The Effects of Cognitive-Enhancing Activities in Senior Canine Patients
Aging process in dogs seem to be like aging in people. Human Alzheimer’s is a neurodegenerative condition very similar to the disorder in dogs, Canine Cognitive Dysfunction (CCD). CCD affects several areas of the brain, mainly ones responsible for regulating locomotion, problem-solving, navigation, and long-term memory. The onset of the disease occurs when neurotoxins are released into the brain. The presence of these toxins is manifested through symptoms including restlessness or lack of movement, disorientation, decreased ability to recognize family members, changes in patterns of interaction, sleep pattern alterations, and loss of house training. Treatment for this disorder is multimodal, including behavioral modification intended to stimulate the brain. In the present study, the canine cognition program, Dognition® was tested for its possibility to aid as a behavioral modification treatment plan to ameliorate symptoms of CCD assessed by a validated scale. We found that after the Dognition® activities, over half of the participants in the trial improved their scores for memory and communication. Additionally, before and after treatment, we found that that over half of the participants also improved their cognition scores. Implementation of diagnostic methods and behavioral modification programs is necessary to recognize and treat CCD in dogs.
Introduction
The canine brain plays the most crucial roles in natural body functioning, including the regulation of movement, response to stimuli in the environment, control of emotions and behavior, and basic body functions such as the sleep/ wake cycle and metabolic rates. The frontal cortex is the most anteriorly situated portion of the cerebrum, and it is known as the major motor cortex, functioning to initiate body movements, problem- solving, cognition and store memories [1]. Additionally, the hippocampal region of the brain, located centrally in the cerebrum, functions in maintaining additional traits associated with cognition, mainly focusing on long-term memory and navigation [2]. Utilizing the hippocampal and frontal cortex, the dog processes the world around it through perception, awareness, learning, memory, and decision-making process known as cognition [3]. This processing of information is very important to a dog’s learning and behavior, and any changes in cognitive function can result in a decline of learned behaviors.
Canine Cognitive Dysfunction (CCD) was initially assessed in a laboratory setting in which researchers compared the cognitive responses elicited in young and elderly dogs. The researchers used simple learning tasks and advanced memory activities in a reward-based system to test canine cognitive function and demonstrated impaired spatial memory and altered executive functioning in senior dogs [4]. Furthermore, research has shown that CCD is very similar to human Alzheimer’s disease in the sense that the physical brain changes observed are nearly identical. Beta-amyloid plaques are seen in both human and canine aging brains, developing first in the frontal cortex, followed by the hippocampus [5, 6, 7]. The beta-amyloid plaque is a proteinaceous formation that is naturally occurring throughout the body that can negatively target the brain by its neurotoxic effects on the nerve cells within the brain [8]. In elderly Beagle dogs, beta- amyloid plaques were identified through computerized image analysis and through their responses to cognitive stimuli. Authors found a strong correlation between the number and size of plaques present in the cerebrum and a decline in cognitive abilities, such as spatial memory [9]. Unfortunately, however, these physical changes cannot be seen upon examination and are only seen through advanced imaging testing or histopathology. Currently, an MRI is the only method that is used to confirm degenerative process associated with CCD, since histopathology is performed postmortem and mostly used for research purposes.
In a clinical setting, the disorder is characterized by several symptoms including: changes in activity resulting in restlessness or lack of movement, increased disorientation, decreased ability to recognize family members, changes in patterns of interaction, sleep pattern alterations, and loss of house training [10]. Many of these changes are often found to be vague or are misinterpreted, leading to lack of diagnosis of CCD in veterinary medicine [11]. Even though this disorder is exceedingly common in the United States, nearly 85% of potentially affected dogs will remain undiagnosed [12].
