Classic Hodgkin Lymphoma with Unusual Cystic Lesions and Presentation in a 5-Year-Old Boy: A Case Report for Clinical Review and Management Approach
Hodgkin lymphomas are a group of malignant neoplasms affecting the lymphatic system. They account for approximately 6% of all childhood cancers. They display a bimodal age distribution with the first peak being in adolescents/young adults and the second peak being in older adults. The incidence and distribution of different Hodgkin lymphoma (HL) subtypes varies depending on socioeconomic factors, geography, family history, immune status and infections such as Epstein-Barr Virus (EBV). About 80% of children with HL present with lymphadenopathy. Other presentations include mediastinal masses on chest x-rays and patients presenting with B symptoms. This paper describes a case of classic Hodgkin Lymphoma (cHL) with unusual cystic lesions and presentation in a 5-year-old boy with a positive history of EBV infection.
Introduction
Hodgkin lymphomas are lymphoid neoplasms in which malignant cells are mixed with inflammatory cells [1, 2, 3, 4].
One of the leading suspects in the pathogenesis of Hodgkin lymphoma (HL) is Epstein Barr Virus (EBV). Some studies have discussed the possibility that childhood and adult HL may differ in their etiologies [5]. However, there is paucity of data available for the pediatric age group.
Common presenting symptoms and signs of HL in children include lymphadenopathy, mediastinal mass on chest x-ray (CXR), systemic symptoms such as fatigue, nausea, anorexia and fever. Patients may also present with hepatosplenomegaly [6]. Diagnosis of HL is established via imaging modalities such as Computed Tomography (CT) scans as well as using samples obtained through Fine Needle Aspiration (FNA) of enlarged lymph nodes and histopathology examination of excised lymph nodes [6].
Here, we discuss a challenging case of a 5-year-old boy with a history of EBV infection who presented with tender cervical lymphadenopathy that was later diagnosed as classic HL (cHL) with a literature review on childhood cHL.
Case Presentation
A 5-year-old boy with a past medical history of global developmental delay, microcephaly, epilepsy, blindness and a previous history of EBV infection presented with 11-day history of right neck swelling and a 1-day history of fever. There was no reported history of weight loss, night sweats, respiratory symptoms, recent travel, or contact with pets. According to his parents, the child’s immunizations were up to date. On admission, the vital signs were normal. On examination: a right sided cervical swelling was observed over the anterior and posterior triangles of the neck. The mass was tender to touch and consisted of a large number of smaller lumps. There was no generalized lymphadenopathy, organomegaly, rashes or scratch marks.
Initial laboratory investigations revealed lymphopenia and elevated inflammatory markers. Investigations for Adenovirus, Parvovirus, Human Herpesvirus, Cytomegalovirus, Diphtheria, Tetanus, Haemophilus Influenzae, Pneumococcus and Toxoplasmosis in blood were all negative. EBV IgG antibody was positive and EBV DNA was detected in blood (1340 copies/mL). T-spot test for Tuberculosis was non-reactive. An ultrasound was done which demonstrated right cervical and periauricular multiple heterogenous echogenic lesions with cystic components, the largest measuring 6.3x3.4cm with deranged architecture representing cystic and necrotic lymph nodes. Guided FNA of lymph nodes was suggestive of Granulomatous Lymphadenitis. Ziehl-Neelsen stain of the FNA cytology sample for Acid Fast Bacilli was non-contributary.
The impression at the time was suggestive of EBV reactivation and the patient remained in the hospital for symptomatic management. He stayed in the hospital for 2 weeks and was discharged but returned 2 days later with a continuous high-grade fever. The Otolaryngology (ENT) team was consulted and they recommended outpatient follow-up for excisional biopsy after the resolution of fever. The patient was discharged within a few days but presented back with the same complaints.
CT scan of the neck was done on the third admission which demonstrated a unilateral large cluster of homogenous non-necrotic nodal masses at the right side of the neck involving levels II, III, IV and V and extending down to the right supraclavicular regions and superiorly to the mastoid level. These radiological features were non-specific and could have been attributed to reactive adenopathy (infection, inflammation or granuloma) versus neoplastic growth (lymphoma). Excisional biopsy and histopathological correlation were highly advised (Figures 1 and 2).
