Case Report of a Primary Parotid Large Cell Neuroendocrine Carcinoma
Large cell neuroendocrine carcinoma (LCNEC) is quite rare in the salivary gland and is difficult to recognize with fine needle aspiration cytology (FNAC). Here, we present a case thought to be a lymphoma in FNAC but was diagnosed as LCNEC with the excision material. A 65-year old female patient was admitted with the complaint of a two-month old, rapidly growing painful mass in the right parotid region. FNAC was performed and it was reported as a malignant tumor, possibly lymphoma. A right superficial parotidectomy and right neck dissection were performed. The case was diagnosed as LCNEC of the parotid gland. The patient was given postoperative radiotherapy. No relapse and metastases were detected in the two-year follow-up of the patient.
Introduction
There are currently four classifications of neuroendocrine tumors (NETs), like those used for lungs: well-differentiated= carcinoid tumor, moderately- differentiated= atypical carcinoid tumor, poorly- differentiated, small cell type = small cell carcinoma, and poorly-differentiated, large cell type = large cell neuroendocrine carcinoma (LCNEC) [1]. Recently, the WHO has separated NETs into three grades based on their proliferation index [2]. Grade 1 has a proliferation index of<2% (mitotic count of <2 per 10 high power fields), grade 2 has well-differentiated NETs and proliferation index 2–20% (mitotic count of 2–20 per 10 high power fields), and grade 3 has NEC and a proliferation index >20% (mitotic count of >20 per 10 high power fields).
Grade 3 can be large cell or small cell type. LCNEC was first defined for the lungs but has also been observed in the cervix, colon, thymus, stomach, gall bladder and bladder [3]. Initially, LCNEC was not a specific entity in the head and neck area; however, recent studies have shown that these tumors fulfill LCNEC criteria and should be regarded as a new entity since they are high grade [4]. LCNEC account for less than 1% of all salivary gland tumors. Kawartani, et al. [5] reported only eight such cases in a PubMed review of the last 40- years [5]. Most large cell neuroendocrine carcinomas contain the major salivary glands, and especially the parotid gland. Peak incidence is in patients in their 7-8th decades and it is more widespread among males [6]. Here, we report a case initially thought to be a lymphoma in FNAC but later diagnosed as:
A 65-year old female patient was admitted with the complaint of a two-month old, rapidly growing painful mass in the right parotid region. The patient had Type 2 diabetes mellitus in her medical history. A hard, fixed mass measuring approximately 6×4cm was detected in the right parotid gland region during the physical examination and a few lymph nodes were palpated in the right cervical region. The patient underwent a head and neck computed tomography (CT). A space-occupying lesion was observed in the CT. It had a hypodense area in the center with irregular contours and maintained a circumferential contour of 26×20 mm in the right parotid gland. A few lymph nodes, the largest of which was 6×5 mm, were observed on the right, level 2. Atypical cells with a narrow cytoplasm, separately or in groups with a vesicular nucleus, were observed in the FNAC of the right parotid gland (Figure 1).
