Incidence of Sleep Disordered Breathing in Children with Adenotonsillar Diseases
Study objectives: Assess the prevalence of sleep disordered breathing in adenotosillar diseases and identify the risk factors of sleep disordered breathing in children. Design: A retrospective random sample who had adenotonsillar diseases , were assessed with validated questionnaire which helped in understanding the impact of sleep disordered breathing which included history of physical suffering, sleep disturbances speech or swallowing problems, emotional distress, activity limitations, caregiver concerns, previous complaints, family history, orofacial or chest anomalies. Setting: The study includes 50 patients (children below 12 years of age) who reported to the E.N.T outdoor unit carried out for 3 months. The questionnaire was parental for below 10 years of agers. Intervention: None Conclusion: The Scores derived from parental questionnaire of child's sleep disturbances, physical suffering, emotional distress, orofacial anomalies are a predictor of incidence of sleep disordered breathing in children below 12 years of age. The implication obtained from the research is to improve quality of life of children suffering from SDB, the incidence of which is increasing day by day in today's life and are left undiagnosed or ignored by physicians or parents. However, the study should be further improvised for physical examination, evaluation of sleep cycle, endoscopic examinations and polysomnographic studies for confirmation of results obtained in the study performed here.
Introduction
Sleep-disordered breathing (SDB) is a general term for breathing difficulties occurring during sleep. SDB can range from frequent loud snoring to Obstructive Sleep Apnea (OSA) a condition involving repeated episodes of partial or complete blockage of the airway during sleep. When a child’s breathing is disrupted during sleep, the body perceives this as a choking phenomenon. The heart rate slows, blood pressure rises, the brain is aroused, and sleep is disrupted. Oxygen levels in the blood can also drop [1]. Sleep disordered breathing (SDB) is increasingly being recognized as a cause of morbidity even in young children. With an estimated prevalence of 1 to 4 per cent, SDB results from having a structurally narrow airway combined with reduced neuromuscular tone and increased airway collapsibility. SDB in children differs from adults in a number of ways, including presenting symptoms and treatment. Presentation may differ according to the age of the child. Children have a more varied presentation from snoring and frequent arousals to enuresis to hyperactivity [2]. Sleep apnoea in infants was first described in 1975 in relation to sudden infant death syndrome. During sleep, the ventilatory drive and upper airway muscle tone decrease. The inspiratory force collapses the pharyngeal airway that is already narrowed from other anatomic causes. The collapse of the pharyngeal airway leads to partial airway obstruction producing hypopnea, or total airway obstruction resulting in apnea [3].
Sleep disordered breathing can lead to following problems
Social: Loud snoring can become a significant social problem if a child shares a room with siblings or at sleepovers and summer camp. Behaviour and learning: Children with SDB may become moody, inattentive, and disruptive both at home and at school. Sleep disordered breathing can also be a contributing factor to attention deficit disorders in some children. Enuresis: SDB can cause increased night time urine production, which may lead to bedwetting. Growth: Children with SDB may not produce enough growth hormone, resulting in abnormally slow growth and development. Obesity: SBD may cause the body to have increased resistance to insulin or daytime fatigue with decreases in physical activity. These factors can contribute to obesity. Cardiovascular: OSA can be associated with an increased risk of high blood pressure or other heart and lung problems [1]. The most common form of pharyngeal narrowing in children is caused by hypertrophy of the adenoids and tonsils and is associated with the fact that the facial bones grow more slowly than the lymphoid tissue during childhood [4]. Adenotonsillar disease (adenoiditis and recurrent tonsillitis) is a prevalent otolaryngologic disorder aetiologically based on chronic inflammation. It is seen in extremes of society; i.e; lower as well as higher economic strata children. In lower strata it is seen due to bacterial infection whereas in higher strata it occurs due to over protection leading to adenotonsillar hypertrophy. Its peak incidence is at around 5-6 years of age. The questionnaire pattern helps to analyse the relation between adenotonsillar diseases and sleep disordered breathing, also it determines the role of sleep disordered breathing leading to orofacial and chest anomalies. By proper diagnosis and prevention of the disease and orofacial anomalies can be prevented and also improve the quality of life of children.
