Juvenile Nasopharyngeal Angiofibromas: Blood, Sweat, Tears and Fresh Ideas-how we do it
Aim Introduction: Management of advanced juvenile nasopharyngeal (JNA) angiofibroma is plagued with surgical frustration, largely because of its propensity for haemorrhage. To minimise blood loss and the need for allogenic blood transfusion we routinely use preoperative embolisation and intra-operative cell salvage.Although endoscopic surgery is now standard of care in many centres, the resection of large tumours with infratemporal fossa extension can be challenging. A combined open and endoscopic approach is often reported for very large tumours if dissection around the tumour is not possible. We have found that the endoscopic Denker's approach, together with the use of cell salvage allows for complete endoscopic resection without the need for any external procedures. Cell salvage allows for more intra-operative blood loss with a rare need for allogenic transfusion. Method: We describe the current treatment protocol for all JNA tumours at our institute showing that complete endoscopic resection is possible using the Denker's approach together with intra-operative cell salvage. Aim: This paper explains how adequate endoscopic access may be gained to dissect around these tumours without the need for debulking. The added benefit of cell salvage during endoscopic resection is discussed.
Background
JNAs are a vasoproliferative malformation that occur due to an uncontrolled process of wound healing and granulation [1] and chromosomal imbalances have been found in both stromal and endothelial cells [2, 3]. JNAs are challenging to manage due to the location, vascularity and size of the tumour at time of diagnosis. For a complete resection, two factors are important-hemostasis and access. Firstly, hemostasis can be achieved by pre- operative embolization, dissecting around the tumour thereby devascularising it further and by using intra- operative cell salvage. Secondly, access is vital and although the traditional open approaches provide wide access, resection of tumour in the area of the basisphenoid, cavernous sinus and infratemporal fossa is often without adequate visualisation. Spontaneous regression, although unusual, has been described and when noted, is extremely slow [4, 5, 6]. The tumour may decrease in aggressiveness as it enters its third decade [7] but currently there are no centres that routinely advocate watchful waiting with regular imaging [8]. After surgical resection, the incidence of residual and recurrent tumours varies significantly in the literature from 10% to 50% [9, 10, 11, 12, 13]. There is evidence that endoscopic surgery has equivalent, if not lower rates of recurrent and residual disease compared to open surgical procedures [10, 14, 15]. Recurrent disease usually occurs within 3 years of surgery [16]. There is some evidence to opt for a conservative approach in managing patients with small tumour remnants due to the belief that the tumour may involute [16]. 86% of patients would be expected to be disease free at long-term follow-up [16]. The leading cause for recurrence is incomplete surgical resection [17]. Larger, more advanced tumours carry greater risk [9, 18]. Independent risk factors include extension into the basisphenoid, erosion of the clivus, intracranial extension medial to the cavernous sinus, invasion of the sphenoid diploe through a widened pterygoid canal and developing a JNA at a young age [12].Radiotherapy may be associated with complications like malignant transformation, hypopituitarism, osteoradio-necrosis and cataracts [9, 16]. Clinical experience with newer techniques, such as intensity modulated radiotherapy and radio surgery remains limited; [19, 20] and therefore does not form part of our treatment protocol. At the University of Cape Town, we have adapted a standard protocol for managing JNA and all tumours are resected endoscopically, regardless of staging, with minimal blood transfusion requirements. The use of cell salvage has made complete tumour resection possible even if blood loss is extensive [21].
Method
The last 15 cases have all been performed using the following protocol: Pre-operative embolisation 2-5 days prior to surgery. Particles are used to flood the tumour bed and feeding vessels, specifically the internal maxillary artery (IMA). It is important to flood the tumour bed in order to minimise bleeding during tumour manipulation. Embolising the IMA proximally is important when an endoscopic resection is planned (Figures 1-2).
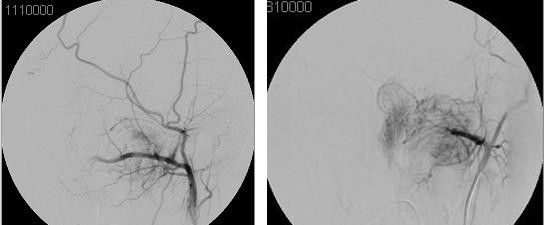
Figures 1-2: Angiography serves the dual purpose of being diagnostic and therapeutic. Image 6 shows the typical “tumour blush”. Image 7 shows the same tumor after embolisation of the internal maxillary artery.
