Open Rhinoplasty for Nasal Tip Correction by the Transverse Columellar Incision for Egyptian & Mediterranean Noses
Rhinoplasty may be the most common, most challenging, most unforgiving in plastic surgery. It is an ultimate combination of an evolving art and science. Rhinoplasty is a precise surgery in which the margin of error is measured in millimeters. Excellent results can only be obtained by a thorough knowledge of nasal anatomy and the surgical relevance of the alteration of the anatomic structures. To a lot of the Junior Staff, Rhinoplasty is a blind procedure requiring much imagination. This procedure has always been a challenge to the plastic surgeons. Objectives: Since the early eighties I had all the worry a young plastic surgeon has: standardizing his results for Aesthetic Rhinoplasty. Results were not always what one expected, and definitely tip correction was a great challenge. It was then I embarked adopting the open Columellar Incision. I am sharing with you my journey over 40 years and the results of believing and mastering a technique, preaching it in different arenas, and the final results achieved d not only nationally or regionally but also internationally when this technique is now universally accepted as a precise tool for better refinement. The indications limitations and the ghost of the scar are shown and proved to be over stated. In the millennium different strategies (suturing and grafting) have been adopted to obtain better aesthetic outcome and less functional disturbances, all these seem to go hand in had with the open rhinoplasty incision. Different indications are briefly gone through in this review and the long-lasting results are shown. Conclusions: Excellent symmetry, Lack of supratip deformity, particularly in Secondary and Tertiary Rhinoplasty The scar was inconspicuous in the healing phase, then in a few months it tended to migrate lower down and becomes almost invisible. The use of either grafts or various tip sutures can help in the control of the tip dynamics. The aesthetic outcome following a combination of suturing and grafting was more satisfactory than the outcome that can be achieved following either one of them. All these techniques could not be achieved through a closed endonasal rhinoplasty
Introduction
To a lot of the Junior Staff, Rhinoplasty is a blind procedure requiring much imagination. This procedure has always been a challenge to the plastic surgeons.
In early 80’s, I was an Assistant Professor at Kasr Alainy Faculty of medicine. I had all the worry a young plastic surgeon has standardizing his results for Aesthetic Rhinoplasty. Results were not always what one expected, and definitely tip correction was a great challenge. When I embarked adopting the open Columellar Incision. I was criticized and torn apart when I first presented the technique.
I published this article “Nasal Tip Correction by The Transverse Columellar Incision. Med. J. Cairo Univ., Vol. 54, No 2: 190-208, 1986”. Since then, I was preaching presenting my experience in different meetings and congresses, in the middle East and Europe.
“Open Rhinoplasty for Nasal Tip Correction by The Transverse Columellar Incision for Egyptian & Mediterranean Noses”; was very well received when presented in the Italian society of Plastic Surgery in Palermo, Italy 1998. A good part of their Tip Bulk being due to DERMOFAT rather than excess cartilage.
Excision of the former, and most important achieving symmetry by the endonasal route is always difficult. Furthermore, Internal Scarring and Synechiae are always, though rare a possibility difficult to avoid (Vogt, 1983).
The aim of a satisfactory rhinoplasty is a refined tip crowning the nose, endomucosal dissection preventing disturbance of the nasal physiology rather than mere reduction to fit nasal profile. We used the transverse columellar incision being a simple one and allowing good access and achieving good cosmetic results.
We used this technique for bulky tip with seborrheic thick skin, secondary and tertiary rhinoplasty, augmentation rhinoplasty with a rib, cleft lip noses, black skin patients, tip correction with excision of alae, correction of deviated septum with satisfactory results. The ghost of a visible scar is False even in the darkest patients. We do not recommend its indiscriminate use but we preserve it when the precise indication is present.
There were certain evolutional steps for Open Rhinoplasty progression; resection, scoring, morselizing, suturing, grafting naturally and synthetically and the overlap between them. In the 80s and 90s we used the suturing technique alone. In the beginning of the New Millennium, Autologous grafts combined with suturing techniques had become very popular. It has proved to be very efficient in reshaping and reconstructing of a new nose and preservation of nasal function internally and externally.
Open rhinoplasty obliges the surgeon to perform a detailed presurgical analysis of each patient, analyzing ethnic characteristics, skin thickness, cartilage strength, and nasal tip shape and position. This analysis helps the surgeon determine the patient’s nasal anatomy and the precise changes that should be performed surgically. The goal is to obtain a natural-looking result that is proportional to the patient’s face and aesthetically attractive as well as stable and durable over time.
Our analysis revealed that surgeons primarily learn Open Septorhinoplasty through residency training and didactic courses. Furthermore, younger surgeons perform open Rhinoplasty more frequently compared with older surgeons for all indications.
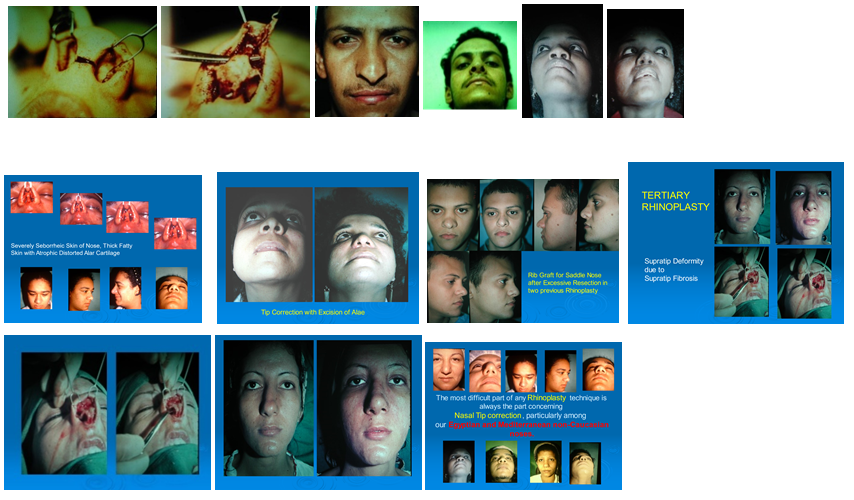
Open Septorhinoplasty provides an opportunity for greater surgical exposure for the operating surgeon and the assistants and thereby provides an excellent teaching tool. Results are Excellent concerning the degree of symmetry and lack of supratip deformity, particularly in Secondary and Tertiary Rhinoplasty. The scar was inconspicuous in the healing phase, and then in a few months it tended to migrate lower down and becomes almost invisible (Figure 1).
Conclusion
Open Septorhinoplasty has been embraced by facial plastic surgeons over the past 40 years in Kasr Al Ainy Hospital and throughout Egypt. It did not stop however a lot of animosity. It has been found useful for most indications except for the “simple” tip or dorsum. Its applications have had an upward trend, but it may now be reaching a plateau.
References
-
Mohamed K (1986) Nasal Tip Correction by The Transverse Columellar Incision. Med J Cairo Univ 54(2): 190-208.
-
Vogt T (1983) Tip Rhinoplastic Operations Using a Transverse Columellar Incision. Aesth Plast Surg 7(1): 13-19.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?