Epidemiology
In 2008, a cohort cross sectional study was done by the Brazilian Journal of Otorhinolaryngology on quality of life in children with sleep disordered breathing. The sample was selected consecutively at the mouth breathing ward of an ENT care reference center between August of 2008 and March of 2009. Caregivers were asked to answer standard questionnaire on sleep disorders prior to polysomnography testing. The subjects' quality of life was assessed based on the answers given by the children's caregivers to questionnaire OSA-18 adapted to Brazilian Portuguese by Silva et al. through the technique of back-translation, to attain exact compliance with the terms used in the original document. One hundred and ten children were examined between August of 2008 and March of 2009. The quality of life of children with sleep-disordered breathing is compromised. The most affected domains on questionnaire OSA-18 were "concern of persons in charge", "sleep disturbance", and "physical suffering", the last item being rated more highly by subjects with apnea than primary snorers. It was with this purpose that a specific survey to assess impact on quality of life - the OSA-18 questionnaire - was answered by the children's caregivers to compare OSAS (apnea) and PS (no apnea) groups. Untreated pediatric SDB may lead to adverse present and future consequences to the affected individuals, their families, and society. Unfortunately, many individuals still remain undiagnosed and untreated [4]. Another research, in 2002, by Department of Pediatrics, Divisions of Clinical Epidemiology and Behavioral Pediatrics and Psychology, Rainbow Babies & Children’s Hospital, Case Western Reserve University School of Medicine, Cleveland, on sleep disordered breathing in which, trained research assistants studied families at home or other convenient locations. Demographic and medical data were assessed with the Children’s Sleep and Health Questionnaire (CSHQ), a pediatric modification of a validated questionnaire (Health and Sleep Questionnaire, HSSQ
Their data suggest that SDB is associated with reduced HRQOL (health related quality of life) in domains related to physical health outcomes, specifically for overall physical health status and for reports of bodily pain [5]. Another in 2004, by University of Thessaly School of Medicine and Larissa University Hospital, Larissa, Greece where children and adolescents (3,680 in all, 1-18 years old) attending schools in central Greece were surveyed by questionnaires distributed to parents. The estimated frequency of obstructive sleep apnea-hypopnea among children without adenoidectomy and/or tonsillectomy was 4.3% in the study. In conclusion, snoring every night was equally prevalent in younger and older ages, more frequent in males, and present even in some children with a history of adenoidectomy and/or tonsillectomy. Chronic rhinitis, family history of snoring, and exposure to cigarette smoke were associated with an increased frequency of habitual snoring [6]. Kosair Children's Hospital Research Institute, and Division of Pediatric Sleep Medicine, Department of Pediatrics, University of Louisville, Louisville, KY 40202, USA in 2004 also did a retrospective study research to assess the predictive validity of parental report of snoring and other behaviours. One hundred twenty-two pre- schoolers and 172 5- to 7-year-olds, and their parents, participated in both subjective-report and objective- recording portions of the study. Scores derived from parental-report questionnaires of children's snoring and other sleep and wake behaviours can be used as surrogate predictors of snoring or sleep-disordered breathing in children [7]. Department of Medicine, Boston University School of Medicine, Boston, in 2003, performed a parent- completed questionnaire was used to ascertain the presence and intensity of snoring and other SDB symptoms and the presence of daytime sleepiness and problem behaviors. SDB symptoms were present in 744 (25%) children.SDB symptoms are common in 5-year-old children and are associated with an increased risk of daytime sleepiness and with problem behaviors suggestive of attention-deficit/hyperactivity disorder [8]. In 2010,Department of Dentistry and Surgery, University of Bari, Italy objective was to investigate the occurrence of sleep-related breathing disturbances in a large cohort of school-aged children in Southern Italy. A screening phase aimed to identify symptomatic children and clinical data from a cohort of 495 children by a self-administered questionnaire. A total of 436 questionnaires (response rate: 88.08%) were returned and scored (202 M, 234 F; Mean age ± Standard deviation: 6.2 ± 1.8); 18 children (4%) were identified as habitual snorers, 140 children (32%) were identified as occasional snorers, and 278 children (64%) were identified as non-snorers [9]. Department of Otolaryngology, State University of New York Downstate Medical Center and The Long Island College Hospital, USA, in 2003, conducted a cohort study in 69 children (age range, 6 months to 13 years; median age, 6.1 years) from a hospital-based pediatric otolaryngology practice in a metropolitan area by using OSA-18 and the most responsive domains were sleep disturbance, physical suffering, and caregiver concerns [10]. In 2013, Melbourne School of Psychological Sciences, The University of Melbourne, Melbourne, Australia prepared a clinical sample of preschool children (3-5 y) and SDB was diagnosed. Parents completed health-related QOL and parenting stress questionnaires. Their findings demonstrate that sleep disordered breathing is associated with reduced quality of life in preschool children and their families. These results support previous quality of life findings in older children and in samples with broader age ranges [11]. Likewise many other studies have also proved that the quality of life was estimated by questionnaires and thus leading to diagnosis and prompt management leading to improved quality of life.