Surgical steps are performed in the following order:
- Endoscopic Denker’s approach for lateral access to the tumour (Figures 3-4)
- Tumour devascularisation by dissecting around the JNA, avoiding debulking of the tumour until adequate devascularisation has been achieved.
- First, a lateral dissection to the IMA and the lateral infratemporal fossa component
- Dissection of tumour off the anterior skull base and fovea ethmoidalis
- Dissection of tumour within the sphenoid sinus and basisphenoid
- Nasopharyngeal dissection and release of tumour off the posterior nasal septum
- Delivery of tumour through the oral cavity (Figures 5- 6)
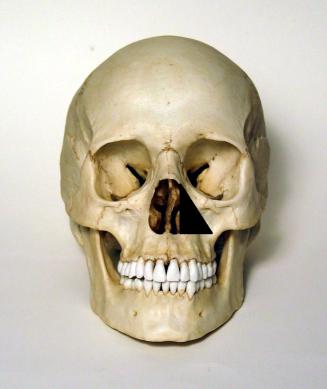
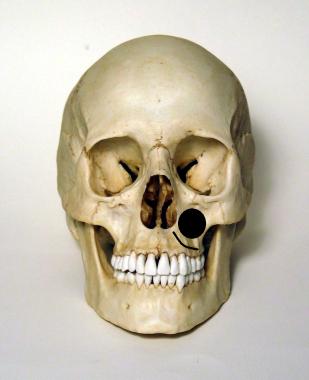

Figure 5-6: En bloc resection of large tumours is possible using and endoscopic Denker’s approach, preoperative embolisation and intraoperative cell- salvage blood transfusion.
How we do it
Pre-operative assessment: Patients are assessed prior to surgery, using CT and MRI, to establish the extent of the tumour and the anatomical landmarks.The archetypal angiographic appearance is a “tumour blush” and absence of venous filling (Figures 1-2). The major arterial supply is provided by the ipsilateral maxillary artery, with occasional additional vessels from branches of the ICA or contralateral external carotid artery (ECA) system [13]. Pre-operative embolisation: Embolisation consists of small particles that flood the tumour bed and is performed 2–7 days prior to surgical resection. At least 48hrs is required to prevent significant bleeding from the tumour. It is not advisable to wait more than 7 days since the tumour becomes hard and fibrotic and difficult to manipulate and resect after this period. Preoperative embolisation has been proven to decrease intraoperative blood loss [9, 10, 13, 16]. This is especially essential in larger tumours that are supplied by additional feeder vessels. Anaesthesia: Total intravenous anaesthesia (TIVA) is essential, the requirements being a normotensive patient with a slow heart rate [13]. Patients are given 48 hours of antibiotics to prevent bacteraemia from cell salvage blood transfusion [21]. Intraoperative cell salvage blood transfusion is used to avoid allogenic blood transfusions, eliminating the risk of developing transfusion associated complications. Our transfusion trigger is intra-operative haemoglobin of less than 7g/dL and a rising trend in the base excess. There was some concern about using blood from a contaminated field but post-operative blood culture results showed no bacterial growth with the use of a leukocyte filter [21]. Access: Adequate access is imperative and is obtained by doing a transnasal endoscopic medial maxillectomy to expose the whole posterior wall of the maxillary sinus. The endoscopic transnasal approach can be used for tumours involving the sinonasal cavity, the pterygopalatine fossa with infratemporal fossa extension and tumours pedicled on the sphenoid rostrum or invading the sphenoid sinus with extension to the cavernous sinuses. A combined open and endoscopic approach is occasionally needed for tumours with extensive infratemporal fossa extension; although by utilising the Denker’s approach we have managed to avoid any additional external approach. The endoscopic Denker’s approach allows for adequate access to the far lateral infratemporal fossa. (Figures 7-8) A Caldwell-Luc sub-labial incision with a maxillary sinusotomy can still be utilized for those not familiar with the Denker’s approach (Figures 3-4).
