Endoscopic Management of Middle Ear Atelectasis
Objective: To determine the contribution of otoendoscopy in the surgical management of atelectatic ear to improve clinical and audiological results. Methods and Materials: Thirty eight ears in 24 patients with middle ear atelectasis and intact ossicular chain were randomly assigned into 2 groups: Group I included 27 ears who were underwent endoscopic T- tube insertion and Group II included 11ears who were underwent endoscopic cartilage tympanoplasty. Assessment of hearing was performed for all cases preoperatively, 3 months postoperatively. Statistical analysis used: The analysis of the data was carried out using the IBM SPSS 20.0 statistical package software. Data were expressed as mean and standard deviation for quantitative measures in addition to both number and percentage for categorized data. Chi-square test or Fisher’s exact test were used to compare categorical variables. A P-value less than 0.05 was considered to be statistically significant. Results: There is significant postoperative improvement of ABG averages reported in the two studied groups with mean hearing gain of 21.67±7.97dB in group I and 19.72±5.3 dB in group II. Conclusion: At three months, there was significant statistical difference concerning different audiological parameters among the two groups.
Introduction
Middle ear atelectasis occurs as a sequela of chronic inadequate middle ear ventilation [1]. Hearing levels are a poor indicator for the severity of the disease [2]. Sadé proposed the first classification system that graded retractions. In 1982, Tos described a classification system solely devoted to Shrapnell’s membrane [3]. Sadé classification of atelectatic ear [3]. Stage I: Slight retraction of tympanic membrane Stage II: Retraction of tympanic membrane, touching the incus or the stapes stage III: Tympanic membrane touching the promontory stage IV: Tympanic membrane adherent to the promontory The ideal treatment strategy for management of is controversy [4]. Compared to the microscope, endoscopic ear surgery is minimally invasive, has less morbidities, results in better hearing outcomes with greater preservation of normal anatomy [5]. The aim of this study was to explore the feasibility and effectiveness of endoscopic management in atelectatic ear.
Materials and Methods
This study was carried on 24 patients with middle ear atelectasis, diagnosed clinically, endoscopically, and audiologically among patients selected from the ENT Outpatient Clinic of Al-Azhar University Hospital (Assiut). Approval of the ethical committee was obtained with patient consents collected before the start of the study. In total, 27 ears were subjected to ventilation tube insertion (T-tube) (group I), whereas the other 11 ears underwent tragal cartilage tympanoplasty (group II). Follow-up visits were scheduled after 1 week, 2 weeks, 1 and 3months. A postoperative audiogram was obtained 3 months later, and the ears were examined endoscopically. The differences between the preoperative and postoperative air bone gaps (ABGs) were also calculated.
Results
The study included 38 affected ears in 24 patients. Demographic data of both study group patients are summarized in (Table 1).
| Basic characteristic | Cartilage group | T-Tube group | All cases | ||
|---|---|---|---|---|---|
| Ear number | 11 | 27 | 38 | ||
| Age (years) | Range | 22-50 | Oct-50 | Oct-50 | |
| Age (years) | Mean±SD | 34.3±10.3 | 16.2±8.6 | 21.3±11.7 | |
| Sex | Male | 4 (36.4%) | 18 (66.7%) | 22 (64.7%) | |
| Sex | Female | 7 (63.6%) | 9 (33.3%) | 16 (35.3%) |
Table 1: Number of ears with mean air bone gap preoperative and postoperative.
Table1: Age and sex of the study groups.
Clinical Results
Group I, at 3 months, tubes were in place in 23 (85%) ears. There were extrusion in four (15%) ears and two (7.5%) of them had residual perforation. The ears that had residual perforations were diagnosed preoperatively as third-stage atelectasis (Table 2). Group II, Grafts were taken in 10 (91%) ears and were broken with residual perforation in one (9%) ear.
| Complications | At three months | |
|---|---|---|
| No. of ears | Percentage | |
| Tubal extrusion | 4 | 15% |
| Residual perforation | 2 | 7.50% |
| Recurrent retraction | 0 | 0% |
| Tubal blockage | 1 | 3.70% |
| Otorrhea | 3 | 11% |
| Tympanosclerosis | 0 | 0% |
Table 2: Number of ears with mean air bone gap preoperative and postoperative.
