Unusual Development of Second Branchial Cleft Cyst in an Adult after URTI: Diagnosis and Detailed Approach
Branchial cleft cyst is a congenital anomaly benign in nature. It usually appears in the lateral aspect of the neck and typically presents as a unilateral fluctuant mass. We present here a 30 years old adult who is previously healthy complaining of five years history of a left lateral neck swelling following an upper respiratory tract infection. Multiple aspirations were done but all resulted in recurrence of condition. Investigations have been done and a CT neck performed which showed a complicated second branchial cleft cyst. The definite treatment for branchial cleft cysts is surgery. He underwent surgical excision of the cyst with minimal scarring. This case is important due to the limited literature done in adults with branchial cleft cysts, in addition to highlighting the correct sequence of management when detecting a lateral cervical swelling.
Introduction
The most frequent clinical presentation in patients with branchial cysts consists of a left-sided, painless, cervical mass [1]. It has four types, type two being the most common type. Second branchial cleft cysts are usually detected in the lateral cervical space anterior to the sternocleidomastoid muscle. There is no gender difference in prevalence [2]. It can present clinically as: cysts, sinuses, and fistulae [3]. A cyst is formed when a branchial groove remnant forms an epithelial-lined space without communication to the skin or mucosa [4]. Preoperative differential diagnoses include thyroglossal duct cyst, cervical lymphadenitis, cervical abscess, toxoplasmosis, tuberculosis, dermoid, dermal inclusion cyst, hydatid cyst, lymphangioma, and malignant neoplasm [5, 6]. However, branchial cleft cysts are uncommon in adults, in addition to that, recent literature regarding branchial cysts is scanty in this age group. For this reason, we are discussing this case starting from when the patient presented to us at the tertiary care public hospital of otorhinolaryngology to after surgical excision of the cyst including the post-operative condition.
Our patient is a 30 year old male who is previously healthy presented to us with a left lateral neck swelling of 5 years duration started when he was 25 years old. It first appeared after the patient had a severe upper respiratory tract infection. The neck swelling increased in size gradually over time. In general, it was painless. However, he had an episode of tenderness and pain seven months ago associated with fever that was relieved by antibiotics. Being treated with antibiotics helped with pain but not the size of the swelling. The patient was aspirated several times before he came to us which resulted in recurrent of the same condition. Overall, he has no other complaints except for the swelling. There was no airway compromise or change of voice. He’s not on any medications regularly, has no allergies, and with no past surgical history. Our patient is a nonsmoker and a nonalcohol consumer.
On examination, the swelling was on the left side of the neck in the submandibular area, large in size around 8x8 cm, round, smooth, fluctuant, and nontender. There was no skin discoloration in relation to the lesion or other masses palpated including lymph nodes. Rest of head and neck examination was unremarkable. Our patient was also afebrile. The fine needle aspiration (FNAC) that was done 7 months ago during the episode of tenderness gave a turbid white fluid aspirate. Smears showed mainly acute inflammatory cells, necrotic debris, viable and degenerated squamous epithelial cells. Special smears for AFB was negative. However, latest fine needle aspiration smear (FNAC) showed dispersed viable and degenerated squamous epithelial cells, few mononuclear inflammatory cells with proteinaceous material in the background. Fluid aspirate was brownish in color with no turbidity. Ultrasound image showed a large cystic swelling measuring 6x8 cm. MRI and CT with and without contrast were done.
Latest CT (4th of April 2021) compared to previous CT study dated 6-12-2016 revealed progressive course of well-defined ablong shaped cystic lesion seen at the left side of the neck related to the left mandibular angle, seen just anteromedial to the sternocleidomstoid muscle and displacing it posteriorly, currently is measuring about 5.3x3.8x6.6 cm in maximum AP, TR, and CC dimensions. It is seen posterior to the left submandibular gland and lateral to the carotid sheath vessels displacing it medially. It also shows mild diffuse mural thickening with few mildly enhancing septae seen mainly in its lower portion. It is associated with mild stranding of the surrounding fat planes along with few subcentemetric loco-regional lymph nodes. Findings are suggestive of complicated left second branchial cleft cyst. After confirming the diagnosis, the plan was to schedule him for surgical resection, which is the gold standard management of branchial cleft cysts. Knowing proper anatomy of the neck including the nerves, vessels, and muscles is essential for safe excision.