Aims and Objectives
The main aim of the study is to find the relation between sleep disordered breathing in children with adenotonsillar disease. There are 2 objectives of the study namely- a) Objective 1: To study the incidence of SDB in children with adenotonsillar disease. b) Objective 2: To determine the role of SDB in children leading to orofacial and chest anomalies.
Materials and Methods
The study was retrospective type only for samples who had adenotonsillar diseases , and was carried with validated questionnaire which helped in understanding the impact of sleep disordered breathing which included history of physical suffering, sleep disturbances speech or swallowing problems, emotional distress, activity limitations, caregiver concerns, previous complaints, family history, orofacial or chest anomalies. The study includes 50 patients (children below 12 years of age) who reported to the E.N.T outdoor unit carried out for 3 months. The questionnaire was parental for below 10 years of agers.
Exclusion and Inclusion Criteria
The choice for the study was for children only below 12 years of age with or without recurrent attacks of tonsillitis. Any disease struck patients (asthma, neurological disorders, cardiomyopathies, pulmonary disorders etc.) were not analysed so as to keep the study focused on SDB caused or exaggerated by adenotonsillar diseases only.
Consent Procedures
Informed consent was already put forward so that the informant or the patient understands the nature of the study. The study was well explained to the patient or the volunteer and makes him/her understand their involvement.
Results
After the completion of the questionnaire for 50 patients, scoring was done on the basis of the problems faced by the patient (Tables 1 & 2), (Figures 1-6).
| Score | Problems Faced |
|---|---|
| 0 | LOW |
| 1 | MEDIUM |
| 2 | HIGH |
Table 1: Scoring system based on the symptoms.
| Physical Suffering | Sleep Disturbances | Speech Problems | Emotional Distress | Activity Limitations | Orofacial Abnormalities | Sum | |
|---|---|---|---|---|---|---|---|
| 1 | 1 | 1 | 0 | 1 | 0 | N | 3 |
| 2 | 1 | 1 | 1 | 2 | 2 | Y | 7 |
| 3 | 1 | 2 | 2 | 2 | 2 | N | 9 |
| 4 | 2 | 2 | 2 | 2 | 2 | Y | 10 |
| 5 | 2 | 2 | 1 | 2 | 1 | N | 8 |
| 6 | 1 | 1 | 1 | 1 | 1 | N | 5 |
| 7 | 1 | 0 | 1 | 2 | 2 | N | 6 |
| 8 | 1 | 1 | 1 | 1 | 1 | N | 5 |
| 9 | 1 | 1 | 2 | 2 | 1 | N | 7 |
| 10 | 1 | 1 | 1 | 2 | 1 | N | 6 |
| 11 | 0 | 1 | 1 | 1 | 1 | N | 4 |
| 12 | 1 | 1 | 1 | 1 | 1 | N | 5 |
| 13 | 1 | 1 | 1 | 0 | 0 | N | 3 |
| 14 | 1 | 1 | 1 | 1 | 1 | N | 5 |
| 15 | 1 | 1 | 1 | 2 | 2 | Y | 7 |
| 16 | 1 | 1 | 1 | 1 | 1 | N | 5 |
