Improvement in Facial Function after Delayed Nerve Decompression in a 48-year-old male with Facial Palsy
Facial palsy occurring as a complication in patients of chronic otitis media is rare. Cases presenting immediately or even within few months after onset of palsy the management hold no ambiguity. Cases presenting much late to hospitals cast, however, doubt over the surgical management. The surgical intervention is indicated as a last resort or performed along with a revision surgery after educating the patient about the guarded prognosis. Our presented case signifies the importance of performing a much delayed nerve decompression in cases with a partial facial nerve palsy, non-cholesteatoma disease, and intact perineurium with no association of co-morbidities. ;
Introduction
The incidence of facial palsy in association with chronic otitis media (COM) has decreased significantly with evolution of potent antibiotics and improving disease care. The literature estimates incidence rates up to 5%. Though rare, it has a very dramatic presentation due to its functional and cosmetic value. The need for nerve decompression at the earliest is the golden standard of management. The ambiguity relates to the timing and utility of nerve decompression in cases presenting late to the tertiary centres [1]. Our paper raises the possibility of nerve decompression in such cases. To date, this paper may also be the first one to report an improvement in the facial palsy of a middle-age male within the English medical literature.
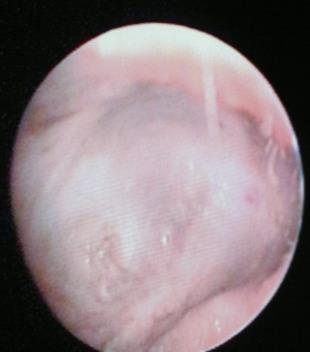
A 67 year old man presented to our tertiary care institute with a history of bilateral hearing loss for 10 years, with left facial palsy since 1962 and persistent discharge in the left ear. The patient also had history of isolated attacks of vertigo over the past 3-4 years. Facial palsy was developed after a surgery for the discharging ear in 1962. The patient’s otological evaluation was suggestive of a discharging left ear with evidence of granulations in the neotympanum and the mastoid cavity with grade 4 facial nerve palsy according to House– Brackmann score. The neuro-otological examination was normal and fistula test was negative. The patient wanted treatment for the persistent discharge and was also ready Otolaryngology Open Access Journal
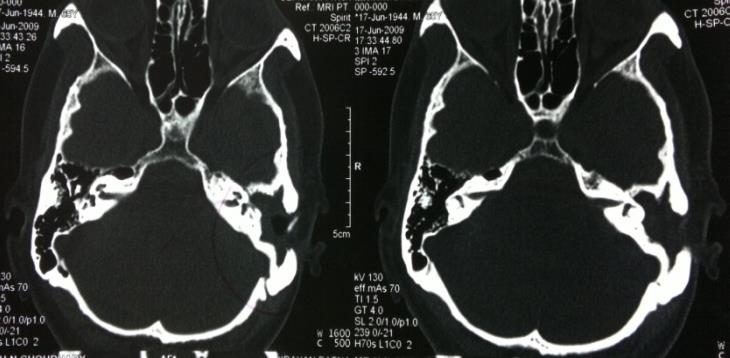
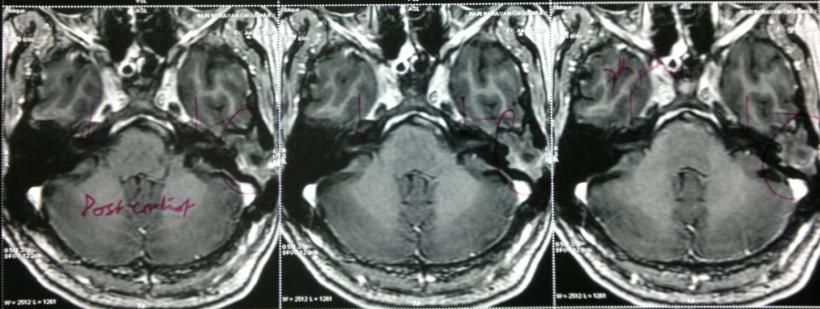
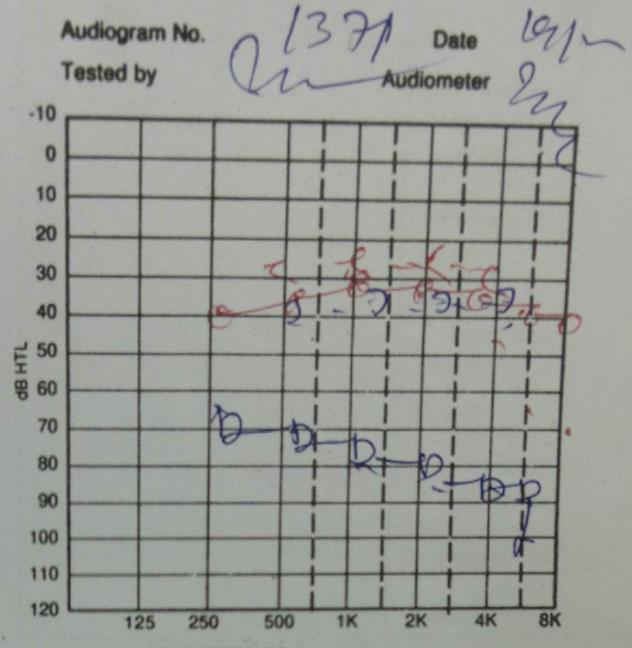
for a surgical intervention. The patient was educated about the surgery in detail and also a very guarded prognosis was explained with regard to his facial nerve palsy and impairment of hearing (Mixed hearing loss) (figure-1). The radiology was also suggestive of a recurrent/residual disease (figure-2). The patient underwent a left sided revision mastoidectomy with facial nerve decompression in our facility because the patient previously underwent a canal wall down mastoidectomy. Intra-operatively, the neo-tympanum and the cavity was found to be filled with granulation tissues and excepting foot plate of stapes all the other ossicles were absent. Granulation tissues over the oval and the round window were removed carefully. The facial nerve was found to be exposed in the tympanic part and there was severe an oedema with evidence of injury in the 2nd genu with a destruction of about (50%) of the fibres. The injured segment was covered in granulation tissues, which were removed meticulously and a nerve decompression was performed from the 1st genu to the vertical segment. In the post-operative period, the patient had an uneventful recovery, with no further complaints of discharge or detoriation of hearing till 1year of follow-up. The histopathological examination revealed fibro-collagenous tissue and inflammatory granulation tissue. Moreover, there was a remarkable improvement in facial nerve palsy from grade 4 to grade 2, in 6 months post-surgery (figure- 3). The high surgical gain attained is maintained till the last follow up session.

