, the multiple bandage changes may eventually nullify the initial price difference. If future studies can demonstrate a significant improvement in outcome and client satisfaction with the TTAP procedure, the authors believe that these setbacks could be offset. The goals of immobilization of the tarsal joint are to protect the tendon repair and resist gap formation while the calcaneal tendon heals. New tendon collagen requires a degree of strain and load for development of correct alignment, although this should not be introduced until initial fibroplasia and collagenization take place over the initial 2-3 weeks [13]. The CT screw is traditionally placed to fix the joint in a hyperextended position. This can alleviate tension on the tendon in the initial phase of healing, but does not allow subsequent physiologic weight- bearing of the tendon to encourage appropriate alignment of the collagen. Additionally, the prolonged hyperextension predisposes the potential formation of superficial digital flexor tendon contracture, which some of the authors have experienced anecdotally in their patients. The TTAP is placed at a normal physiologic angle, which may facilitate the described appropriate tendon healing. To mitigate potential gap formation and failure of the primary repair, the surgeons in the study did not utilize the plate technique in patients that had excessive tendon shortening due to either contraction or need for debridement. Lister et al. demonstrated that maximum strain on the calcaneal tendon was similar in dogs with and without immobilized tarsi in a weight-bearing stance, and suggested that the protection offered with immobilization could stem largely from the decreased weight bearing as well as activity restriction [14]. Further investigation is needed to elucidate the role of the position of the tarsus in post-operative calcaneal tendon healing. The major complication rate in the CT screw cohort was 47% (n=8) in this study. A previous retrospective study involving 45 dogs who injured their calcaneal tendon, 37 of which received a CT screw, reported a 35% (n=16) overall complication rate, 6 cases of which were considered major. Only 3 of the 37 screws were noted to be bent or broken and had to be replaced (9). The relatively large difference in complication rate between the two studies can likely be attributed to low case numbers in addition to different definitions of major complications. 3 of the 17 CT screws in this study were broken at the time of explant, but that did not appear to compromise the repair; therefore, these did not contribute to the overall complication rate. However, 5 major complications in this study were due to reinjury (rupture or avulsion), all of which happened at least 6 months after the primary tendon repair surgery. It is possible that these tendons were not adequately healed prior to return to normal activity, or that the dogs were returned to full activity too quickly. Future research should involve repeated ultrasounds at regular intervals in order to differentiate between fully healed tendons that are re-injured or tendons that have not fully healed.
There was 1 major complication in the TTAP cohort: tendon laxity. The dog did not present for plate explant until 150 days after explant, due to a miscommunication. It is reasonable to presume that if the explant procedure was done within the recommended time frame, this complication could have been avoided. The dog was placed in a splint for 4 weeks after explant surgery, but there was no clinical improvement after splint removal. A tarsal arthrodesis or tendon shortening procedure was recommended, but the dog was lost to follow up after this recommendation was made. There was one TTAP case that documented a broken plate on recheck radiographs 15 days after surgery. The plate was explanted 35 days after surgery and the dog was managed medically with a custom orthotic. 51 days after explant, the dog was documented to be doing well with minimal lameness. While the number of TTAP cases was relatively low, it is encouraging that a single major complication was documented in this cohort. Future studies with more cases and detailed documentation of progression are necessary to better validate the procedure and possible complications. There were several limitations of this study. The retrospective design limited the conclusions drawn from the data. The primary tendon repair method was not standardized; future study designs should plan to eliminate this as a factor confounding data interpretation of immobilization method. Case management and documentation varied among surgeons, limiting the conclusions able to be drawn from certain details such as potential bandage morbidity, lameness examinations, or differences between types of initial tendon injuries. Case selection of the population that received the TTAP also differed from those selected for application of the CT screw, as dogs that required tendon debridement were not eligible for placement of a TTAP. Objective outcome measures were not utilized, such as tendon ultrasound, or gait analysis. Although the previously cited literature regarding calcaneal tendon also utilized subjective gait analysis, objective outcome measures would have been preferable. In addition, the institution that this study was conducted at suffered a natural disaster within the years the procedures were performed; consequently, many details in the records were lost and unable to be evaluated and analysed as part of this study, including implant information, imaging studies and surgery and anaesthesia data. The relatively small case numbers also precluded direct comparison of results between the CT and TTAP cases.