Cognitive decline scales have been developed in the past to better assess and more accurately diagnose cognitive dysfunction in dogs, such as the Canine Cognitive Dysfunction Rating scale (CCDR) [13], Rofina Scale [14], CAnine DEmentia Scale (CADES) [15], and the Age-Related Cognitive and Affective Disorders scale (ARCAD) [16]. Common criteria identified within these scales include orientation, memory, sleep/wake disturbances, and house-soiling [15, 17]. By using a numeric rating to interpret the dog’s behavior in each of the categories, the sum the result from each section suggests that the overall score indicates the presence of CCD. If it is concluded that the patient does in fact have CCD, then immediate treatment is warranted.
Veterinarians often explore different treatment options with the owners to find the best fit for the individual patient. Treatment options include dietary changes, nutraceuticals, drug therapy, pheromones, sedatives, and behavior modification. Both dietary changes and nutraceuticals aim to improve brain chemical physiology. Exercise and diets rich in antioxidants can help to reduce oxidative stress and possibly delay the effects of aging by providing the essential fatty acids needed to repair damaged brain cells [18]. Drug therapy often involves medications such as L-deprenyl, which ultimately works to increase the amount of oxygen supplied to the brain by increasing cardiac output [19]. Drug therapy is more effective when combined with a behavior modification protocol and environmental management, which promote both mental and physical stimulation using cognitive activities. Mentally stimulating activities may promote cell growth in the hippocampus by increasing blood flow to the central nervous system [12]. A study on dogs diagnosed with CCD and treated with a diet rich in antioxidants, a behavior modification program, or the combination of the diet and behavior program showed that the antioxidant diet combined with daily walks, social interaction, cognitive stimulating toys, and cognitive stimulating games was the most successful treatment for CCD, and it even seemed to have helped to reduce the effects of the present beta-amyloid plaques that were observed in the participants [20].
Due to the recent research findings that have highlighted the positive effects of behavioral modification programs, there has been an increased interest in canine cognition and CCD. One of the most popular canine cognition programs is Dognition®, which was developed by Dr. Brian Hare, the Director of the Duke Canine Cognition Center. This program involves a series of games that, once completed, gives the owner a personality assessment of the dog. Additionally, after completion of the program, the owner receives a detailed report on how the dog processes information and responds to social cues [21]. Although this program was not developed with the intent of treating cognitive dysfunction in dogs, it does indeed have the behavioral modification component often used in research that could be a helpful tool to prevent and treat CCD.
Hypothesis and Predictions
Behavior modification games used to stimulate cognitive function have shown to be a useful tool to help counter the effects of CCD. However, owners are often unable to find specific cognitive stimulating games to play with their dogs or have limited access to programs shown to be correlated with preventing CCD. The online program, Dognition®, will be tested for its mentally stimulating effects and its use as a behavioral modification tool for CCD. Additionally, the ARCAD scale will be used to score the participants during the trial and was chosen based upon its ability to differentiate between affective disorders and cognitive disorders.
We hypothesized that the Dognition® program would have a positive effect on cognitive function of elderly dogs with changes assessed by the ARCAD scale. We predicted that after an initial Dognition® series of activities was completed, followed by a week of practice with the owner at home, the initial ARCAD score recorded for the dog during the first session would decrease after a week of cognitive stimulation provided by the Dognition® games.
Methods
This study was approved for exemption by the Institutional Review Board (IRB) and was approved by the Institutional Animal Use and Care Committee (IACUC).
Privately owned dogs were recruited through electronic mail by contacting current and former students, PhD students, and faculty members from the Washington State University, College of Veterinary Medicine. Initially, owners received an invitation to participate, and if willing to do so, they were asked to respond to the email for more information. Following, owners were provided with a second email explaining the specific details of the investigation and their role in testing. If the terms were then agreed upon, owners were asked to sign up for a testing date. Testing was conducted for 22 days.