Table2: Complications of tube insertion and their percentage.
Audiological Results
Tables 3-5 and Figure 1 show a comparison between the mean hearing gain and mean ABG for the two groups.
| Time | Cartilage group | Tube group | Chi square | P value | |
|---|---|---|---|---|---|
| Preoperative | 0-10 dB | 0 (0.0%) | 0 (0.0%) | 0.133 | 0.248(NS) |
| Preoperative | 10-20 dB | 1 (9.1%) | 7 (25.9%) | 0.133 | 0.248(NS) |
| Preoperative | >20 dB | 10 (90.9%) | 20 (74.1%) | 0.133 | 0.248(NS) |
| At 3 months postoperative | 0-10 dB | 4 (36.4%) | 22 (81.5) | 0.104 | 0.008(S) |
| At 3 months postoperative | 10-20 dB | 6 (54.5%) | 3 (11.1%) | 0.104 | 0.008(S) |
| At 3 months postoperative | >20 dB | 1 (9.1%) | 2 (7.4%) | 0.104 | 0.008(S) |
Table 3: Number of ears with mean air bone gap preoperative and postoperative.
| Preoperative | 3 months post-operative | |
|---|---|---|
| Mean±SD | Mean±SD | |
| Hearing gain | - | 21.67±7.97 |
| Air bone gap | 25.25±5.19 | 3.59±6.28 |
Table 4: Mean hearing gain and air bone gap for group I.
| Preoperative | 3 months post-operative | |
|---|---|---|
| Mean±SD | Mean±SD | |
| Hearing gain | - | 19.72±5.3 |
| Air bone gap | 27.09±2.74 | 7.36±6.67 |
Table 5: Mean hearing gain and air bone gap for group II.
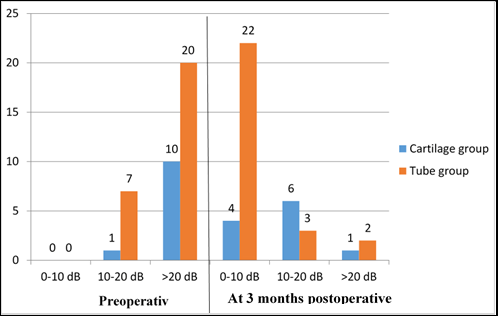
Figure1: Number of ears with mean air bone gap preoperatively and postoperatively in both group.
Discussion
As regards clinical results at 3 months postoperatively, the first group showed a marked improvement. Despite the presence of postoperative otorrhea in three (11%) ears. This incidence of infection was superior to that of Bluestone [6] who recorded 30% of ears with postoperative otorrhea after using classic Goode T-tube. There was extrusion in four (15%) ears two of them had residual perforation (7.5%). The ears that had residual perforation were third-stage atelectasis preoperatively. As we mentioned above, there was extrusion of tube in four (15%) ears. This was in agreement with the findings of Sederberg-Olsen, et al. [7] who found 18% extrusion after insertion using Goode T-tubes.
Using the classic operative technique of Goode T-tube insertion, Leopold and McCatx [8] reported that extrusion occurred earlier in the thin TM. There were two (7.5 %) ears with persistent perforation. These results were superior to that of Courteney-Harris and colleges who reported 15% residual perforation after insertion of T-tubes [9] .Tubal blockage was present in one (3.7%) ear, which was in agreement with the results obtained by Isaacson [10] who reported 7% tubal occlusion as a complication of tube insertion.
