Posterior Semicircular Canal Dehiscence: Third Window to the Inner Ear- A Rare Cause of Vertigo
Posterior semicircular canal dehiscence is a very rare cause of vertigo and is suspected and evaluated rarely even after advent of good radiology. The prime cause for its late diagnosis is the varied presentations possible and also the multiple differential diagnosis that needs to be ruled out prior to diagnosing it. Here we are presenting a case of a 23 year old female who presented to us with noise induced vertigo for the past 4 years. She was evaluated to rule out other causes and was diagnosed with posterior semicircular canal dehiscence on radiology. The different treatment options were considered and patient was ultimately treated with conservative management with significant relief in morbidity. This paper tries to evaluate the possible options of management and considers the merits (risk benefit ratio) of surgical treatment versus conservative management.
Introduction
Canal dehiscence has been a well known entity in literature mostly associated with the lateral semicircular canal (LSCC). Since the description of superior semicircular canal dehiscence (SSCCD) by minor in 1998, it has been studied exhaustively and now is considered higher up in the differential diagnosis list of every clinician [1]. Posterior semicircular canal dehiscence (PSCCD) was described associated with a high jugular bulb in 1986 [2]. The PSCCD mimics numerous otological conditions, and usually patients are treated for other pathologies with no significant benefit. Thus the morbidity the patient faces is very significant. This paper tries to enlighten the diagnostic lacunae and also evaluate the right mode of management for these patients, questioning the need for surgical management in all patients.
A 23 year old female presented with the complaint of vertigo for the past 4 years. The vertiginous attacks were episodic, objective in nature, and lasted 5-10 minutes Otolaryngology Open Access Journal
each. The patient was completely asymptomatic in between attacks. It was reported that vertigo was often precipitated by loud sounds and sudden head movements. No associated hearing loss or tinnitus was reported. The patient also specifically reported of a dangerous difficulty with driving a two-wheeler on city roads as she was liable to get sound provoked vertigo from loud vehicular horns.
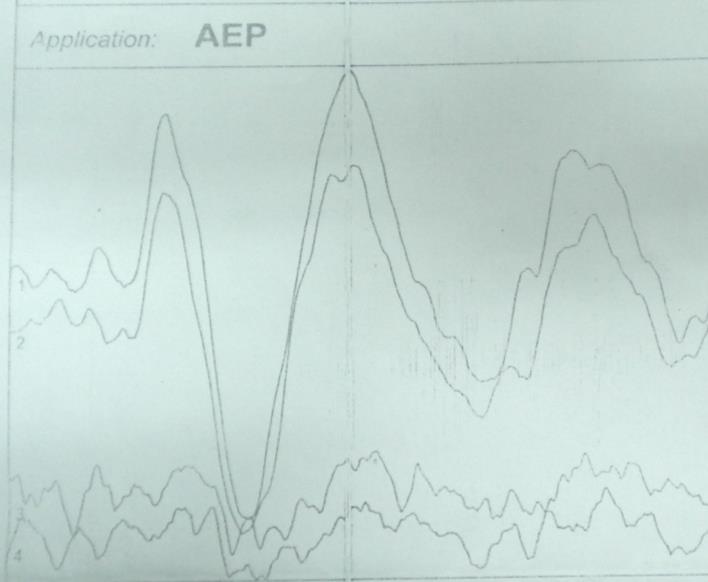
Examination of the ears and general systemic examination were normal. Neuro-otological evaluation by assessment of both vestibule - spinal and vestibule - ocular tests was entirely normal. The fistula sign was negative and no deficit was noted on evaluation of the cranial nerves or cerebellar signs. Pure tone audiometry (PTA) indicated normal hearing thresholds, and tympanometry was noted as normal with normal acoustic reflexes. The patient was also directly questioned for any giddiness while undertaking these tests and she reported of a sensation of mild giddiness provoked by pta testing, at 80 db more on the right side as compared to the left. The differential diagnosis at this stage included the possibilities of endolymphatic hydrops, inner ear inflammation, possible perilymphatic fistula, and the 3rd window phenomenon (semicircular canal dehiscence). Syphilis was excluded by appropriate serology. Vestibular evoked myogenic potential testing (500hz, 5/second, tone burst at 90-100 db ) indicated to a high amplitude response at low threshold on the right side thus confirming the tendency for increased vestibular responses to sound (figure-1).