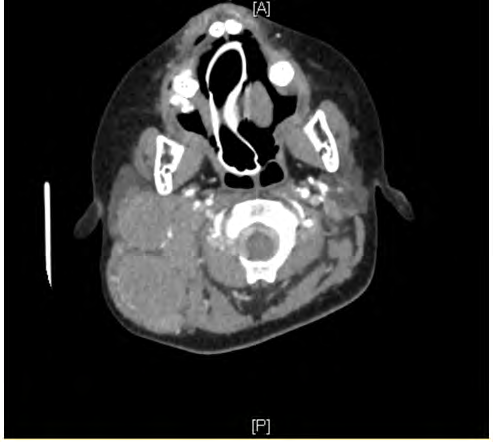
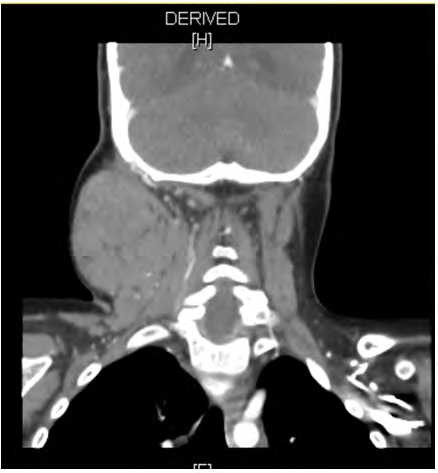
A second Fine needle aspiration revealed atypical cells, granuloma, histiocytic cells and reactive lymphoid cells possibly suggestive of lymphoreticular malignancy.
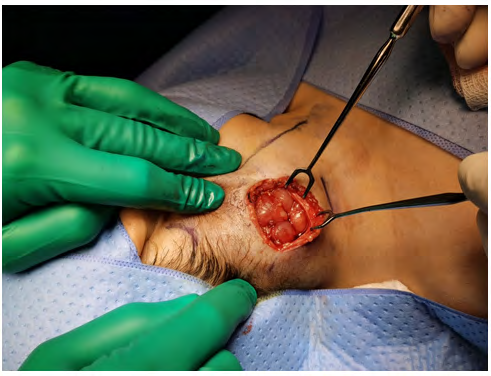
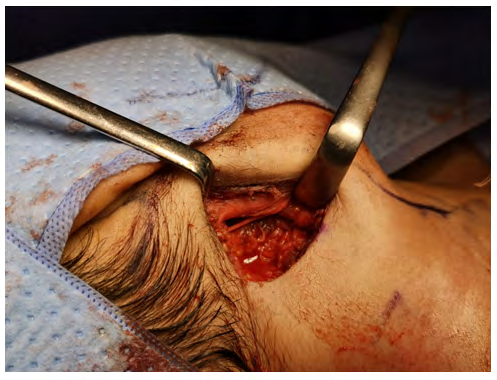
A decision was made to proceed with surgical intervention during which posterolateral neck dissection was performed at levels IIb, III, IV and Va. Under general anaesthesia, a transverse incision was made two fingers above the supraclavicular region from the anterior border of the sternocleidomastoid extending three centimetres to the back. Subplatysmal flap dissection revealed a large number of lymph nodes and excision was performed at levels IIb, III, IV and Va. Dissection reached the mylohyoid and accessory nerve inferiorly which was intact and posteriorly to the anterior border of the trapezoid muscle. Closure of skin was done in layers and a vacuum drain was placed (Figures 3 and 4).
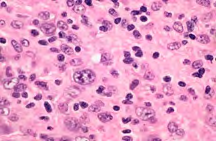
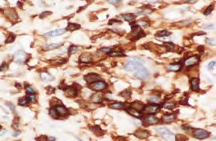
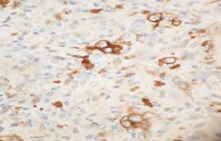
Histopathology examination of lymph nodes revealed classic Hodgkin Lymphoma (cHL) (Figures 5-7).
Discussion
Hodgkin lymphomas are lymphoid neoplasms in which malignant cells are mixed with a heterogeneous population of non-neoplastic inflammatory cells [4]. HL is characterised by mono-nucleated Hodgkin cells and bi-/multi-nucleated Reed-Sternberg cells [7]. The World Health Organization (WHO) classifies HL pathologically into cHL and nodular lymphocyte predominant HL [8]. The former is further subdivided into four subtypes, namely: nodular sclerosis HL (NSHL), mixed cellularity HL (MCHL), lymphocyte-rich HL (LRHL) and lymphocyte depleted HL (LDHL) [5].