| 17 | 1 | 1 | 1 | 1 | 1 | N | 5 |
| 18 | 1 | 1 | 1 | 1 | 1 | N | 5 |
| 19 | 2 | 2 | 1 | 2 | 2 | N | 9 |
| 20 | 1 | 2 | 2 | 2 | 2 | Y | 9 |
| 21 | 1 | 2 | 1 | 2 | 1 | Y | 7 |
| 22 | 1 | 1 | 0 | 0 | 1 | N | 3 |
| 23 | 1 | 0 | 1 | 2 | 1 | Y | 5 |
| 24 | 2 | 2 | 2 | 2 | 2 | Y | 10 |
| 25 | 2 | 0 | 1 | 1 | 1 | N | 5 |
| 26 | 2 | 2 | 2 | 2 | 1 | Y | 9 |
| 27 | 2 | 2 | 2 | 2 | 2 | Y | 10 |
| 28 | 1 | 1 | 1 | 1 | 1 | N | 5 |
| 29 | 2 | 2 | 0 | 0 | 1 | N | 5 |
| 30 | 1 | 1 | 1 | 0 | 1 | N | 4 |
| 31 | 1 | 1 | 1 | 2 | 0 | N | 5 |
| 32 | 1 | 1 | 1 | 0 | 1 | N | 4 |
| 33 | 0 | 1 | 1 | 1 | 1 | N | 4 |
| 34 | 2 | 1 | 1 | 0 | 1 | N | 5 |
|---|---|---|---|---|---|---|---|
| 35 | 1 | 1 | 1 | 2 | 2 | Y | 7 |
| 36 | 2 | 2 | 2 | 1 | 1 | Y | 8 |
| 37 | 0 | 0 | 2 | 2 | 0 | N | 4 |
| 38 | 1 | 1 | 1 | 1 | 1 | N | 5 |
| 39 | 1 | 1 | 1 | 2 | 1 | Y | 6 |
| 40 | 0 | 1 | 1 | 0 | 0 | N | 2 |
| 41 | 1 | 2 | 2 | 1 | 1 | Y | 7 |
| 42 | 1 | 1 | 1 | 2 | 1 | N | 6 |
| 43 | 1 | 1 | 1 | 0 | 1 | N | 4 |
| 44 | 1 | 1 | 0 | 2 | 0 | N | 4 |
| 45 | 1 | 0 | 2 | 1 | 0 | N | 4 |
| 46 | 1 | 1 | 1 | 2 | 1 | Y | 6 |
| 47 | 1 | 1 | 2 | 1 | 1 | Y | 6 |
| 48 | 1 | 2 | 1 | 1 | 0 | N | 5 |
| 49 | 1 | 0 | 1 | 1 | 1 | N | 4 |
| 50 | 1 | 1 | 2 | 2 | 0 | N | 6 |
Table 3: Compilation of the results based on the scores (OUT OF 50 PATIENTS).
$$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$
$$ = \frac {1}{2} $$ $$ = \frac {1}{2} $$
$$ = \frac {1}{2} $$ Figure 3: Pie chart showing incidence of emotional distress.

If all the parameters are of moderate risk- score 5 If all the parameters are of high risk- score 10 Thus, we conclude that – Between score 0- score 5: child less likely to have sleep disordered breathing Between score 6- score 10: child more likely to have sleep disordered breathing.
In our data
a) 28 children have score between 0-5; i.e, they are less likely to have sleep disordered breathing. b) 22 children have score between 6- 10; i.e, they are Figure 5: Chart showing patients in whom incidence of sleep disordered breathing found to be high and low in our study.
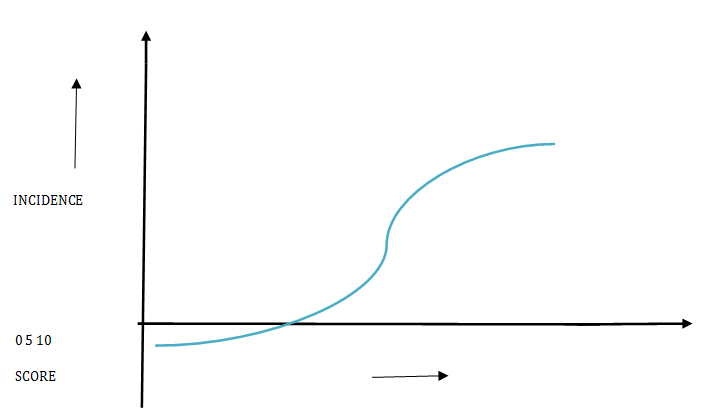
Figure 6: Graph showing the incidence of sleep disordered breathing in patients taken for the study. In the pie chart of orofacial anomalies, we see that, 16 children have had orofacial or chest anomalies while the rest 36 did not have anomalies. And if we see in the Table 1 the children who have orofacial or chest anomalies are high risk scorers (score between 6-10) or under the children who are most likely to have SDB, thus supporting the objective 2 of the research; i.e, role of SDB in orofacial anomalies.