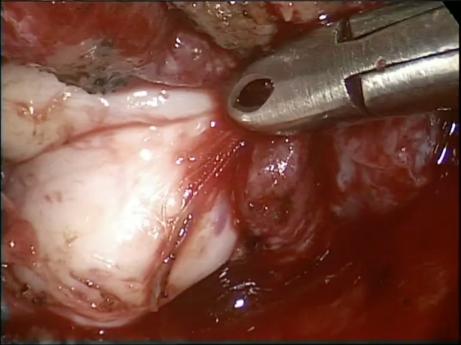
Figure 8: Axial CT scan showing tumour extending into the infratemporal fossa. Surgery: En-bloc resection is the author’s preference. This is achieved by dissecting around the tumour thereby avoiding bleeding from the larger tumour vessels. However, it is only possible if adequate surgical access is obtained. Larger tumours often require debulking to provide access within the nasal cavity to manipulate instruments and allow for 4-handed surgery. This can be achieved using a microdebrider or by piecemeal resection using bipolar cautery and scissors. Extensive bleeding can be a limiting factor despite adequate pre-operative embolisation and debulking is avoided if possible. Once the lateral aspect of the tumour has been identified, the skull base and fovea ethmoidalis are exposed superior to the tumour (via a fronto- ethmoidectomy). Dissection continues posteriorly to reach the sphenoid sinus, where the planum is identified and tumour is peeled off the roof, and the posterior and lateral wall of the sphenoid sinus. Be aware that the ICA may be dehiscent and no traction should be applied on tissues in this area. The tumour is rolled out of the sphenoid sinus, over the rostrum of the sphenoid. The tumour is usually adherent to the rostrum of the sphenoid and significant bleeding can occur during this part of the dissection. The vidian artery (a branch of the ICA) is located at the level of the floor of the sphenoid sinus and needs to be cauterized/ligated since embolisation is unable to address the ICA system. A combination of bipolar dissection/laser dissection is required with frequent packing to tamponade the bleeding. Profuse bleeding at this stage of the dissection is usually secondary to hemorrhage from either the vidian artery or the ophthalmic artery and could lead to the procedure being abandoned. Once the tumour is freed off the rostrum, posterior nasal septum and nasopharynx, the lateral aspect is addressed. Care must be taken to avoid disrupting the internal maxillary artery proximally. The tumour is gently retracted towards the midline of the nose while the laser or bipolar is used to obtain a dissection plane between the normal tissue and angiofibroma. The 4-handed approach is essential during this stage. The pterygoid plates may require drilling down but this is usually not required. The tumour is finally pushed into the nasopharynx and delivered through the oral cavity. Post-operative packing consists of a hemostatic (NexStat®) powder only. All patients require a MRI 3 months post-surgery to assess for residual tumour [9].
Results
Fifteen patients were treated in our unit. The patients were staged according to the University of Pittsburgh Medical Center’s Classification for endoscopic resection of JNA tumors: [18]. Stage 2-9 patients Stage 3-4 patients Stage 4-2 patients The data were nonparametric. Median blood loss was 700mL (minimum 200mL; maximum 4000mL; interquartile range 400mL-1350mL). Median blood transfusion was 300mL (minimum 0; maximum 2500mL; interquartile range 200mL-650mL). Mean hospital stay was 2 days.
Discussion
External approaches were originally the only option for tumour resection [10]. Although open surgery allows for wide access, visualisation of the basisphenoid area, cavernous sinus and infratemporal fossa are limited and injury to vessels in these areas can result in tremendous blood loss. Transpalatal approaches were used for tumours isolated to the nasopharynx and a Caldwell Luc approach was used to access the pterygomaxillary area [10]. More lateral tumours were accessed by a lateral rhinotomy and transnasal/transantral approach [10].Tumours involving the lateral infratemporal fossa were originally regarded to be a contraindication to endoscopic surgery alone [10]. However, with increasingly skilled anterior skull base surgeons and instrument development, it has been described for advanced tumors [22]. The endoscopic Denker’s approach allows for greater access to the lateral infratemporal fossa, using a zero degree endoscope and straight instrumentation. Endoscopic resection is associated with lower morbidity and it has at least equivalent complication and recurrence rates compared to open techniques [10]. Preoperative embolization has further reduced blood loss [10] and our unit is the first to describe autologous blood transfusion use during anterior skull base surgery [21]. It has the added advantage of reducing the risk of blood transfusion related complications and does not increase the risk of bacteraemia if a leukocyte filter is used [21].
Conclusion
By utilizing an endoscopic Denker’s approach in combination with pre-operative embolization and intra- operative cell salvage blood transfusion, we have been able to resect large tumours en bloc without the need for autologous blood transfusion.
References
-
Beham A, Beham SC, Regauer S, Aubock L, Stammberger H (2000) Nasopharyngeal angiofibroma: true neoplasm or vascular malformation? Adv Anat Pathol 7(1): 36-46.