In conclusion, the results of this pilot study demonstrate the application of a TTAP as an acceptable immobilization technique after primary calcaneal tendon repair despite limited case numbers. A prospective, controlled, multi- institutional study is warranted to validate the procedure.
References
-
Dueland R, Quenin J (1980) Triceps tenotomy: biomechanical assessment of healing strength. Journal of the American Animal Hospital Association 16: 507.
-
Carmichael S, Marshall WG (2018) Tarsus and Metatarsus. In: Tobias KM, Johnston SA, editors. Veterinary Surgery: Small Animal. 1. (2 Edn). St. Louis, MO: Elsevier pp: 1193-1209.
-
Denny HR, Butterworth SJ (2000) The Tarsus. A Guide to Canine and Feline Orthopaedic Surgery. 4 Edn. Ames, IA: Blackwell Science Ltd pp. 575-597.
-
Reinke JD, Mughannam AJ, Owens JM (1993) Avulsion of the gastrocnemius tendon in 11 dogs. Journal of the American Animal Hospital Association 29(5): 410-418.
-
de Haan JJ, Goring RL, Renberg C, Bertrand S (1995) Modified Transarticular External Skeletal Fixation for Support of Achilles Tenorrhaphy in Four Dogs. Vet Comp Orthop Traumatol 8(1): 32-35.
-
Morshead D, Leeds EB (1984) Kirschner-Ehmer Apparatus Immobilization Following Achilles Tendon Repair in Six Dogs. Vet Surg 13(1): 11-14.
-
Guérin S, Burbidge H, Firth E, Fox S (1998) Achilles Tenorrhaphy in Five Dogs: A Modified Surgical Technique and Evaluation of a Cranial Half Cast. Veterinary and Comparative Orthopaedics and Traumatology 11(4): 205-210.
-
Nielsen C, Pluhar GE (2006) Outcome following surgical repair of achilles tendon rupture and comparison between postoperative tibiotarsal immobilization methods in dogs: 28 cases (1997-2004). Vet Comp Orthop Traumatol 19(4): 246-249.
-
Corr SA, Draffan D, Kulendra E, Carmichael S, Brodbelt D (2010) Retrospective study of Achilles mechanism disruption in 45 dogs. Vet Rec 167(11): 407-411.
-
Sugiyama T, Woodward A, Ryan SD (2018) Biomechanical evaluation of 6 transarticular tibiotarsal immobilization methods in canine cadaveric limbs. Vet Surg 47(5): 705- 714.
-
Johnson KA (2014) Approach to the Calcaneus. Piermattei’s Atlas of Surgical Approaches to the Bones and Joints of the Dog and Cat (5Edn.) St. Louis, MO: Elsevier pp. 448-449.
-
Johnson KA (2014) Approach to the Medial Malleolus and Talocrural Joint. Piermattei’s Atlas of Surgical Approaches to the Bones and Joints of the Dog and Cat (5Edn.) St. Louis MO: Elsevier pp: 440-443.
-
Carmichael S, Marshall WG (2018) Muscle and Tendon Disorders. In: Tobias KM, Johnston SA, editors. Veterinary Surgery: Small Animal (1.2 Edn.) St. Louis, MO: Elsevier pp. 1316-1322.
-
Lister SA, Renberg WC, Roush JK (2009) Efficacy of immobilization of the tarsal joint to alleviate strain on the common calcaneal tendon in dogs. Am J Vet Res 70(1): 134-140.
- The Digital Stethoscope: Harnessing AI in Veterinary Medicine Without Losing Our Healing Touch
- Meningoencephalomyelitis of Unknown Etiology: Short-Term Effect of Two Treatment Protocols on Cerebrospinal Fluid
- Safety and Efficacy of the HomeoPet Cough in Domestic Pets –A Clinical and Correction Analysis Based Upon User Response Survey
- Non Human Animals Responses to Social Loss
- Owner Reported Clinical Outcomes of a Homeopathic Proprietary Preparation for the Treatment of Upper Respiratory and Nasal Disorders in Companion Animals
- Effects and Diagnostic Approach of Ultrasound in Veterinary Practice: A Systematic Review