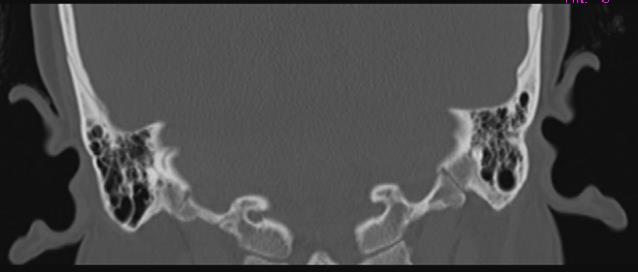
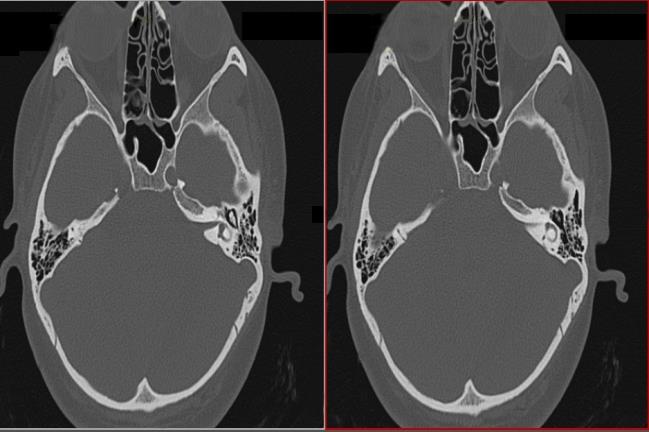
HRCT (High Resolution Computed Tomography) temporal bone with 1mm non-overlapping contiguous cuts demonstrated the right posterior semicircular canal to be dehiscent at its dome on the medial surface of the temporal bone (figure 2). No dense labyrinthine bone was noted medial to the right posterior semicircular canal (PSCC), and the appearance on HRCT was of the PSCC lumen being contiguous with the posterior cranial fossa contents. A diagnosis of right sided PSCCDEHISCENCE (PSCCD) with dehiscence towards the posterior cranial fossa was made.

The surgical options of treatment i.e. semicircular canal resurfacing and semicircular canal plugging were both explored. The potential risks to hearing with surgical treatment, as also the non-surgical alternatives were also Otolaryngology Open Access Journal
discussed. The non-surgical option offered included a full explanation of the mechanism of vertigo and the precipitating factors, the use of fitted ear plugs for noisy situations, and individualized lifestyle modification (avoidance of driving a two wheeler). The patient decided to defer the surgical option and has had significant relief in symptoms with the conservative life style options offered.
Discussion
The understanding of tullio’s phenomenon (sound provoked vertigo) has progressed significantly from the time of its first recognition in 1929. While it was initially supposed to be caused by sound waves just preferentially moving into the new opening, the emergence of radiology has made us aware that the commonest cause of the same is a “3rd window” in the inner ear. In normal circumstances, the round window in the cochlea acts as a pressure release mechanism and sound pressure entering from the oval window is therefore preferentially dissipated towards the cochlea. The presence of a “3rd window” in the vestibular portion of the inner ear leads to pressure also being dissipated towards the vestibule, thus leading to stimulation of the vestibular epithelium and consequent vertigo. The typical constellation of clinical features of the tullio’s phenomenon, giddiness on pta testing, and prominent vemp waveforms led us to the diagnosis. HRCT is considered e the cornerstone for the diagnosis with a reported sensitivity of (100%) and specificity of (99%) [3]. Since vestibular 3rd windows have been almost exclusively noted in the superior SCC, and since specific VNG testing to discern the variations in nystagmus between different variants was not undertaken, it was presumed to be the only site initially. The HRCT was undertaken with the intent of confirmation of the superior SSCCDEHISCENCE (SSCCD), but instead noted the vestibular dehiscence to be at posterior SCC (PSCCD). SSCCD is usually noted in the 4th to 6th decade and is presumed to result from pressure erosion from Dural pulsations in the floor of the middle cranial fossa. PSCCD is in contrast extremely rare and only few cases have been reported in the literature. It has been most commonly noted at the interface of the PSCC and the jugular foramen or at its dome adjacent to the posterior cranial fossa [4]. As with SSCCD the patients of PSCCD can present with both acoustic and vestibular symptoms and just pulsatile tinnitus. The fact why some have predilection for either one group of symptoms is still not clear. The prominent symptoms which guided us were the complaints of vertigo on exposure to loud noise and the development of giddiness on pta testing. The patients can present with either conductive, mixed, pure sensor neural hearing loss or a normal hearing thresholds4 as in our case. The literature describes a mixed hearing loss (67%) as the most common mode of presentation [3]. But a normal hearing level does not rule out pathology. Suprathreshold values on pta and hyperacusis to bone conducted sounds are commonly seen and are highly suggestive. The possible hypothesis for hyperacusis are due to 3rd window acting as a amplifier of bone conducted sounds or the air conduction sound energy being dissimilated through the 3rd window [5]. The importance of ruling out other pathologies is very essential as an PSCCD can be presenting an asymptomatic person also. The incidence of PSCCD according to European radiographic survey was (4.5%) [6]. But a possibility of selection bias was considered as only patients of vertigo were