-
Coutinho CCM, Brentani MM, Nagai MA (2008) Genetic alterations in juvenile nasopharyngeal angiofibromas. Head Neck 30(3): 390-400.
-
Silveira SM, Custódio DMA, Butugan O, Brentani MM, Rogatto SR (2012) Tumor microenvironmental genomic alterations in juvenile nasopharyngeal angiofibroma. Head Neck 34(4): 485-492.
-
Lloyd G, Howard D, Phelps P, Cheesman A (1999) Juvenile angiofibroma: the lessons of 20 years of modern imaging. J Laryngol Otol 113(2): 127-134.
-
Weprin LS, Siemers PT (1991) Spontaneous regression of juvenile nasopharyngeal angiofibroma. Arch Otolaryngol Head Neck Surg 117(7): 796-799.
-
Jacobsson M, Petruson B, Ruth M, Svendsen P (1989) Involution of juvenile nasopharyngeal angiofibroma with intracranial extension. Arch Otolaryngol Head Neck Surg 115(2): 238-239.
-
Bhatia ML, Mishra SC (1967) Intracranial extensions of juvenile angiofibroma of the nasopharynx. J Laryngol Otol 81(12): 1395-1403.
-
Spielmann PM, Adamson R, Cheng K, Sanderson RJ (2008) Juvenile nasopharyngeal angiofibroma: spontaneous resolution. Ear Nose Throat J 87(9): 521-523.
-
Liu L, Wang R, Huang D, Han D, Ferguson EJ, et al. (2002) Analysis of intra-operative bleeding and recurrence of juvenile nasopharyngeal angiofibromas. Clin Otolaryngol Allied Sci 27(6): 536-540.
-
Khoueir N, Nicolas N, Rohayem Z, Haddad A, Abou HW (2014) Exclusive endoscopic resection of juvenile nasopharyngeal angiofibroma: a systematic review of the literature. Otolaryngol Head Neck Surg 150(3): 350-358.
-
Herman P, Lot G, Chapot R, Salvan D, Huy PT (1999) Long-term follow-up of juvenile nasopharyngeal angiofibromas: Analysis of recurrences. Laryngoscope 109(1): 140-147.
-
Tyagi I, Syal R, Goyal A (2007) Recurrent and residual juvenile angiofibromas. J Laryngol Otol 121(5): 460- 467.
-
Panda NK, Gupta G, Sharma S, Gupta A (2012) Nasopharyngeal Angiofibroma-changing Trends in the Management. Indian J Otolaryngol Head Neck Surg 64(3): 233-239.
-
Mann WJ, Jecker P, Amedee RG (2004) Juvenile Angiofibromas: Changing Surgical Concept over the Last 20 Years. Laryngoscope 114(2): 291-293.
-
Pryor SG, Moore EJ, Kasperbauer JL (2005) Endoscopic versus Traditional Approaches for Excision of Juvenile Nasopharyngeal Angiofibroma. Laryngoscope 115(7): 1201-1207.
-
Leong SC (2013) A systematic review of surgical outcomes for advanced juvenile nasopharyngeal angiofibroma with intracranial involvement. Laryngoscope 123(5): 1125-1131.
-
Fagan JJ, Snyderman CH, Carrau RL, Janecka IP (1997) Nasopharyngeal angiofibromas: selecting a surgical approach. Head Neck 19(5): 391-399.
-
Snyderman CH, Pant H, Carrau RL, Gardner P (2010) A new endoscopic staging system for angiofibromas. Arch Otolaryngol Head Neck Surg 136(6): 588-594.
-
Roche PH, Paris J, Regis J, Moulin G, Zanaret M, et al. (2007) Management of invasive juvenile nasopharyngeal angiofibromas: the role of a multimodality approach. Neurosurgery 61(4): 768- 777.
-
Álvarez FL, Suárez V, Suárez C, Llorente JL (2013) Multimodality approach for advanced-stage juvenile nasopharyngeal angiofibromas. Head Neck 35(2): 209-213.
-
Wasl H, McGuire JK, Lubbe D (2016) Avoiding Allogenic Blood Trasfusions in Endoscopic Angiofibroma Surgery. J Otolaryngol Head Neck Surg 45: 25.
-
Carrau RL, Snyderman CH, Kassam AB, Jungreis CA (2001) Endoscopic and endoscopic-assisted surgery for juvenile angiofibroma. Laryngoscope 111(3): 483- 487.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?