Discussion
Our data suggests that SDB is associated with high risk of physical suffering, emotional stress and sleep disturbances mainly. The incidence of SDB increased with severity of the parameters. The possible explanations of the result coming out this way can be- 1) increased discomfort related to increased work of breathing or mouth breathing related to upper airway obstruction 2) morning headache pain following impaired gas exchange associated with SDB or 3) dysphagia related to enlarged tonsils often associated with childhood SDB. Alternatively, children with SDB and poor quality sleep may be more fatigued or irritable compared to children without SDB. This fatigue or heightened irritability may trigger more general somatization of symptoms [5]. Our findings of incidence of SDB more in children with high complaints of physical suffering, sleep disturbances, emotional stress and role of SDB in orofacial anomalies are consistent with other researches [12]. Just by parental questionnaire one can judge the children for symptoms relative for SDB which can lead to prompt care and management of the disease and better quality of life for children. The possible limitation of our study can be the relative mild degree of SDB in low risk scorers which would have been neglected during the course of study as the study just comprises of questionnaire and no other investigations performed (polysomnography, physical examination, endoscopic examinations).
Scores derived from parental questionnaire of child’s sleep disturbances, physical suffering, emotional distress, orofacial anomalies are a predictor of incidence of sleep disordered breathing in children below 12 years of age. The significance of the finding obtained from the research is to improve quality of life of children suffering from SDB, the incidence of which is increasing day by day in today’s life and are left undiagnosed or ignored by physicians or parents. However, the study should be carried forward for physical examination, evaluation of sleep cycle, endoscopic examinations and polysomnographic studies for confirmation of results obtained in the study performed here.
Summary
The purpose of the study was to describe the prevalence of sleep disordered breathing in children with adenotonsillar disease and also the role of SDB leading to orofacial and chest anomalies like adenoid facies or cardiovascular sequele. 50 children of age below 12 years were studied by a parental questionnaire for those reporting to the ENT ward. Several parents complained of their children’s snoring, fatigue, activity limitations, lack of sleep problems. The set questionnaire was scored on the basis of complaints (graded from high to low), which was then evaluated. The results of which then compiled as- a) 28 children who have total score between 0-5 were less likely to have sleep disordered breathing. b) 22 children who have total score between 6-10 were more likely to have sleep disordered breathing due to high complaints of sleep disturbances and physical suffering out of those 22, 16 had orofacial anomalies.
References
-
(2016) American Academy of Otolaryngology–Head and Neck Surgery. Pediatric sleep disordered breathing in children.
-
Deepti S, Christian G (2010) Sleep disordered breathing in children. Indian J Med Res pp. 311-320.
-
Hsueh-Yu Li, Li-Ang Lee (2016) Sleep-disordered breathing in children 32(3): 247-257.
-
Amaury de MG, Otávio M dos S, Kleber P, Pablo PM, Leonardo MG, et al. Quality of life in children with sleep-disordered breathing. Braz J Otorhinolaryngol 78(5).
-
Carol L Rosen, Tonya MP, Emma KL, Susan R (2016) Health-related Quality of Life and Sleep-disordered Breathing in Children. 25(6): 648-658.
-
Kaditis AG, Finder J, Alexopoulos EI, Starantzis K, Tanou K, et al. (2004) Sleep-disordered breathing in 3,680 Greek children. Pediatr Pulmonol 37(6): 499- 509.
-
Montgomery-Downs HE, O'Brien LM, Holbrook CR, Gozal D (2004) Snoring and sleep-disordered breathing in young children: subjective and objective correlates. Sleep 27(1): 87-94.
-
Gottlieb DJ, Vezina RM, Chase C, Lesko SM, Heeren TC, et al. (2003) Symptoms of sleep-disordered breathing in 5-year-old children are associated with sleepiness and problem behaviors. Pediatrics 112(4): 870-877.
-
Cazzolla AP, Lacarbonara V, Pellegrino B, Testa NF, Fidanza F, et al. (2010) Sleep-disordered breathing in a sample of 495 children in Southern Italy**.** Eur J Pediatr Dent 11(4): 189-192.
-
Sohn H, Rosenfeld RM (2003) Evaluation of sleep- disordered breathing in children. Otolaryngol Head Neck Surg 128(3): 344-352.
-
Jackman AR, Biggs SN, Walter LM, Embuldeniya US, Davey MJ, et al. (2013) Sleep disordered breathing in early childhood: quality of life for children and families. Sleep 36(11): 1639-1646.
-
Moraleda-Cibrián M, Edwards SP, Kasten SJ, Berger M, Buchman SR, et al. (2014) Symptoms of sleep disordered breathing in children with craniofacial malformations. J Clin Sleep Med 10(3): 307-312.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?