The Role of Collaborative Diagnosis in Identifying Nevoid Basal Cell Carcinoma Syndrome: A Vigilant Radiologist Helping a Surgeon
Nevoid basal cell carcinoma syndrome is a rare inherited condition caused by mutations in the PTCH1 gene. It causes a wide range of developmental abnormalities. These patients are encountered by otolaryngologists and radiologists initially presenting with the odontogenic keratocysts affecting maxilla and mandible. Multiple basal cell carcinomas, pits in palmoplantar region and jaw cysts are cardinal features. Often surgeons are unfamiliar with the different manifestations leading to failure to diagnose the condition. A vigilant radiologist can help in the diagnosis and potentially preventing the sequelae.
Case Report
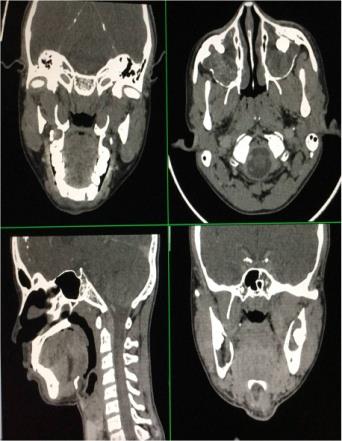
A 27 year old male, presented in the department of otolaryngology with progressive bilateral maxillary swelling since childhood causing substantial disfigurement, there was history of intermittent nasal obstruction; with no history pain, sinus, facial heaviness or epiphora. The patient had no other complaints. The patient was provisionally diagnosed as a case of odontogenic tumor and a contrast enhanced CT scan of face, nose and paranasal sinuses, 1-1.5 mm sections, both in soft tissue and bone window settings; axial, coronal and sagittal view was advised. In the department of radiology, contrast enhanced CT scan of face and paranasal sinuses (bone and soft tissue window) showed multiple cystic expansile lesions with unerupted teeth suggestive of odontogenic keratocysts. Incidentally the visualized portion of the brain and cranium in the CT scan of face revealed calcification of falx cerebri and tentorium cerebelli raising the suspicion of nevoid basal cell carcinoma syndrome. The patient was then thoroughly investigated by the radiologists and a chest X-Ray was done which showed the classical picture of bifid and fused ribs. And finally the case was radiologically reported as a possible case of nevoid basal cell carcinoma syndrome. This vigilant reporting encouraged the otolaryngologists to closely examine the patient for any basal cell nevus or carcinoma. An asymptomatic retro-auricular ulceronodular lesion was detected which was present there for over an year. It looked suspicious and was excised with adequate margins (1 cm from the palpable margins) and on histopathological examination showed features of basal cell carcinoma. The odontogenic keratocyst was excised too with a guarded prognostication for relapse. Also multiple nevi were present at the back. No family history of facial swellings and basal cell naevi was present (Figure 1-3).


Discussion
Nevoid basal cell carcinoma syndrome was first reported by Jarish in 1894 [1]. Gorlin and Goltz in 1960 gave the complete description and of the new syndrome [1]. Nevoid basal cell carcinoma usually present at the first, second or third decade [2]. There are so many other confusing names of the syndrome including Gorlin syndrome, basal cell nevus syndrome, syndrome of jaw cysts, hereditary cutaneo mandibular polyonocosis or jaw cyst-basal cell nevus-bifid rib syndrome [3, 4]. Gorlin had suggested the term nevoid basal cell carcinoma syndrome, however all the affected patients did not have basal cell carcinomas. Nevoid basal cell carcinoma is inherited by autosomal dominant mode, but can have a variable phenotypic penetration, or can have sporadic presentation as seen in our case [5]. This syndrome is associated with a wide spectrum of developmental anomalies and neoplasms. Keratocystic odontogenic tumor or odontogenic keratocyst is usually the first feature of the syndrome. The tumor is typically found as incidental radiographic findings or may present as jaw swellings. It has been suggested that multiple OKCs alone may be confirmatory of the syndrome [6]. Although benign, the recurrence rate after excision of OKC is very high, ranging from 12 to 62.5% and multiple recurrences are not unusual [7]. The PTCH 1 gene, the human homologue of the Drosophila segment polarity gene, has been seen to be involved in the development of Gorlin- goltz syndrome [8, 9]. Odontogenic keratocystic tumors in Gorlin-Goltz syndrome comprise unilocular or multilocular radiolucencies of the mandibular body, angle, or ramus [2]. In children and adolescents, the cysts may cause displacement of developing teeth and delayed dental development with associated impacted tooth [7]. The most frequent skin lesions of Gorlin-Goltz syndrome are cutaneous basal cell carcinomas, benign dermal cysts, and palmar and plantar keratosis or pits [2, 7]. Ectopic calcification of falx cerebri, tentorium cerebella, and bridged sella may also be detected radiologically [7]. The patient usually has cranio-facial anomalies comprising of frontal and parietal bossing and broad nasal root which may be associated with ocular hypertelorism [2]. Thoracic cage anomalies such as bifid and fused ribs may be present as classically seen in two of our cases. Syndactyly or polydactyly of toes may be the other skeletal abnormalities along with kyphosis and scoliosis [2]. The diagnosis of Gorlin-Goltz syndrome requires the presence of two major or one major and two minor criteria [7, 9](Table 1).