evaluated. The literature associates a high jugular bulb (70%) [3]. To be common etiological factor, more so on the right side due to the dominant circulation on the right. But as in our case the lack of high jugular does not rule out an existing pathology, suggesting a role of other etiological factors like benign intracranial hypertension, trauma, cholesteatoma, fibrous dysplasia etc. The literature tends to advocate surgical treatments for SSCCD. The surgical experience is primarily based on SSCCD and includes two options - canal resurfacing and canal plugging [7]. Canal resurfacing covers the dehiscence on the dome of the SCC so as to close the 3rd window and so reestablish normal physiology. For SSCCD, access is obtained by a subdural approach along the floor of the middle cranial fossa, and such access is relatively risk free. A similar subdural approach to access the PSCCD along the lateral surface of the posterior cranial fossa as required in this case could potentially be undertaken by the retro labyrinthine or retrosignoid approach. Access by either of these approaches would however necessitate manipulation of the endolymphatic sac and duct which are placed poster medial and medial and to the PSCC and thus risk inner ear injury. The other surgical option of canal plugging by the trans-mastoid route works by obliterating the canal lumen at a point between the SCC cupula and the dehiscence and seems potentially safer. The literature on canal plugging for SCCD is currently limited and has been noted to provide upto (70%) relief in symptoms [7]. PSCC canal plugging has been more frequently advocated for persistent BPPV, and the experience for this indication Otolaryngology Open Access Journal
report of a risk of sensor neural hearing loss upto (5%) [7]. In the particular case being reported the dehiscence was seen to extend to the common crus with the superior SCC; an attempt at canal occlusion would therefore have necessitated occlusion of both the SSCC and the PSCC and further magnified the risks to hearing. It does seem therefore that an entirely risk free and effective surgical treatment for PSCCD is currently unavailable. In one case reported in literature canal plugging resulted in upto (75%) decrease in symptoms [7]. But as in our case a patient with normal hearing and good relief with conservative measures raises the doubt if surgical procedure is required, as even it produces only a partial relief. The best way to plan the management action would be to individualize the management according to the morbidity caused to the patient, rather than making a rigid plan of action.
Conclusion
The diagnosis of PSCCD needs a constellation of symptoms and signs, along with radiology and vemp. All the factors are important and complement each other in guiding to a diagnosis. The finding of a PSCCD in an asymptomatic person does not warrant a treatment. The treatment must be individualized and all patients must receive a conservative approach initially if there is no significant hearing loss. Surgical management should be preserved for severe cases and if patients are willing to take the risk and they should be explained about the partial response expected.
References
-
Minor Lb, Solomon D, Zinreich Js, Zee DS (1998) Sound- and/or pressure-induced vertigo due to bone dehiscence of the superior semicircular canal. Arch Otolaryngol Head Neck Surg 124(3): 249-258.
-
Wadin K, Thomander L, Wilbrand H (1986) Effects of a high jugular fossa and jugular bulb diverticulum on the inner ear. A clinical and radiologic investigation. Acta Radiol Diagn (Stockh) 27(6): 629-636.
-
Minor Lb (2005) Clinical Manifestation of Superior Semicircular Canal Dehiscence. Laryngoscope 115(10): 1717-1727.
-
Quinton Gopen, Zhou G, Poe D, Kenna M, Jones D (2010) Posterior semicircular canal dehiscence: first reported case series. Otol Neurotol 31(2): 339-344.
-
Merchant S, Rosowski J (2008) Conductive hearing loss caused by third window lesions of the inner ear. Otol Neurotol 29(3): 282-289.
-
Krombach Ga, Dimartino E, Schmitz-Rode T, Prescher A, Haage P, et al. (2003) Posterior semicircular canal dehiscence: a morphologic cause of vertigo similar to superior semicircular canal dehiscence. Eur Radiol 13(6): 1444-1450.
-
Mikulec AA, Poe DS (2006) Operative management of a posterior semicircular canal dehiscence. Laryngoscope 116(3): 375-378.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?