Bilateral Peritonsillar Abscess: A Rare Case Report
Peritonsillar abscess is one of the most common complication of acute tonsillitis. However, bilateral forms are rare. A peritonsillar abscess occurs when pus accumulates in the peritonsillar space, located between the tonsils and superior constrictor muscle. Diagnosis is usually based on clinical presentation and examination. Symptoms and findings generally include fever, sore throat, dysphagia, trismus, and muffled “hot potato” voice. It is considered as an emergency, as it could be complicated by an upper airway obstruction. Immediate diagnosis and urgent drainage are needed to avoid serious life-threatening situation.
Introduction
Peritonsillar abscess is a bacterial infection that usually begins as a complication of untreated acute tonsillitis, it develops outside the tonsillar capsule, mainly located in the region of the upper pole and involve the soft palate pushing the tonsils forwards and towards the uvula. Peritonsillar abscesses are the most prevailing deep neck infections.
Unilateral peritonsillar abscesses are very common, while bilateral peritonsillar abscesses are rare. The overall incidence of bilateral peritonsillar abscess is reported to reach 4.9% [1].
Patients usually presents with sore throat, odynophagia, dysphagia, otalgia, trismus, oral drooling, and fever. Diagnosing such cases might be challenging since bilateral peritonsillar abscess lacks the characteristic features of unilateral peritonsillar abscess [2].
Case Presentation
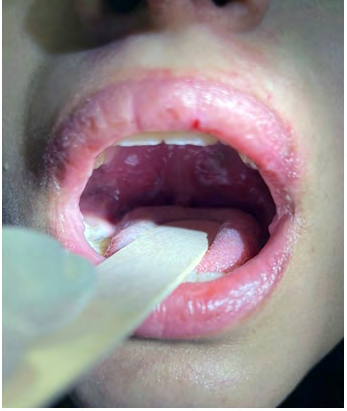
An 18 year old girl known case of asthma, was transferred to the Emergency Department with 5 days history of sore throat, difficulty in swallowing solid and liquid, multiple episodes of vomiting and fever. She was seen by primary care center where she received oral antibiotics (Augmentin 1 gm 12 hourly) and mouth gargles. Her symptoms worsened, then she was transferred to our hospital for further evaluation. On examination, high grade fever was documented (39°C), other parameters were within normal range, she had muffled voice without stridor. She also had limited mouth opening due to trismus. Examination of the oral cavity and oropharynx showed bilateral peritonsillar abscess and bulge follicular tonsillitis. Bilateral submandibular lymph nodes were palpable.
White blood count was 22.3, Neutrophils 17.3, other lab results were unremarkable, (COVID-19 test was negative). Needle aspiration followed by incision and drainage was done under local anesthesia. A 10cc pus drained from right peritonsillar abscess and 5 cc drained from left peritonsillar abscess. No radiological investigation was done as the diagnosis was clear.
She was admitted to the ward for intravenous fluids, intravenous antibiotics and analgesia. She had good recovery and discharged home after 2 days without any complications (Figures 1 & 2).

Discussion
Peritonsillar abscess is a collection of pus inside the peritonsillar space between the superior constrictor muscle and tonsillar capsule. Peritonsillar abscess is usually unilateral, however bilateral peritonsillar abscess is considered extremely rare. Bilateral peritonsillar abscess is considered an otolaryngologic emergency. The incidence reported in the literature concerning bilateral peritonsillar abscess is varied. The greater percentage involves cases of incidental contralateral abscess was found during tonsillectomy. The incidence of unsuspected contralateral peritonsillar abscess recognized at tonsillectomy has been reported to be between 1.9% and 24%, however the overall incidence of peritonsillar abscess is reported to reach 4.9% [1]. The majority of patients are reported among young adults aged 20–40-years old with a male-to-female ratio of 2:1, and seldom include children or infants [2]. The incidence of peritonsillar abscess in children is around 14 to 30 cases per 100.000 [3]. Marom T, et al. reported a changing trend of peritonsillar abscess occurring among older patients, which is associated with prolonged hospitalization and higher morbidity and mortality rates compared with children [4].
Progression of tonsillitis to bilateral peritonsillar abscess, is possibly due to an infection of both tonsils, depending on the evolution of the abscesses being different on each side. However, according to literature the patient’s systemic response to infection, antibiotics, or surgical intervention may interrupt the progression of this disease at any stage [1]. Up to this time, there are two hypotheses to explain the pathogenesis of peritonsillar abscess. The first is that peritonsillar abscess is a complication of acute bacterial tonsillitis. The second is that peritonsillar abscess is a minor salivary gland infection (Weber’s glands specifically) [3]. Peritonsillar abscess is a polymicrobial disease, which can be caused by aerobic organisms including Streptococcus pyogenes, Streptococcus viridans, Haemophilus influenza and anaerobic organisms including Fusobacterium and Bacteroides [1]. In addition to tonsillitis, other risk factors that could possibly be associated with peritonsillar abscess are smoking, which would cause a change in oral cavity flora and decreases oral immunity [2], also immunocompromised patients with poor oral hygiene which might cause dental infections [5], and infectious mononucleosis.