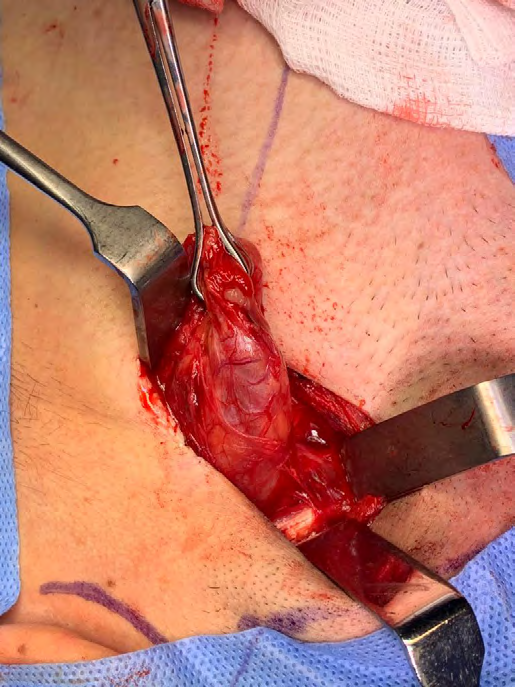
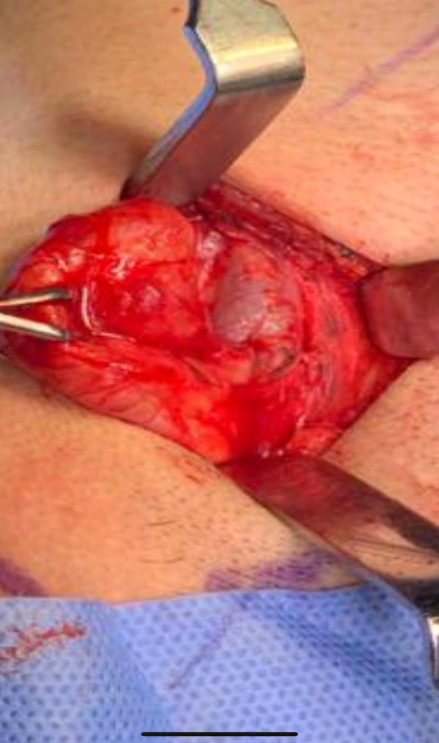
Our plan is to schedule our patient for surgical excision. He underwent the surgery, which showed a branchial cleft cyst that was pushing the glossopharyngeal and the hypoglossal nerve superio-medially and the internal jagular vein inferio-medially, extending to the accessory nerve inferiorly and ending in the pyriform fossa.There was no intraoperative complications and a wound on a skin fold that was closed subcuticular to minimize scarring. During his hospital stay he complained of minimal pain that was managed with regular painkillers (Figures 1-8).
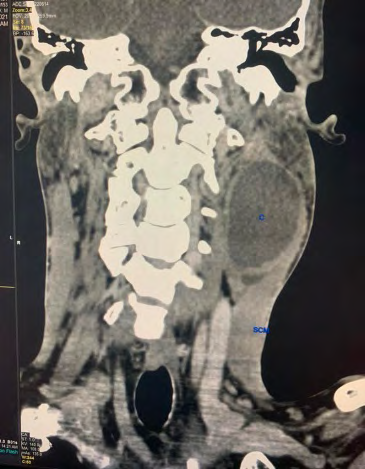
C: Branchial cleft cyst SCM: Sternocleidomastoid Figure 1: CT scan of neck coronal view.
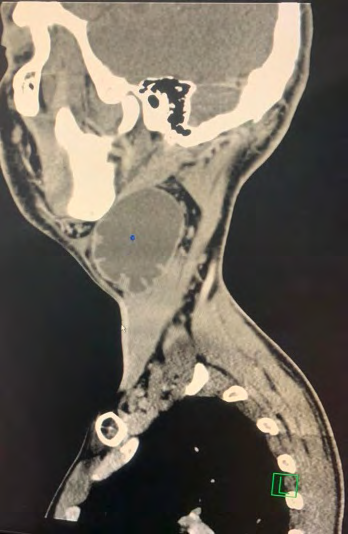
C: Branchial cleft cyst Figure 2: CT scan of neck sagittal view.