Many risk factors for HL have been proposed. Indeed, these include a personal history of infectious mononucleosis (IM), immunocompromised states (such as HIV infection) and a family history of HL (in a parent or sibling) [9, 10, 11]. In fact, one study conducted in Sweden found ~28% heritability of HL in the population [11]. The same study has also demonstrated an independent association between high fetal growth and HL. In contrast, another study, which focused on the role of childhood social environment in the development of HL, suggested that early exposure to common infections may have a protective effect against HL, possibly by enhancing cellular immunity maturation (i.e., T helper 1/Th1-type immunity). This was demonstrated by a novel inverse association between nursery school/day care attendance and HL [7].
The implication of EBV in many head and neck cancers (including HL) has led to a possible link between the infectious agent and the disease. This association was hypothesized first in 1964; after detection of EBV in tumor cells from patients with Burkitt lymphoma [12]. A study in Peru demonstrated that patients with HL had an abnormally high levels of antibodies against EBV antigens [13].
Recently, up to half of classical HL cases in immunocompetent individuals were found to be associated with EBV [13]. Strikingly, a higher rate of EBV positivity was observed in children under 10 years old compared with other age groups [14]. There are two hypotheses that may explain the bimodal age incidence curve of HL (in developing and developed countries). It either reflects exposure to the same infectious agent at a different age (i.e., resembling ‘the polio model’ in the pre-vaccine era) or suggests different etiologies for pediatric and young-adult HL [14, 15].
Although there is little data regarding childhood HL, the role of EBV involvement in the pathogenesis of the disease is certain, especially in children under 10 years of age and particularly in the mixed cellularity subtype (MCHL) [14, 15]. Furthermore, four epidemiological varieties (Type I-IV) of HL have been described in the literature. Children characteristically belonged to Type I, which is found in developing countries with suboptimal socioeconomic conditions [16]. A preponderance of MCHL has been reported in Third World countries [13]. However, conclusions about many other aspects concerning pediatric HL could not be drawn (sometimes because the number of participants was too small).
EBV transmission is mainly through infected saliva (e.g., coughing, sharing food, kissing- hence the layman’s term ‘kissing disease’) and, less commonly via sexual activity [12, 17]. The virus amplifies by initiating the lytic phase after entering the Waldeyer tonsillar ring in the oropharynx [18]. Infected individuals may be contagious for up to 180 days (and even longer) according to one study [12]. It has been hypothesized that age at exposure to EBV may influence the severity of symptoms and risk of developing HL [12]. Interestingly, some studies found that primary EBV infection is more severe and more frequently associated with the syndrome of IM- a risk factor to HL- in adolescents [12, 15].
EBV and the Latent Infection Model
Approximately 50% of all 5-year-old children in developed countries have evidence of a previous EBV infection [17]. It is considered the most potent human virus that transforms in vivo and can persist in >90% of individuals [18]. Nevertheless, it causes disease in <10% of infected humans [17]. Additionally, young children usually have mild respiratory symptoms or have a subclinical course [17]. Primarily, it spreads by initiating a lytic phase resulting in the production of infectious virions which remain in saliva as a source of transmission or may infect other B cells [17]. Latent EBV infection has a predilection toward B lymphocytes. The virus induces tumor formation by modifying B-cell growth transcription factors (different patterns of EBV gene expression have been described; Latency I-III) [17]. Latency II results in the expression of latent membrane protein-1 (LMP-1) gene and seems to associate with both pediatric as well as adult HL [18]. The tumorigenesis of a latent EBV infection is thought to be explained by an underlying immune dysfunction related to Th1/Th2 imbalance [5]. This, in turn, leads to either an enhanced viral replication or a subtle and complex viral-host interaction [5, 15, 18]. Furthermore, two EBV strains (type A and B) have been described recently; with differences in their efficiency of transforming lymphocytes and the ease of maintaining these transformants in culture [15]. Epigenetic pathways or high levels of growth factors (such as insulin-like growth factor-I or IGF-1) may also contribute to the pathogenesis; by either augmenting the host sensitivity to the carcinogenic properties of the infectious agent or inhibiting apoptosis of the transforming/ transformed lymphocytes [11]. Histologically, although 4 subtypes of classic HL have been described, one hypothesis suggests that the disease progresses from one to the other in the following order: lymphocyte predominant–mixed cellularity–lymphocyte depleted–nodular sclerosis; the latter representing arrest of this progression and indicating an advanced stage of the disease (thus, poor prognosis) [16].