Upon arrival, both the owner and the dog were escorted back to the testing area to begin the initial questionnaire (testing occurred at Washington State University’s Veterinary Teaching Hospital in room “Special Medicine 1706AB”). To initiate testing, the Age-Related Cognitive and Affective Disorders (ARCAD) scale was used to evaluate the participant’s current cognitive status. For consistency, the same researcher with a general understanding of the scale and how to interpret the categories recorded the responses for the owner. On the ARCAD scale, a higher score indicates a greater risk or diagnosis of CCD, and a lower score indicates behavior closer to normal aging. After completion of this initial assessment, the owner was then asked to replace their leash with a provided slip lead, and subsequently, to hand the lead to a research assistant to start the cognitive games.
To begin the games, a research assistant demonstrated to the owner how to play the first game from the Dognition® series with the dog. After a thorough explanation, the owner was then asked to perform the movements as demonstrated, to elicit a response from the dog. This pattern was continued until the last game in the Dognition® series was completed (Refer to “Table 1” for the general layout of activities performed during the trial; Refer to Appendix E for the complete list of activities). For each activity, the responses elicited from the dog were recorded on a data sheet by a research assistant.
| Empathy | Warm Up |
| Empathy | Yawn Game |
| Empathy | Eye Contact Game |
| Communication | Warm Up |
| Communication | Response to Arm Pointing |
| Communication | Response to Foot Pointing |
| Cunning | Watching |
| Cunning | Turning Back |
| Cunning | Covering Eyes |
| Cunning | Turning Back |
| Memory | Warm Up (Cups) |
| Memory | Pointing vs. Memory (Cups) |
| Memory | Smell vs. Memory (Cups) |
| Memory | Delayed Cup Game (Cups) |
| Reasoning | Warm Up |
| Reasoning | Inferential Reasoning (Cups) |
| Reasoning | Warm Up |
| Reasoning | Physical Reasoning (Paper) |
Table 1: Summary of Dognition Series.
Once the activities were completed, the owner was then asked to sign up for a return evaluation date one week after the initial testing series. Additionally, the owner was asked to complete a small homework assignment with the dog for approximately 10 minutes each day for the following seven days, involving a short, adapted version of the Dognition® series. The homework included a game from both the “Communication” and “Memory” sections of the program. On the seventh day, the owner was instructed to record the responses from the dog and return them to the research team.
After the seven-day homework period, the owner returned to the WSU Veterinary Teaching Hospital, without the dog, to again complete the ARCAD scale. The same research assistant recorded the owner’s responses to the questionnaire, asking the same questions regarding the criteria outlined within the scale. Following completion, the owners were thanked for their participation, as they had successfully completed their part in the trial.
In order to determine if the mean response of the initial ARCAD scores was statistically different than the mean response of the final ARCAD score, a Paired Sample Student T-Test was conducted. The program used to perform this test was Microsoft Excel 2013. Additionally, the average initial responses to the Dognition® activities were compared to the final responses recorded by owners through the homework assignment. These scores were compared as a percentage also generated by Microsoft Excel 2013.
Results
Although all responses were recorded from the initial Dognition® series, the two categories that were measured for changes in response were Memory (Figure 1) and Communication (Figure 2), since these were the two categories additionally tested in the homework. An improvement in response was defined as the correct elicited response from the activity, according to the Dognition® program.
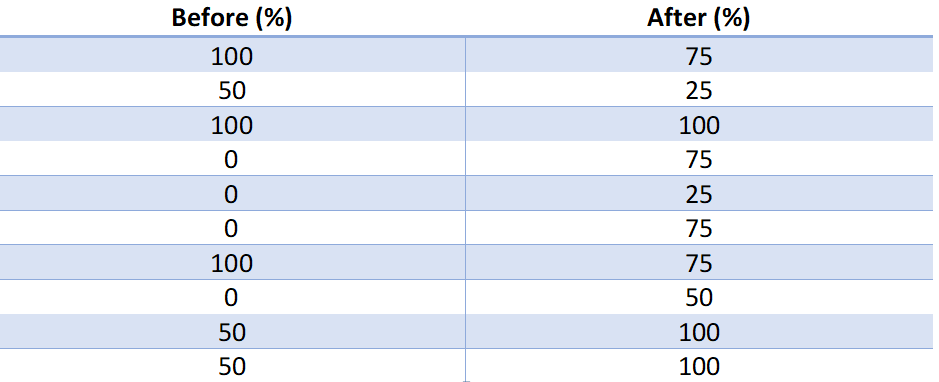
Before and after Dognition® scores for memory elicited by the participant: The before scores were recorded by the research team during the initial assessment in the experimental room, while the after scores were recorded by the owner at home on the seventh day of completing the homework. Scores are recorded as the percentage of correct responses.