As regards audiological results at 3 months postoperatively, the mean hearing gain for the first group was 21.67±7.97 dB at 3 months postoperatively. The mean ABG was 25.25±5.19 dB preoperatively, 3.59±6.28 dB at 3 months postoperatively. These audiological results were in agreement with that of Goode [11] who used the Goode T-tube for long-term ventilation of the middle ear by classic technique. He reported 87% of the patients with normal hearing threshold 1 year postoperatively [11]. Bluestone and colleagues reported almost similar results after use of long- term ventilation tube in the treatment of recurrent effusion and atelectatic ear [7, 12].
For the second group, as regards clinical results, tragal cartilage grafts were taken in 10 (91%) ears, whereas break with residual perforation occurred in one (9%) case. This result was nearly in agreement with that of Dornhoffer [12] who, in his 1000 case series, reported that an atelectatic TM was the surgical indication in 15%, of which 20% were revision cases and two-thirds were in children. The success rate was more than 95% for graft take [12]. As regards audiological results at 3 months postoperatively, the mean air bone gap was 27.09±2.74 dB preoperatively, 7.36±6.67 dB at three months postoperatively. This result also was nearly in agreement with that of Elsheikh, et al. [13] who operated 23 cases and reported that in the atelectatic ear, cartilage allowed reconstruction of the TM with good anatomical and functional results with recurrent disease in three cases.
Recommendations
The obvious limitations of study are relative short follow up. As tympanic membrane retractions and reperforations have been reported even years later, a longer follow up with a larger sample size is recommended.
References
-
Satar B, Hidir Y, Coskun U (2010) New morphometric findings in adhesive otitis media: Petroclival angle and eustachian tube-tympanic cavity ventilation angle. Auris Nasus Larynx 37(1): 61-65.
-
Sadé J (1980) Retraction pockets and attic cholesteatomas. Acta Otorhinolaryngol Belg 34(1): 62-84.
-
Emmett SD, Kokesh J, Kaylie D (2018) Chronic Ear Disease. Med Clin North Am 102(6): 1063-1079.
-
Djalilian HR, Paparella MM (2000) The atelectatic ear. Current opinion in otolaryngology & head and neck surgery 8(5): 369-374.
-
Kozin ED, Gulati S, Kaplan AB, Lehmann AE, Remenschneider AK, et al. (2015) Systematic review of outcomes following observational and operative endoscopic middle ear surgery. Laryngoscope 125(5): 1205-1214.
-
Bluestone CD (2002) Tympanostomy tubes and related procedures. Atlas Ped Operative Otolaryngol 1: 4-18.
-
Sederberg Olsen JF, Sederberg Olsen AE, Jensen AM (1994) Late sequelae related to treatment with ventilation tubes for secretory otitis media in ENT practice. In: Mogi G, et al. (Eds.), Recent advances in otitis media, Amsterdam Kugler Publications, pp: 843.
-
Leopold DA, McCatx BF (1980) Factors influencing tympanostomy tube function and extrusion: a study of 1127 ears. Otolaryngol Head Neck Surg 88(4): 447-454.
-
Courteney RG (1992) Closure of tympanic membrane perforation after the removal of Goode-type tympanostomy tubes: the use of silastic sheeting. J Laryngol Otol 106(11): 960-962.
-
Isaacson GC (2015) Overview of tympanostomy tube placement, postoperative care, and complications in children.
-
Goode RL (1996) Long-term middle-ear ventilation with T-tubes: the perforation problem. Otolaryngol Head Neck Surg 115(6): 500-501.
-
Dornhoffer J (2003) Cartilage tympanoplasty: indications, techniques, and outcomes in a 1,000-patient series. Laryngoscope 113(11): 1844-1856.
-
Elsheikh MN, Elsherief HS, Elsherief SG (2006) Cartilage tympanoplasty for management of tympanic membrane atelectasis: is ventilatory tube necessary? Otol Neurotol 27(6): 859-864.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?