Even though rare, chronic active EBV (CAEBV) infection which mainly affects children, increases the likelihood of developing lymphoma and lymphoproliferative disorders as the infection progresses [4, 11]. It is more common in East Asia and the disease’s progression seems to vary depending on a balance of factors, with a more favourable prognosis in children [4, 12].
Lymphadenopathy may be divided into localized or widespread and, from another aspect, causes may be categorized into non-neoplastic and neoplastic [7]. Asymptomatic lymphadenopathy, most often in the cervical region, is the commonest presentation of HL [6]. It usually starts as a solitary node enlargement, then spreads to adjacent lymph nodes as the disease progresses [6]. Some patients will have accompanying systemic symptoms such as B symptoms (fever, night sweats, weight loss, fatigue) and pruritus [4, 6]. On examination, organomegaly may be evident as well. Incidental radiological findings (e.g., a mediastinal mass on CXR) may also be suggestive of HL [6]. Having said that, many conditions have similar clinical presentation that may mimic HL and vice versa [4, 12, 18]. In addition, atypical presentation may be encountered in individuals with an immunocompromised state (particularly, those in the extremes of a population). For instance, even when an enlarged node reaches a considerable size, it may be difficult to distinguish it macroscopically and clinically from neoplastic disorders [7]. Thus, a thorough history (including personal, sexual and family) with a high index of suspicion and attention to clinical examination findings (especially an unusual neck swelling or mass) are key parts of the diagnostic process and essential to avoid misdiagnosis leading to inappropriate treatment and possibly poor prognosis.
To reach a timely diagnosis of lymphoma, it is imperative to begin with a thorough history and clinical examination. Because of the similarity in presentations between benign and malignant lymphadenopathy, consideration of a wide array of differential diagnoses cannot be overemphasized. Imaging modalities aid in establishing the extent of the disease as well as guiding biopsy [4, 6]. CXR may reveal mediastinal masses [6]. CT scans aid in providing better view of enlarged lymph nodes and provide information on possible extra- nodal involvement [6]. Positron Emission Tomography (PET) scans are more sensitive at detecting diffuse disease and are more sensitive at detecting any bone marrow involvement [19, 20]. Samples obtained from lymph nodes via ultrasound guided or non-guided FNAC and through lymph node biopsy are crucial to rule-out lymphoma [4, 6].
The therapeutic approach to children who are diagnosed with lymphoma requires a multidisciplinary approach and is decided based on the staging and prognosis of the patient [4, 6, 9]. It involves the surgical excision of affected lymph nodes along with combination chemotherapy and radiation therapy [6].
Given the tumorigenic ability of EBV, preventive measures should be prioritized. There is an increasing interest in the development of a vaccine against EBV infection [12]. However, future research should focus on the identification of high-risk individuals at young ages, the costs, benefits (especially, in preventing EBV-related cancers) and side effects.
In our case, our patient presented with a history of tender cervical lymphadenopathy and persistent fever. While an excisional biopsy was advised, it was in fact delayed due to an initial impression of EBV reactivation as well as the hesitance of the surgical team to operate on a febrile patient. We believe that tailored algorithms (to target groups) can be utilized, in turn, to aid early diagnosis of HL where an overlap between diseases’ presentation occurs. Advanced testing, particularly in young children, may be necessary due to the complex pathogenic mechanisms of EBV in pediatric HL.
Conclusion
In summary, while classic Hodgkin Lymphoma remains one of the most common causes of malignancy in children, this case highlights an unusual presentation of extensive cervical lymphadenopathy with cystic and necrotic components extending through several levels of lymph nodes in the neck in a young child. This case emphasises the importance of a systematic approach in distinguishing benign and malignant lymphadenopathy as well as offering prompt management.
References
-
Altekruse SF, Kosary CL, Krapcho M, Neyman N, Aminou R, et al. SEER Cancer Statistics Review. 1975-2007. National Cancer Institute. Bethesda, MD.