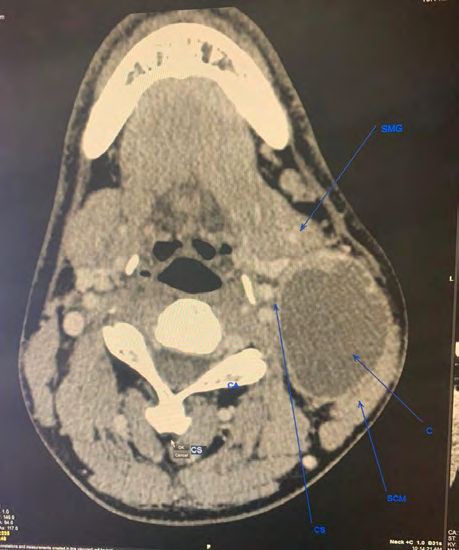
SCM: Sternocleidomastoid C: Branchial cleft cyst CS: Carotid sheath SMG: Submandibular gland Figure 3: CT scan of neck axial view.



Discussion
Branchial cleft cysts form early in gestation. Four branchial (pharyngeal) clefts form five ridges during the fourth week of embryonic development. These ridges consistute to the formation of parts of the head, neck, and thorax. In which they form the six branchial (pharyngeal) arches. The branchial arches form pouches internally and grooves or clefts externally. A pouch is lined by endoderm and associated with a ventral or dorsal wing. Ectoderm lines the branchial cleft derivatives, however, branchial arch derivatives are lined with mesoderm. Each arch is related to a cartilaginous bar, carotid artery derivative, cranial nerve, and vein. The nerves are located anterior to the artery of each arch it is associated with, except for the sixth arch in which the nerve runs posterior to the artery [7]. Incomplete involution of branchial cleft structures during embryonic development results in branchial cleft cysts, making it a congenital condition. It is common to first appear after an upper respiratory tract infection as the case in our patient.
There are 4 types of brancial cleft cysts classified according to the level:
First Branchial Cleft Cyst
First cleft cysts contribute to the formation of about 5-25% of all branchial cleft anomalies and are subclassified by the Work classification system. On physical examination, work type I shows preauricular masses or sinuses that track medial and anterior to the external auditory canal and contains ectoderm only. They classically appear lateral to the facial nerve and end within the external auditory canal, or attach to the umbo of the middle ear, as a duplication of the external auditory canal. Work type II cysts contain both ectoderm and mesoderm, and are more common. Classically they present in the submandibular area or at the angle of the mandible. They can appear either medial or lateral to the facial nerve and cross superficial to it in 57% of cases, 30% are deep, or between branches of the facial nerve in 13% of them [8].
Second Branchial Cleft Cyst
It forms approximately 40-95% of branchial anomalies making it the most common type. The external opening is found anterior and medial to the sternocleidomastoid (SCM) on the skin of the neck. Branchio-oto-renal syndrome is associated with bilateral second branchial cleft cysts. Its’ sinus has an external opening that is located on the neck skin as described above, with the fistula running deep to the platysma then passes in between the internal and external carotids, being superficial to both glossopharyngeal and hypoglossal nerves before attaching to the tonsillar fossa. Cysts or sinuses of this branchial cleft can appear anywhere along this tract [2, 9]. Second branchial cleft cysts have been classified into subtypes by Bailey back in 1929 [10]
- Type I: Most superficial and lies along the anterior surface of sternocleidomastoid deep to the platysma, but not in contact with the carotid sheath.
- Type II: Most common type where the branchial cleft cyst lies anterior to the sternocleidomastoid muscle, posterior to the submandibular gland, adjacent and lateral to the carotid sheath.
- Type III: Extends medially between the bifurcation of the internal and external carotid arteries, lateral to the pharyngeal wall.
- Type IV: Lies deep to the carotid sheath within the pharyngeal mucosal space and opens into the pharynx.
Intraoperatively our patient’s branchial cleft cyst was pushing the glossopharyngeal and the hypoglossal nerve superio-medially and the internal jagular vein inferio- medially, extending to the accessory nerve inferiorly and ending in the pyriform fossa.