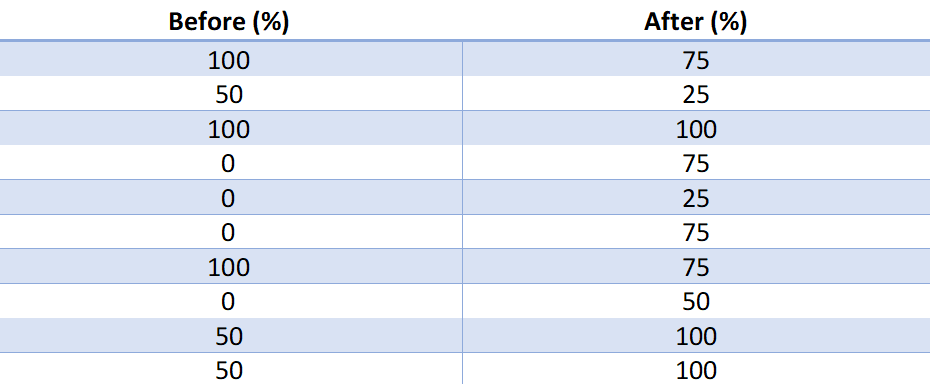
Before and after Dognition® scores for communication elicited by the participant: The before scores were recorded by the research team during the initial assessment in the experimental room, while the after scores were recorded by the owner at home on the seventh day of completing the homework. Scores are recorded as the percentage of correct responses.
From the 10 participants in the study, 60% had an improvement in their memory (Figure 3) responses and 70% had an improvement in their communication responses (Figure 4).
The percentages were determined by comparing the before and after scores for all participants, of which had a higher rate of correct responses after a week of the assigned homework. Additionally, in the memory portion, 30% experienced a decline while 10% showed no improvement. Furthermore, in the communication portion, a similar trend was observed and 20% of the dogs had a decline, while 10% had no improvement or no change.
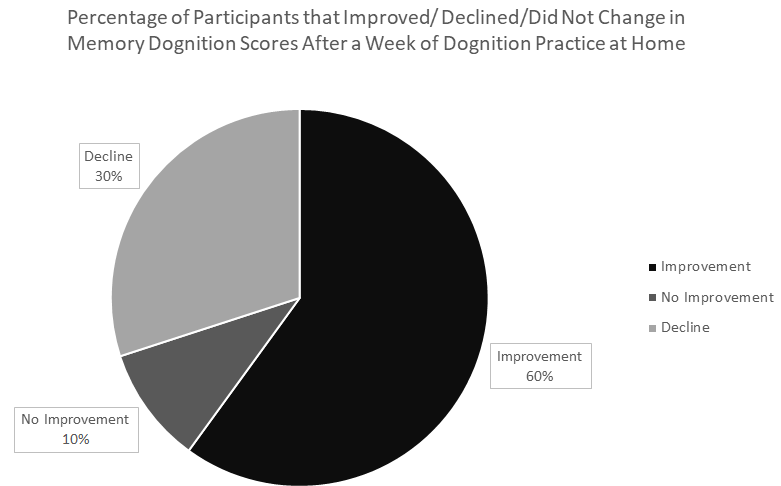
60 % of dogs improved in Dognition® Memory responses after a week of practice at home with the owners. Additionally, 10% of the dogs experienced no change and 30% experienced a decline in memory scores.