-
Barista I, Varan A, Ozyar E (2007) Bimodal age distribution in hodgkin’s disease and nasopharyngeal carcinoma. Medical Hypotheses 68(6): 1421.
-
Bazzeh F, Rihani R, Howard S, Sultan I (2010) Comparing adult and pediatric Hodgkin lymphoma in the Surveillance, Epidemiology and End Results Program. 1988-2005: an analysis of 21 734 cases. Leuk Lymphoma 51(12): 2198-2207.
-
Bahethi R, Gray M, Salib C, Likhterov I (2020) Lymphoma Mimicking Chronic Active Epstein-Barr Virus: A Case Report. Head Neck Pathol 14(4): 1028-1031.
-
Chang ET, Zheng T, Weir EG, Borowitz M, Mann RB (2004) Childhood social environment and Hodgkin’s lymphoma: new findings from a population-based case- control study. Cancer Epidemiol Biomarkers Prev 13(8): 1361-1370.
-
Tina BM, McQueen S (2018) Essential Med Notes 2018: Comprehensive Medical Reference & Review for USMLE II and MCCQE, 34th (Edn.), Thieme, pp: 45-46.
-
James u, Cross S (2009) General and Systematic Pathology: With STUDENT CONSULT Access, 5th (Edn.), Churchill Livingstone, pp: 599-606.
-
Swerdlow SH, Campo E, Pileri SA, Harris NL, Stein H, et al. (2016) The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood 127(20): 2375-2390.
-
Ward E, DeSantis C, Robbins A, Kohler B, Jemal A (2014) Childhood and adolescent cancer statistics, 2014. CA Cancer J Clin 64(2): 83-103.
-
Hjalgrim H, Askling J, Rostgaard K, Hamilton Dutoit S, Frisch M, et al. (2003) Characteristics of Hodgkin’s Lymphoma after Infectious Mononucleosis. New England Journal of Medicine 349(14): 1324-1332.
-
Crump C, Sundquist K, Sieh W, Winkleby MA, Sundquist J (2012) Perinatal and family risk factors for Hodgkin lymphoma in childhood through young adulthood. American journal of epidemiology 176(12): 1147-1158.
-
Anders F, Lykkegaard CA (2019) Epstein-Barr virus and Its Association with Disease - a Review of Relevance to General Practice. BMC Family Practice 20(1): 62.
-
Chang KL, Albújar PF, Chen YY, Johnson RM, Weiss LM (1993) High prevalence of Epstein-Barr virus in the Reed-Sternberg cells of Hodgkin’s disease occurring in Peru. Bloodvol 81(2): 496-501.
-
Armstrong AA, Alexander FE, Paes RP, Morad NA, Gallagher A, et al. (1993) Association of Epstein-Barr virus with pediatric Hodgkin’s disease. The American journal of pathology 142(6): 1683-1688.
-
Ambinder RF, Browning PJ, Lorenzana I, Leventhal BG, Cosenza H, et al. (1993) Epstein-Barr virus and childhood Hodgkin’s disease in Honduras and the United States. Blood 81(2): 462-467.
-
Olweny CL, Katongole Mbidde E, Kiire C, Lwanga SK, Magrath I, et al. (1978) Childhood Hodgkin’s disease in Uganda: a ten year experience. Cancer 42(2): 787-792.
-
Binesh Marvasti Tina, McQueen S (2018) Pediatrics. Essential Med Notes 2018: Comprehensive Medical Reference & Review for USMLE II and MCCQE, 34th (Edn.), Thieme, pp: 52-53.
-
Tejaswi K, Khoory MS (2020) Infectious Mononucleosis Mimicking Epstein–Barr Virus Positive Diffuse Large B-Cell Lymphoma Not Otherwise Specified. International Journal of Hematologic Oncology 9(2): IJH25.
-
Robertson VL, Anderson CS, Keller FG, Halkar R, Goodman M, et al. (2011) Role of FDG-PET in the definition of involved-field radiation therapy and management for pediatric Hodgkin’s lymphoma. Int J Radiat Oncol Biol Phys 80(2): 324-332.
-
Sioka C (2013) The utility of FDG PET in diagnosis and follow-up of lymphoma in childhood. Eur J Pediatr 172(6): 733-738.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?