Third Branchial Cleft Cyst
These cysts approximately form 2-8% of all branchial cleft anomalies. The external skin opening is located over the middle to lower third of the anterior SCM in the case of third branchial cleft cysts. Its’ sinus has a skin opening as described above then the tract runs deep to the platysma and course posterior to the internal carotid artery. It then passes between the glossopharyngeal (IX) and hypoglossal (XII) nerves, and can be closely associated with the superior laryngeal nerve, classically passing superior to it. After that it connects to the pyriform sinus in the larynx [11].
Fourth Branchial Cleft Cyst
These cysts represents around 1% of all branchial cleft anomalies, making them very rare and the rarest out of them all. It is more common to appear on the left, with the skin opening close to the medial lower border of the SCM. The exact path of the fourth branchial cleft remnant is not very well established due to its rarity, however, it typically runs deep to the common carotid and can curve around either the aortic arch in a left-sided anomaly or the subclavian in a right-sided anomaly. These pass superficial to the recurrent laryngeal nerve and hypoglossal nerve ending in the apex of the pyriform sinus in the larynx [11].
Ruling out other conditions that may present similarly is essential. Some of the differential diagnosis that should be kept in mind in such presentation include lymphadenopathy (reactive, neoplastic, lymphoma, metastasis), hemangioma, carotid body tumor, cystic hygroma, ectopic thyroid or salivary tissue, vascular neoplasm or malformation thyroglossal duct cysts, cat scratch disease, atypical mycobacterial infections, and cystic squamous cell carcinoma. Since our patient is an adult, it is beyond important to rule out cancer as early as possible. As it has been said time is money and a neck swelling in this age group is cancer until proven otherwise. Hence, proper investigations should be done starting from basic laboratory tests, ultrasound, fine needle aspiration is essential, and CT/MRI should be done. Open biopsy is indicated if there is high suspicion of malignancy and FNAC is negative.
Oropharyngeal HPV-associated squamous cell carcinoma (SCC) can metastasize to a cervical lymph node as a cystic squamous cell carcinoma. Literature suggests the importance of carefully ruling out this differential as the presentation and imaging can look almost identical to a branchial cleft cyst. Not considering HPV-associated SCC can lead to delayed diagnosis of disease hence delayed treatment. It is more common in young male adults and non-smokers. It has a good prognosis with chemoradiotherapy. It is still to be determined in the next several years by public health officials whether adolescent boys should be vaccinated against HPV, in comparison to young sexually active girls who are getting vaccinated [12]. There are different methods to detect human papilloma virus. For example, Nicolas F Schlecht, et al. and colleagues [13] had the highest estimates obtained for oropharyngeal tumors by in-situ hybridization using the Ventana Fam16 probe cocktail. However, other studies, such as Agoston, et al. [14] have reported higher detection rates in oropharyngeal tumors using in-situ hybridization with the Ventana Fam16 probe cocktail, and PCR using L1 and E7 DNA primers, but did not provide analogous estimates of test performance as comparisons were made to combined test results assuming no false positives [13].
On histopathology, branchial cleft cysts usually appear as a cyst with lining epithelia categorized into stratified epithelium without keratinization, columnar epithelium with or without cilia, or a mixture of both. In about 90% of cases branchial cleft cysts are usually lined by squamous epithelium. Two percent of cysts show both types of epithelium, squamous and columnar. On the other hand, 8% are made of ciliated columnar epithelium [15]. There is usually lymphoid tissue under the epithelium, commonly with germinal centers and subcapsular lymph sinuses. A branchial cleft cyst itself is usually encircled by lymphoid tissue also. It is common to have marked inflammatory changes and the epithelium superimposing the lymphoid tissue is attenuated or absent [16].
Treatment of branchial cleft cysts consists of antibiotics if there is active infection, with avoiding of incision and drainage as it might cause alteration of surgical planes. After resolution of the infection, full excision of the cyst is the gold standard management. Excision of a branchial cleft cyst by itself is not considered as an emergent procedure. Due to recurrent infections and the low risk of malignancy, it is usually done. However, emergent surgery may be required in case of airway compromise or large abscess [17, 18]. The incision is usually made within the line of a natural skin crease to make the wound look as cosmetic as possible. Recurrence is usually uncommon once branchial cleft cysts are excised. There is an approximated recurrence risk of 3%. However, recurrence can be as high as 20% if previous surgery or recurrent infection has occurred [19, 20].