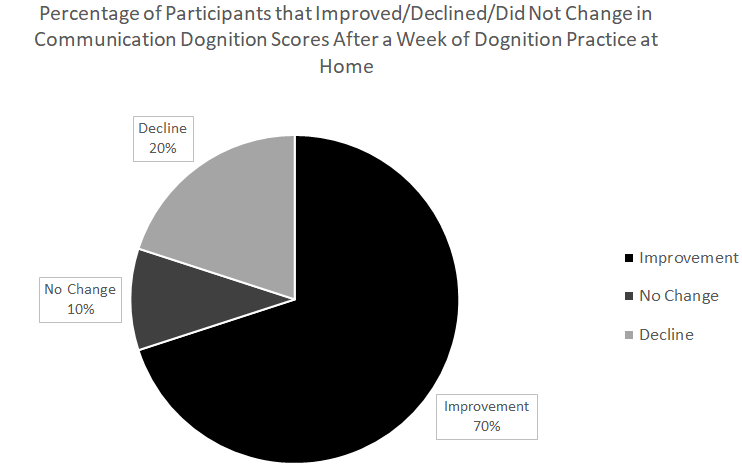
70 % of dogs improved in Dognition® Communication responses after a week of practice at home with the owners. Additionally, 10% of the dogs experienced no change and 20% experienced a decline in communication scores.
The T-test analysis comparing the “Before” and “After” ARCAD scores showed that the difference in the means from the before ARCAD scores vs. after ARCAD scores were statistically significant. There was a significant difference in the scores for the ARCAD “Before” (Mean=18, Standard deviation=4.784) and ARCAD “After” (Mean=15.7, Standard deviation=4.295) conditions; t (4), p = 0. 003219 (Figure 5).
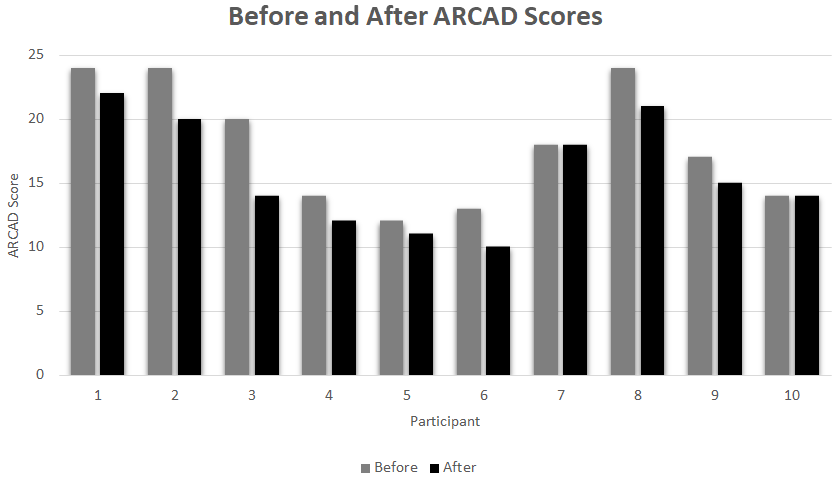
The before and after scores of the ARCAD scale: The owner was first asked the questions about their dog’s cognitive functioning on the initial testing day (before) and then was again questioned after a week of the homework assignment (after).
Additionally, 80% of participants improved upon their initial ARCAD score, 40% of which went down a category on the ARCAD scale, rather than just improving upon their initial score (Figure 6).
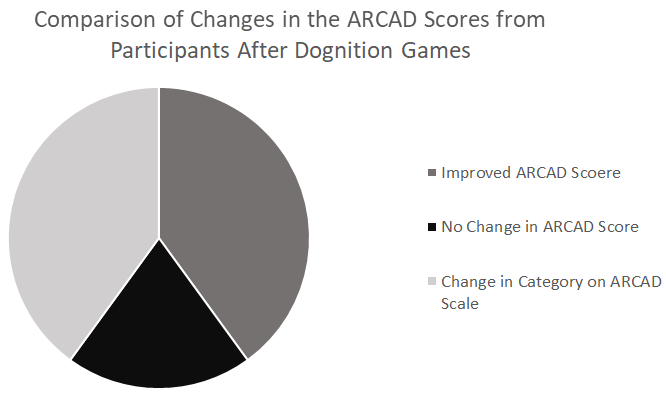
Based upon the initial responses recorded in the ARCAD Scale and comparing them to the second ARCAD scores that were recorded after the Dognition® games, 40% of participants improved scores, and 40% changed categories on the scale (toward the normal score values ), while 20% showed no change.