| Major Criteria | Minor Criteria |
|---|---|
| Multiple Bcc | Macrocephaly |
| Odontogenic Keratocyst | Congenital Malformation |
| Palmar/ Plantar Pits | Skeletal Anomaly |
| Calcified Falx Cerebri | Radiologic Anomaly |
| Bifid/ Fused Rib | Ovarian Fibroma |
| 1stDegree Relative | Medulloblastoma |
Table 1: Criteria for Diagnosis.
The clinical management includes surgical treatment (enucleation and peripheral ostectomy) of the lesions [10]. Addressing the risks associated with syndrome, the development of neoplasm’s on sun or radiation exposure, recurrent odontogenic keratocysts etc., warrants utmost importance. Thus a regular follow up, interdisciplinary cooperation for the diagnosis, treatment and rehabilitation is required. All the patients were counseled regarding the syndrome and are kept under active follow- up/surveillance for early detection of cutaneous malignancies and other sequelae of the syndrome.
Conclusion
The patients affected by Gorlin-Goltz syndrome must be evaluated by several relevant specialists to precisely confirm the diagnosis. Early diagnosis and treatment may reduce the severity of the long term sequelae of Gorlin- Goltz syndrome including malignancy and oral maxillofacial deformation and destruction.
References
-
Jones EA, Sajid MI, Shenton A, Evans DG (2011) Basal cell carcinomas in gorlin syndrome: A review of 202 patients. J Skin Cancer 2011: 217378.
-
Kantarci M, Ertas U, Alper F, Sutbeyaz Y, Karasen RM, et al. (2003) Gorlin's syndrome with a thin corpus callosum and a third ventricular cyst. Neuroradiology 45(6): 390-392.
-
Kalogeropoulou C, Zampakis P, Kazantzi S, Kraniotis P, Mastronikolis NS (2009) Gorlin-Goltz syndrome: incidental finding on routine CT scan following car accident. Cases J 2: 9087.
-
Hisatomi M, Asaumi J, Konouchi H, Shigehara H, Yanagi Y (2003) MR imaging of epithelial cysts of the oral and maxillofacial region. Eur J Radiol 48(2): 178- 182.
-
Ortega de GAA, García AO, Zepeda NS, Acha SA, Aguirre UJM (2008) Gorlin-Goltz syndrome: clinicopathologic aspects. Med Oral Patol Oral Cir Bucal 13(6): E338-E343.
-
Lo Muzio L, Staibano S, Pannone G, Bucci P, Nocini PF, et al. (1999)Expression of cell cycle and apoptosis- related proteins in sporadic odontogenic keratocysts and odontogenic keratocysts associated with the nevoid basal cell carcinoma syndrome. J Dent Res 78(7): 1345-1353.
-
Jawa DS, Sircar K, Somani R, Grover N, Jaidka S (2009) Gorlin-Goltz syndrome. J Oral Maxillofac Pathol 13(2): 89-92.
-
Boutet N, Bignon YJ, Drouin-Garraud V, Sarda P, Longy M, et al. (2003) Spectrum of PTCH1 mutations in French patients with Gorlin syndrome. J Invest Dermatol 121(3): 478-481.
-
Larsen AK, Mikkelsen DB, Hertz JM, Bygum A (2014) Manifestations of Gorlin-Goltz syndrome. Dan Med J 61(5): A4829.
-
Rai S, Gaubak K (2007) Jaw cyst-Basal cell nevus-Bifid rib syndrome: a case report. J Indian Soc Pedod Prev Dent 25(3): 137-139.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?