Conclusion
Branchial cleft cyst is one of the most common causes of a lateral neck mass in children. However, in adults it is considered rare and a diagnosis of exclusion. It is a must to rule out malignancy in case of any new neck mass appearing in an adult. This case is important due to the limited literature done in adults with branchial cleft cysts, in addition to highlighting the correct sequence of management when detecting a lateral cervical swelling. Surgical management is the definite treatment for this condition with very minimal recurrence rate.
References
-
Agaton Bonilla FC, Gay Escoda C (1996) Diagnosis and treatment of branchial cleft cysts and fistulae. A retrospective study of 183 patients. Int J Oral Maxillofac Surg 25(6): 449-452.
-
Muller S, Aiken A, Magliocca K, Chen AY (2015) Second Branchial Cleft Cyst. Head Neck Pathol 9(3): 379-383.
-
Glosser JW, Pires CA, Feinberg SE (2003) Branchial cleft or cervical lymphoepithelial cysts: etiology and management. J Am Dent Assoc 134(1): 81-86.
-
Goff CJ, Allred C, Glade RS (2012) Current management of congenital branchial cleft cysts, sinuses, and fistulae. Curr Opin Otolaryngol Head Neck Surg 20(6): 533-539.
-
Kenealy JF, Torsiglieri AJ Jr, Tom LW (1990) Branchial cleft anomalies: a five-year retrospective review. Trans Pa Acad Ophthalmol Otolaryngol 42: 1022-1025.
-
Daoud FS (2005) Branchial cyst: an often forgotten diagnosis. Asian J Surg 28(3): 174-178.
-
Allen SB, Jamal Z, Goldman J (2021) Branchial Cleft Cysts. In: StatPearls.
-
Work WP (1972) Newer concepts of first branchial cleft defects. Laryngoscope 82(9): 1581-1593.
-
Bajaj Y, Ifeacho S, Tweedie D, Jephson CG, Albert DM, et al. (2011) Branchial anomalies in children. Int J Pediatr Otorhinolaryngol 75(8): 1020-1023.
-
Bailey H (1929) Branchial cysts and other essays on surgical subjects in the fascio-cervical region. BJS 17(66): 362.
-
Nicoucar K, Giger R, Pope HG Jr, Jaecklin T, Dulguerov P (2009) Management of congenital fourth branchial arch anomalies: a review and analysis of published cases. J Pediatr Surg 44(7): 1432-1439.
-
Moscicki AB (2008) HPV Vaccines: today and in the Future. J Adolesc Health 43(4): 26-40.
-
Schlecht NF, Brandwein Gensler M, Nuovo GJ, Li M, Dunne A, et al. (2011) A comparison of clinically utilized human papillomavirus detection methods in head and neck cancer. Mod Pathol 24(10): 1295-1305.
-
Agoston ES, Robinson SJ, Mehra KK, Birch C, Semmel D, et al. (2010) Polymerase chain reaction detection of HPV in squamous carcinoma of the oropharynx. Am J Clin Pathol 134(1): 36-41.
-
Prada LR, Koripalli VS, Merino CL, Fulger I (2017) A Case of a Rapidly Enlarging Neck Mass with Airway Compromise. J Clin Diagn Res 11(5): 14-16.
-
Schmidt K, Leal A, McGill T, Jacob R (2016) Rapidly enlarging neck mass in a neonate causing airway compromise. Proc (Bayl Univ Med Cent) 29(2): 183-184.
-
Prosser JD, Myer CM (2015) Branchial cleft anomalies and thymic cysts. Otolaryngol Clin North Am 48(1): 1-14.
-
Coste AH, Lofgren DH, Shermetaro C (2021) Branchial Cleft Cyst. In: StatPearls.
-
Zaifullah S, Yunus MR, See GB (2013) Diagnosis and treatment of branchial cleft anomalies in UKMMC: a 10-year retrospective study. Eur Arch Otorhinolaryngol 270(4): 1501-1506.
-
Nahata V (2016) Branchial Cleft Cyst. Indian J Dermatol 61(6): 701.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?