Discussion
In this study, we aimed to investigate if the Dognition® program was an effective tool for the behavior modification of senior patients, and therefore, a potential treatment modality for CCD. Currently, there is significant research interest in the causes and symptoms related to CCD, while fewer studies focus on treatment of the disorder. Additionally, of the studies that have suggested behavior modification as a valid treatment modality, there fails to be a validated treatment plan that is easily accessible for both owners and veterinarians. The current behavior modification protocols for CCD described in the literature seem to be non-specific and remarkably vague.
The data from this trial showed that the Dognition® program had profound effects on senior dogs’ cognitive capabilities. Over half of the dogs included in the study improved in both memory and communication functioning, areas that are notably impaired in patients displaying the symptoms of CCD. Furthermore, since the frontal cortex and hippocampus, the areas responsible for motor function and long-term memory respectively, are the main targets of CCD, we suggest that these areas were possibly the most stimulated regions of the brain. With increased stimulation of both the frontal cortex and hippocampus, the blood flow to these areas may have been increased, stimulating cell growth, and effectively counteracting the degenerative effects seen in the most commonly targeted regions of the brain affected by CCD [12].
The ARCAD assessment showed that the difference in means from the “Before” and “After” ARCAD scores was statistically significant. According to the ARCAD scale, dogs whose score ranges between 9-15 are experiencing normal aging, while those whose score ranges between 16-21 are borderline CCD patients who should be re-evaluated every 6 months. Our data suggest that the cognitive games provided by the Dognition® series were able to change a borderline cognitive decline and decrease the effects of the disorder to a point in which the dogs’ behaviors were interpreted as normal aging.
A previous study on the behavior of 25 dogs ranging from ages 3 to 19 years of age was assessed using the ARCAD score upon veterinary-recommended euthanasia due to a chronic illness or disorder. The brains from these dogs were then studied for the characteristic signs of CCD, including the unique beta-amyloid plaque formation. The authors found that the patients exhibiting higher ARCAD scores also had greater beta-amyloid plaque formation and tended to be amongst the oldest of the group. On the other hand, those who had unremarkable ARCAD scores, similarly had little to no presence of beta-amyloid plaques, specifically on the frontal cortex and hippocampal regions [22]. We suggest that the dogs in our trial with high ARCAD scores most likely also had a greater accumulation of beta-amyloid plaques in the same brain areas, which may explain the cognitive deficit identified before the trial. Many of the dogs with higher ARCAD scores in the study also showed a decrease in their score after one week of cognitive stimulation. The physiological alterations associated with this change in score are unknown and we cannot attribute to the use of cognition games at this point, but we entertain the possibility that behavioral modification programs do indeed have positive effects on the canine brain, potentially to a molecular level, with a mechanism yet to be investigated.
Even though most participants improved in their communication and memory scores, several participants showed no improvement, or even a decline in correct responses after the at-home Dognition® games. This outcome could be because some dogs may not respond to cognitive stimulation as well as others, or even have a more severe form of CCD, which is very difficult to assess without imaging. A future study with pre and post magnetic resonance findings associated with the ARCAD scores may warrant more accurate and easier to interpret findings. Additionally, since a research assistant was initially recording the “Before” results and the owners recorded the “After” results, the data may be inconsistent due to the bias of the owners, or a misinterpretation of responses. We also entertain the possibility that since the dogs were practicing the games at home for a week, and the second data point was recorded on the seventh day, dogs may have gotten bored with the activities, and lost interest in playing the games. There is also the possibility that the treats the owner was using were not consistently treats of high value and the dogs lost interest in performing the tasks.