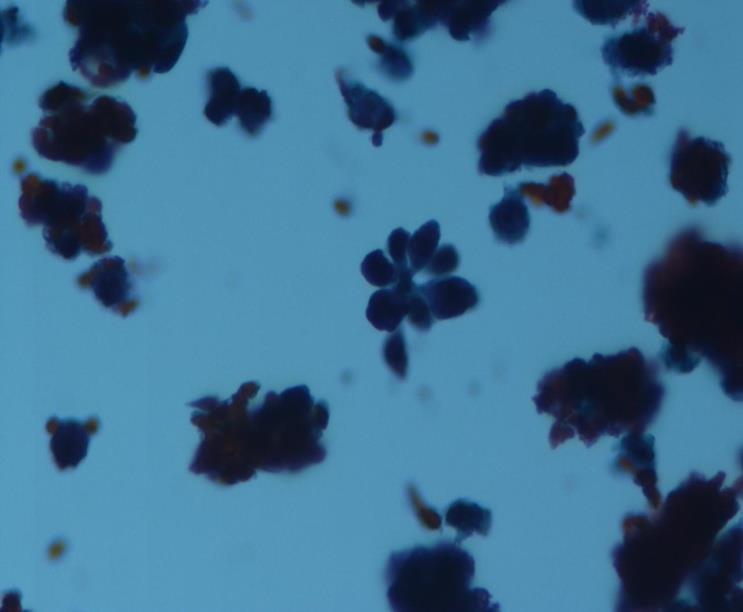
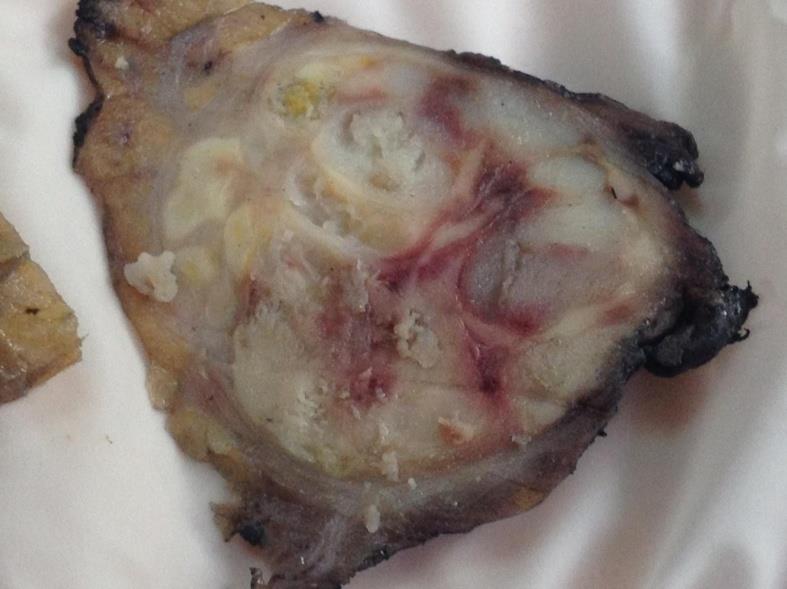
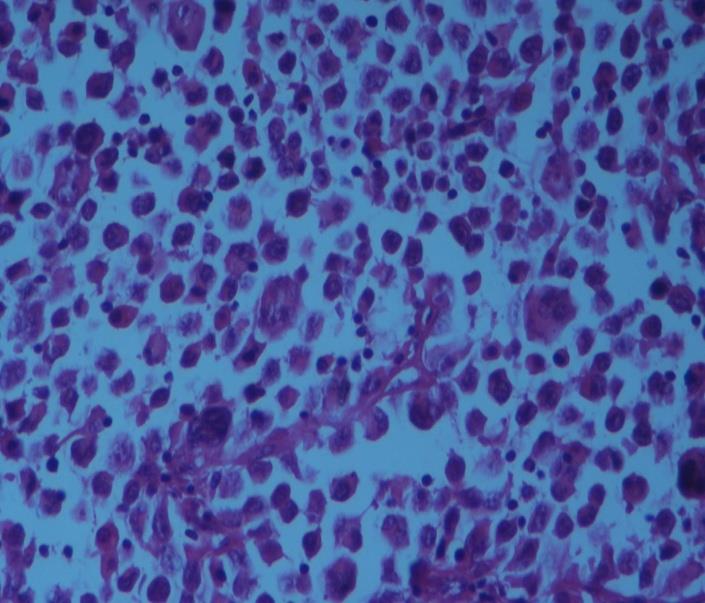
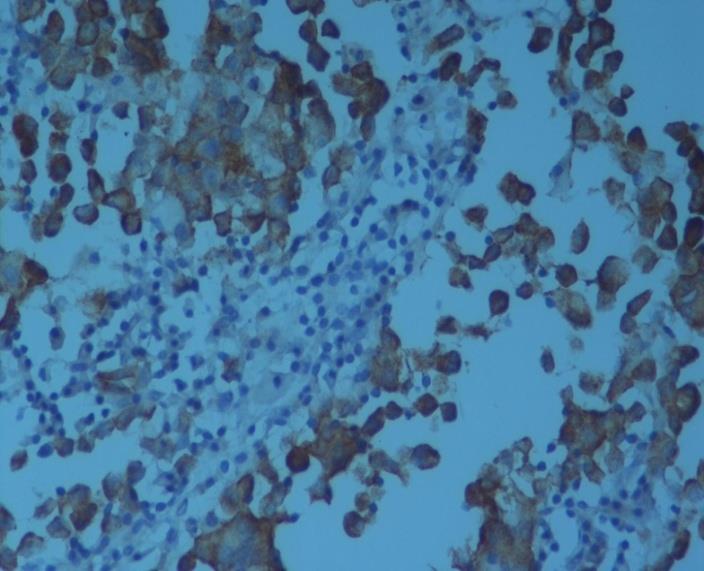
Figure 1: Atypical cells with a narrow cytoplasm, separately or in groups with a vesicular nucleus were observed in the FNAC (X40). The FNAC showed a malignant tumor, possibly large cell lymphoma. A right superficial parotidectomy and right neck dissection of levels 1–4 were performed on the patient. A well-defined, necrotic, off-white to yellow solid tumor measuring 4×2.5×2.5 cm was observed in the cross section of the salivary gland, which measured7.5×3.5×3 cm (Figure 2). A tumor was observed in the histopathological examination of the mass. It comprised cells with eosinophilic cytoplasm with prominent nucleoli, irregular nuclear contours, and pleomorphism. Tumor cells formed solid islands and cords. There were many mitotic figures, giant cells (Figure 3), large necrosis areas, perineural invasion, and mild lymphoplasmacytic cell infiltrations. NSE (Figure 4), CD56, and EMA were stained positively in the immunohistochemical examination.
TTF1, HMB45, Melan-A, Chromogranin, CD30, CK5, and CK7 were stained negatively. The Ki67 proliferation index was around 50%. The case was diagnosed as LCNEC based on these findings. No metastases were detected in Level 1–4 lymph nodes. Forty gray radiotherapy was given to the patient postoperatively because perineural invasion was reported in the pathology report. No relapse and metastases were detected in the two-year follow-up.
Discussion