The diagnosis of peritonsillar abscess in general is based on history and physical examination. The appearance of bilateral peritonsillar abscess in the oral cavity, lacks the asymmetry and uvula deviation, that are usually presented in cases of unilateral peritonsillar abscess [1]. On the other hand, steroid and antibiotic treatment might conceal the signs and symptoms of peritonsillar abscess [1]. For that reason, bilateral peritonsillar abscess can be confused with other conditions, like bilateral lymphomas of the tonsils, infiltrating carcinomas of the soft palate or uvula, any tumors of the small salivary glands of the oral cavity, tonsillar cellulitis, or infectious mononucleosis [1]. Furthermore, in situations where the diagnosis is uncertain, imaging studies such as: CT scan with contrast must be considered to differentiate between bilateral peritonsillar abscess and other conditions [2] (Table 1).
| Laboratory Investigations | Radiological Investigations |
| Complete blood count (CBC) | X-ray of the neck |
| Pus culture/sensitivity from needle aspiration (gold standard) | CT with contrast |
| Monospot test (to rule out infectious mononucleosis) | Intraoral ultrasonography |
| Inflammatory markers (C-reactive protein) |
Table 1: Investigations to Diagnose Peritonsillar Abscess.
Our patient presented with bilateral symmetrical swelling and midline uvula. CT scan was not performed, since the diagnosis was confirmed by bilateral diagnostic needle aspiration. In such cases, needle aspiration is both a diagnostic and therapeutic procedure to confirm the diagnosis and relieve symptoms. Literature also suggested the diagnostic use of intraoral ultrasound in cooperative patients [2].
Although it is controversial on what is the definitive management of bilateral peritonsillar abscess, needle aspiration and incision and drainage are the ideal options along with intravenous antibiotics. Quinsy tonsillectomy may be indicated for patients who are not responding to intravenous antibiotic treatment, needle aspiration, and incision and drainage of peritonsillar abscess [6].
Needle aspiration is considered more preferable as it is a less invasive procedure and useful for culture specimen than incision and drainage, and the reported successful rate is 94% [7]. However, its more painful than incision and drainage. In our case, needle aspiration was done by using large- bore needles for culture specimen, then incision and drainage was used as the definitive management. Two incisions (1 cm each) were made on the lower arch of the abscess pockets, and hemostat instrument was used to spread the pocket to make sure the whole collection is drained. Then the patient treated with empirical intravenous antibiotic along with a single dose of corticosteroid to relieve the symptoms.
In the majority of cases, peritonsillar abscess is located superior to the tonsil. Once the abscess pocket is located, 1 cm long incision should be made through the area where needle aspiration was done into the palatoglossus muscle to enter the peritonsillar space, following the arch of the abscess pocket. It must be done carefully as the carotid artery lies 2-2.5 cm posterolateral to the tonsillar capsule.
Bilateral peritonsillar abscess can cause various life- threatening complications, if not treated promptly. Upper airway obstruction due to mucosal edema of the pharynx is one of the most common and critical complications and must be managed immediately. Progression of the infection may lead to retropharyngeal abscess, necrotizing fasciitis, mediastinitis, internal carotid artery lesion and brain abscess [8]. However, in unilateral peritonsillar abscess, the chance of developing such complications is quite low, compared to bilateral peritonsillar abscess, since the space occupied by the abscess in bilateral form is larger [9]. Moreover, there is increased risk of spread of infection to deeper neck compartments [9].
A retrospective study was done on 172 patients treated from peritonsillar abscess showed that the recurrence rate of peritonsillar abscess was 13.9% [10]. Recurrent tonsillitis with extra peritonsillar spread is considered a significant risk factor for recurrence [10].
Conclusion
This case delineates, the rareness of bilateral peritonsillar abscess, in addition to the difficulty of diagnosing such cases, due to the limited literature available and the intraoral appearance of bilateral peritonsillar abscess, which lacks the clinical features of unilateral peritonsillar abscess such as, deviated uvula and unilateral bulging. Bilateral peritonsillar abscess is considered an otolaryngologic emergency, which can cause airway obstruction leading to possible mortality. Early management leads to better outcome.
References
-
Papacharalampous GX, Vlastarakos PV, Kotsis G, Davilis D, Manolopoulos L (2011) Bilateral Peritonsillar Abscesses: A Case Presentation and Review of the Current Literature with regard to the Controversies in Diagnosis and Treatment. Case Reports in Medicine 2011: 981924.
-
AlAwadh I, Aldrees T, AlQaryan S, Alharethy S, AlShehri H (2017) Bilateral peritonsillar abscess: A case report and pertinent literature review. Int J Surg Case Rep 36: 34-37.
-
Arunathan R, Tan SN (2020) A Rare Case of Bilateral Peritonsillar Abscess in a Child: An Impending Deadly Condition. Anatol J Family Med 3(3): 267-269.
-
Marom T, Cinamon U, Itskoviz D, Roth Y (2010) Changing trends of peritonsillar abscess. Am J Otolaryngol 31(3): 162-167.
-
Hemail M Alsubaie, Maisa B Alsmadi, Eidah F Aljuaid (2020) Bilateral peritonsillar abscess: a case study and literature review. Journal of Surgical Case Reports 2020(8).
-
Johnson RF, Stewart MG, Wright CC (2003) An evidence- based review of the treatment of peritonsillar abscess. Otolaryngol Head Neck Surg 128(3): 332-343.
-
Herzon FS (1995) Harris P Mosher Award thesis. Peritonsillar abscess: incidence, current management practices, and a proposal for treatment guidelines. Laryngoscope 105: 1-17.
-
Klug TE, Greve T, Hentze M (2020) Complications of peritonsillar abscess. Ann Clin Microbiol Antimicrob 19: 32.
-
Boon C, Mohamad WE Wan, Mohammad I (2018) Bilateral peritonsillar abscess: A rare emergency. Malays Fam Physician 13(1): 41-44.
-
Chung J, Lee Y, Shin S, Eun Y (2014) Risk factors for recurrence of peritonsillar abscess. J Laryngol Otol 128(12): 1084-1088.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?