Many other factors can influence a dog’s behavior and response to stimuli including health status, environmental factors, or other animals. If the dog had distractions in the room such as another dog barking, someone talking nearby, or even loud noises outside, the response to the game could have been interfered with. Furthermore, if the dog was not feeling well the day the owner recorded responses, it is possible that some dogs drive to perform the tasks was diminished.
The diagnosis of CCD is becoming more and more crucial as many cases go undiagnosed, and therefore, untreated. Early diagnosis and treatment may increase quality of life of senior patients, preventing the development of affective disorders such as depression and anxieties secondary to the cognitive decline. Owners often are unable to recognize cognitive decline symptoms in their dogs due to the common misconceptions associated with normal brain aging. From an owner’s perspective, it is acceptable for the elderly dog to become unable to control certain behaviors, or become unresponsive to commands, not recognize familiar people or the environment due to a decrease in sensory capabilities such as hearing or vision. Many owners feel defeated as they watch their dogs slowly develop impairments, and interpret it as an effect of time, rather than a disorder that can be treated, and potentially even delayed in onset if diagnosed and treated early enough.
Education of both owners and veterinarians on the positive effects associated with behavioral modification, CCD can become more readily recognized and treated. Implementation of one of the diagnostic scales such as the CADES, Rofina, CCDR, or ARCAD scales is the first step to diagnose CCD. Furthermore, it is important to emphasize that owners should also have a role in the treatment and prevention processes. Understanding the full spectrum of CCD and the multimodal therapy approach is of utmost importance in ameliorating the quality of aging in dogs.
To further improve future testing, a control group for not only within, but also between groups analysis should be considered. Additionally, one should consider a blind to the protocol trial where owners were unaware of what the expected outcome could be, given that details within the study can often be subjective, and therefore, influence the owner’s responses during testing. Finally, future studies should also lengthen the duration of the trial, to observe the long-term effects associated with behavioral modification, if any.
Conclusion
The Dognition® program seems to be a useful tool as a behavioral modification treatment for CCD. By exploring different types of behavior modification activities that can be easily performed at home by owners, associated with other treatment modalities for CCD, one can expect the number of severe cases of CCD to dwindle. Early diagnosis and CCD prevention is key while more research into the exact causes of the disorder is necessary. Validated scales to assess cognitive decline can be effectively used to diagnose the disease, and a treatment plan involving behavior modification should be readily implemented to mitigate the effects of cognitive decline.
References
-
Tapp PD, Siwak CT, Gao FQ, Chiou JY, Black SE, et al. (2004) Frontal Lobe Volume, Function, and Beta-Amyloid Pathology in a Canine Model of Aging. J Neurosci 24(38): 8205-8213.
-
Tapp CT, Head E, Muggenburg BA, Milgram NW, Cotman CW (2007) Neurogenesis decreases with age in the canine hippocampus and correlates with cognitive function. Neurobiol Learn Mem 88(2): 249-259.
-
Frank D (2002) Cognitive Dysfunction in Dogs. Hill’s European Symposia on Canine Brain Ageing. Accessed.
-
Landsberg G, Araujo JA (2005) Behavior Problems in Geriatric Pets. Vet Clin North Am Small Anim Pract 35(3): 675- 698.
-
Borras D, Ferrer I, Pumarola M (1999) Age-related Changes in the Brain of the Dog. Vet Pathol 36(3): 202- 211.
-
Azkona G (2009) Prevalence and risk factors of behavioral changes associated with age-related cognitive impairment in geriatric dogs. J Small Anim Pract 50(2): 87-91.
-
Satou T, Cummings BJ, Head E, Nielson KA, Hahn FF, et al. (1997) The progression of beta-amyloid deposition in the frontal cortex of the aged canine. Brain Res 774(1-2): 35-43.