Primary NETs of the head and neck area are rare. LCNEC is a new clinicopathological entity within the NET group (3). Primary NET derived from the larynx most frequently in the head and neck area, however, only 0.5– 1% of all tumors are located here. The larynx is followed by the parotid gland. Poorly-differentiated neuroendocrine carcinoma is more widespread among males [7] but our case is female. Histopathology and immunohistochemical examinations play an important role in diagnosing LCNEC. Histopathologically LCNEC contains organoid nesting with large polygonal-shaped cells, rosette trabeculae, giant cells, inflammatory cells, and frequent necrosis. Small ductal structures and squamous differentiation areas can be observed. Neuroendocrine markers are immunohistochemically positive and have >20% mitosis per 10 high power fields [6]. Our case was diagnosed as LCNEC based on its histopathological image, CD56 and NSE positivity of neuroendocrine markers, severe necrosis, and a >20% mitotic index. FNAC is valuable in diagnosis, though it can confuse LCNEC with other high-grade tumors since this LCNEC is high-nuclear graded and rare. Hence, it is obligatory to examine the excision material. Based on FNAC, the tumor was reported to be a lymphoma suspect due to its nuclear properties. The LCNEC differential diagnosis should consider adenoid cystic carcinoma, malignant melanoma, poorly-differentiated squamous cell carcinoma, metastasis, merkel cell carcinoma and as in our case, lymphoma. The immunohistochemical examination is also valuable in differential diagnosis.