Discussion
The occurrence of facial palsy in cases of COM could be due to either direct involvement of the nerve by the disease or indirect injury in the form of compression, osteitis, toxin injury etc. In our case the evidence of injury suggests a probable iatrogenic cause or a rare scenario of disease causing direct destruction of the nerve. The approximately 10% chance of an exposed tympanic Otolaryngology Open Access Journal
segment with dehiscent canal bone renders this area more susceptible to injury. The literature review suggests that cholesteatoma is more often implicated in causing facial nerve paralysis than a granulation disease [2, 3]. The cholesteatoma matrix is postulated to cause direct damage to the facial nerve by the released toxins and inflammation. There are reports of delayed improvement of nerve function in both cases associated with COM and traumatic fractures. The delay in surgery has a detrimental effect on the prognosis, but some patients have improvement with function in surgery delayed by 3- 5 months [1, 2]. Delayed nerve decompression in the present scenario has a definitive role in contrast to the traditional teachings. Surgical intervention is indicated if the Electroneuronography (ENoG) shows > (90%) degeneration within 3 weeks or Electromyography (EMG) shows total denervation potentials after 3 weeks. However, this does not hold true with cases associated with COM. Simply the longer the delay is evident, the more damage to the nerve is observed [4]. So in cases of COM it is logical to intervene early if no improvement is noted on conservative management. Traditionally the poor prognostic factors for facial palsy improvement are, longer duration of facial palsy to surgery interval, progressive onset of palsy, cholesteatoma, prior ear surgery and labyrinthine destruction [1]. In our case the improvement noted could be due to its association with granulation disease rather than a cholesteatoma, which is a major detrimental factor. The presence of only a partial palsy, an intact perineurium and lack of co-morbidities might have helped the nerve maintain its functional integrity all through.
Conclusion
The presence of partial palsy without cholesteatoma, and absence of co-morbidities is an ideal scenario where a trial of delayed nerve decompression can be provided as an option for facial rehabilitation. Though the chances are poor, but still a trial of nerve decompression is indicated as a last resort. The intactness of the perineurium and complete removal of the disease is vital to prevent further injury to the nerve and allow its regeneration.
Consent: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. Acknowledgments: None. Conflict of Interest: None.
References
-
Kim J, Jung GH, Park SY, Lee WS (2012) Facial Nerve Paralysis due to Chronic Otitis Media: Prognosis in Restoration of Facial Function after Surgical Intervention Yonsei Med J 53(3): 642-648.
-
Savic DL, Djeric DR. (1989) Facial paralysis in chronic suppurative otitis media. Clin Otolaryngol Allied Sci 14(6): 515-7.
-
Altuntas A, Unal A, Aslan A, Ozcan M, Kurkcuoglu S, et al. (1998) Facial nerve paralysis in chronic suppurative otitis media: Ankara Numune Hospital experience. Auris Nasus Larynx 25(2):169-172.
-
Sanus GZ, Tanriover N, Tanriverd T, Uzan M, Akar Z (2007) Late Decompression in patients with acute facial nerve paralysis after Temporal bone fracture. Turkish Neurosurgery 17(1): 7-12.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?