-
Gandy S (2005) the role of cerebral amyloid beta accumulation in common forms of Alzheimer disease. J Clin Invest 115(5): 1121-1129.
-
Cummings BJ, Head E, Afagh AJ, Milgram NW, Cotman CW (1996) Beta-amyloid accumulation correlates with cognitive dysfunction in the aged canine. Neurobiol Learn Mem 66(1): 11-23.
-
Hunthausen W (1994) Identifying and treating behavior problems in geriatric dogs. Vet Med 89(9): 688-700.
-
Osella MC, Re G, Odore R, Girardi C, Badino P, et al. (2007) Canine cognitive dysfunction syndrome: Prevalence, clinical signs, and treatment with a neuroprotective nutraceutical. Applied Animal Behaviour Science 105(4): 297-310.
-
Druce K (2014) Canine cognitive dysfunction- recognition and treatment. Veterinary Nursing Journal 29(8): 268- 270.
-
Salvin HE, McGreevy PD, Sachdev PS, Valenzuela MJ (2011) the canine cognitive dysfunction rating scale (CCDR): a data-driven and ecologically relevant assessment tool. Vet J 188(3): 331-336.
-
Rofina JE, Ederen AM, Toussaint MJM, Secreve M, Van A, et al. (2006) Cognitive disturbances in old dogs suffering from the canine counterpart of Alzheimer’s disease. Brain Res 1069 (1): 216-226.
-
Madari A, Farbakova J, Katina S, Smolek T, Novak P, et al. (2015) Assessment of severity and progression of canine cognitive dysfunction syndrome using the CAnine DEmentia Scale (CADES). Applied Animal Behaviour Science 171: 138-145.
-
Pageat P (1998) Patologia comportamentale Del cane. Pp: 346-356.
-
Schutt T, Toft N, Berendt M (2015) A comparison of 2 screening questionnaires for clinical assessment of canine cognitive dysfunction. Journal of Veterinary Behavior 10(6): 452-458.
-
Snigdha S, Berchtold N, Astarita G, Saing T, Piomelli D, et al. (2011) Dietary and Behavioral Interventions Protect against Age Related Activation of Caspase Cascades in the Canine Brain. PLoS One 6(9): e24652.
-
Ruehl WW, Bruyette DS, DePaoli A, Cotman CW, Head E, et al. (1995) Canine cognitive dysfunction as a model for human age-related cognitive decline, dementia and Alzheimer’s disease: clinical presentation, cognitive testing, pathology and response to 1-deprenyl therapy. Prog Brain Res 106: 217-25.
-
Pop V, Head E, Hill MA, Gillen D, Berchtold NC, et al. (2010) Synergistic effects of long-term antioxidant diet and behavioral enrichment on beta-amyloid load and non-amyloidogenic processing in aged canines. J Neurosci 30(29): 9831-9839.
-
Stewart L, MacLean EL, Ivy D, Woods V, Cohen E, et al. (2015) Citizen science as a new tool in dog cognition research. PLoS ONE 10(9): e0135176.
-
Colle MA, Hauw JJ, Crespeau F, Uchihara T, Akiyama H, et al. (2000) Vascular and parenchymal Abeta deposition in the aging dog: correlation with behavior. Neurobiol Aging 5: 695-704.
- The Digital Stethoscope: Harnessing AI in Veterinary Medicine Without Losing Our Healing Touch
- Meningoencephalomyelitis of Unknown Etiology: Short-Term Effect of Two Treatment Protocols on Cerebrospinal Fluid
- Safety and Efficacy of the HomeoPet Cough in Domestic Pets –A Clinical and Correction Analysis Based Upon User Response Survey
- Non Human Animals Responses to Social Loss
- Owner Reported Clinical Outcomes of a Homeopathic Proprietary Preparation for the Treatment of Upper Respiratory and Nasal Disorders in Companion Animals
- Effects and Diagnostic Approach of Ultrasound in Veterinary Practice: A Systematic Review