LCNEC is immunohistochemically distinguished from malignant melanoma with the negativity of the markers such as S100, HMB45 and Mart-1 [8]. Immunohistochemical staining is helpful to rule out the differential diagnosis of a primary NET at the parotid gland from a distant metastasis from a NET with another primary origin. For example, TTF-1 is a sensitive marker for lung small cell carcinoma. TTF-1 also helps to rule out Merkel cell carcinoma, where it is consistently negative [9]. S100 is positive in the myoepithelial layer in adenoid cystic carcinoma. CK5/6 is positive in luminal cells. It is distinguished from lymphoma by the positivity of neuroendocrine markers, which also distinguished it from poorly-differentiated squamous cell carcinoma. Histological evidence of epithelial differentiation, as well as the identification of positive staining with leukocyte common antigen and other more specific T and B cell lymphoid markers (CD3, CD5, CD20) among others, can help distinguish LCNEC from malignant lymphoma [6]. Relapse and metastases are prevalent since LCNEC of the head and neck area is quite aggressive. Metastases are observed most frequently in cervical lymph nodes, liver, bones, skin and lungs. The survival rate is similar to that of small cell carcinoma of the lungs, with two-and-five- year survival rates of only 16% and 5%, respectively [10]. No relapse and metastases were detected in the two-year follow-up of our patient. The most common treatment of LCNEC is excision and adjuvant radiotherapy (6). Others suggest postoperative radiotherapy and chemotherapy [3]. Postoperative radiotherapy was given to our patient.
Conclusion
LCNEC of the salivary gland may be confused with other tumors in FNAC; thus, it is crucial to examine the excision material and perform an immunohistochemical examination. Caution should be exercised in diagnosis since LCNEC is rare in the salivary gland and has an aggressive course. Early diagnosis and treatment are important to improve outcomes. Compliance with Ethical Standards Disclosure of potential conflicts of interest: There is no conflict of interest among the authors and this research has received no financial grant from any funding agency, commercial or not-for-profit sectors. Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institution research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent: Informed consent was obtained from patient.
References
-
Brandwein-Gensler M, Mahadevia P, Gnepp DR (2009) Laryngeal pathology. In: Fried MP, Ferlito A, (Eds.) The Larynx 3 San Diego: Pleural Publishing Inc pp: 355-360.
-
Rindi G, Klimstra DS, Arnold R, Carlo C, Klimstra DS, et al. (2010) Nomenclature and classification of neuroendocrine neoplasms of the digestive system. In: Bosman FT, et al. [Eds.] WHO classification of tumours of the digestive system. 4th (Edn), Lyon: IARC Press pp: 13-14.
-
Faisal M, Haider I, Waqas O, Taqi M, Hussain SR, Jamshed A (2016) Large Cell Neuroendocrine Carcinoma of Parotid Gland: A Diagnostic Dilemma among High Grade Carcinomas of Parotid Gland-Case Report and Review of Literature. J Rare Dis Diagn Ther 2(3): 45.
-
Kao HL, Chang WC, LI WY, Chia-Heng Li A, Fen-Yau Li A (2012) Head and neck large cell neuroendocrine carcinoma should be seperated from atypical carcinoid on the basis of different clinical features, overall survival, and pathogenesis. Am J Surg Pathol 36(2): 185-192.
-
Kawaratani H, Tsujimoto T, Yoshikawa M, Kawanami F, Shirai Y, et al. (2013) Large cell neuroendocrine carcinoma presenting with neck swelling in the submandibular gland: a case report. J Med Case Rep 7: 81.
-
Eveson JW, Thompson LDR (2013) Malignant Neoplasms of the Salivary Glands. In: Thompson LD Head and Neck Pathology. 2nd edn. Philadelphia: Elsevier pp: 332-333.
-
Ferlito A, Devaney KO, Rinaldo A (2006) Neuroendocrine neoplasms of the larynx: advances in identification, understanding and management. Oral Oncol 42(8): 770-778.
-
Kerr EH, Hameed O, Lewis JS, Bartolucci AA, Wang D, et al. (2012) Head and neck mucosal malignant melanoma: clinicopathologic correlation with contemporary review of prognostic indicators. Int J Surg Pathol 20(1): 37-46.
-
Olga Martinez-Saez, Javier Molina-Cerillo, Carmen Moreno García del Real, Rafael Barberá Durban, Juan J Díez, et al. (2016) Primary Neuroendocrine Tumor of the Parotid Gland: A Case Report and a Comprehenssive Review of a Rare Entity. Case Rep Otolaryngol 6971491.
-
Meacham R, Matrka L, Ozer E, Ozer HG, Wakely P, et al. (2012) Neuroendocrine carcinomas of the head and neck: a 20-year case series. Ear, Nose and Throat Journal 91(3): 20-24.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?